
Abstract
Background:
The pectoralis major (PM) is made up of multilaminar muscle segments that form a complex insertion on the proximal humerus; it is composed of an anterior and a posterior tendon layer. The tear patterns and patient characteristics of operatively treated PM ruptures in the general population remain poorly understood.
Purpose:
To comprehensively report the demographic characteristics of patients who are clinically diagnosed with structurally significant PM ruptures and to describe PM tear patterns identified during surgery.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective analysis of surgically treated PM tears was performed for a single-surgeon case series between January 1, 2003, and November 1, 2017. Patient demographic characteristics, classification of tear pattern, and treatment (repair/reconstruction) were recorded.
Results:
A total of 104 surgical cases of PM tendon rupture were identified; 100 patients underwent primary repair and 4 underwent dermal allograft reconstruction. All patients were male, with a mean age of 36.5 ± 9.2 years. Chronic tears (>6 weeks old) accounted for 63.6% of surgical cases, and 96% (n = 100) of tears occurred at or between the musculotendinous junction and tendinous insertion. A partial-thickness, complete-width tear of the posterior tendon layer at this same location was the most common tear pattern identified.
Conclusion:
PM ruptures occurred almost exclusively at or between the musculotendinous junction and tendinous insertion, with predominant involvement of the posterior tendon layer. Chronic tears can be safely treated with primary repair in the vast majority of cases.
Rupture of the pectoralis major (PM) was first reported by Patissier in 1822 in a French boy who was lifting a heavy piece of beef from a hook. 17 Although this type of injury fell into obscurity, the number of reported PM tears has dramatically increased over the past 25 years. We have also seen several new descriptions of surgical repair techniques for both acute and chronic ruptures. 3,6,7,22
Recent multicenter studies have outlined PM tear incidence, repair results, and complication rates among United States military personnel. 2,19 The question remains regarding how well the surgical and clinical characteristics of these reported cases can be extrapolated to a more general civilian population. Further, these studies have not routinely used a standardized descriptive classification of PM tears, adding ambiguity to the outcomes and complications reported.
The PM is made up of a uniform clavicular head and multisegmented sternal head that combine to form an insertion on the proximal humerus. It is composed of anterior and posterior tendon layers that do not twist or rotate at the level of the musculotendinous junction. 12 With this anatomic framework in mind, ElMaraghy and Devereaux 9 described a comprehensive classification system for PM tears that incorporates tear timing, location, and extent in terms of both thickness and width. This comprehensive standardized classification system for PM tears can be applied to a community population to help practitioners recognize and treat this rare clinical entity.
The goal of this study was to perform a retrospective analysis of a single community surgeon case series of structurally significant PM ruptures. With this new cohort of patients, we hoped to accurately describe the patient characteristics and classify the morphologic features of PM tears in a nonmilitary population and identify those tears that are amenable to primary versus grafted repair. We hypothesized that the majority of tear patterns will be partial thickness in nature, will involve the complete width of the posterior tendon layer, and will occur at or between the musculotendinous junction and tendinous insertion.
Methods
Patients
After approval was granted from our institutional research ethics review board, a retrospective chart review identified 110 patients referred to the senior author (A.W.E.) for treatment of a PM tear between January 1, 2003, and November 1, 2017. Inclusion criteria included patients older than 16 years with a primary clinical diagnosis of a structurally significant PM tear requiring surgical exploration and repair. A PM tendon tear was deemed structurally significant if the patient reported unacceptable levels of pain, deformity, or weakness and if physical examination revealed a positive Pectoralis Major Index. 10 Some patients had undergone imaging ordered elsewhere; further imaging was believed to be necessary only in some chronic cases with significant retraction, to determine whether enough extramuscular and/or intramuscular tendon collagen was present on the medial tissue, suggesting reparability. Even if believed to be reparable, very chronic tears with extensive medial retraction were considered for possible dermal allograft reconstruction if primary repair was not possible at the time of surgery. Patients were excluded from the study if they had previous shoulder girdle pathology noted on primary history and physical examination.
Clinical Data Collection
The patient demographic characteristics, injury date, and date of surgical consultation were recorded. Clinical data collected included injury mechanism, hand dominance, occupation, smoking history, and steroid use. Operative reports were reviewed, and the surgical date and surgical procedure performed (primary repair vs allograft reconstruction) were recorded. Based on information from the operative report, each tear was classified according to the comprehensive classification system previously described by ElMaraghy and Devereaux 9 (Figures 1 and 2, Table 1). Tears were considered chronic if surgical treatment was performed >6 weeks from the date of injury.
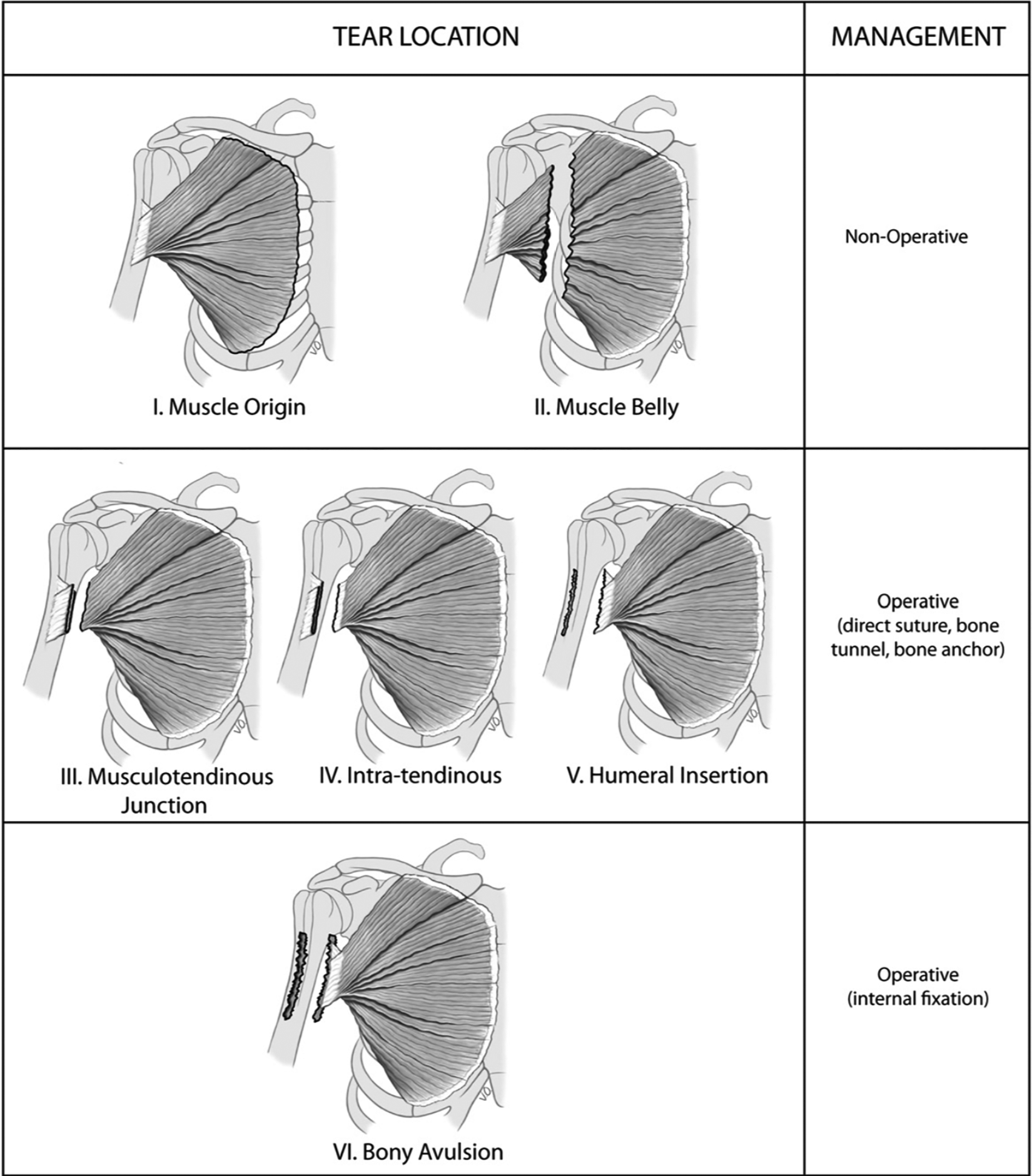
Possible locations of pectoralis major tears and associated management strategies. (Image reprinted with permission from ElMaraghy AW, Devereaux MW. A systematic review and comprehensive classification of pectoralis major tears. J Shoulder Elbow Surg. 2012;21(3):412-422. ©2012, Elsevier Ltd.)

(A) Tear extent is assessed by its width in a proximal-to-distal direction and its thickness in an anterior-to-posterior direction. AT, anterior tendon layer; PT posterior tendon layer. (B) Tear patterns (dark line) can affect 1 or both layers of the bilaminar tendon (eg, thickness) and can be complete or incomplete in width. (Image reprinted with permission from ElMaraghy AW, Devereaux MW. A systematic review and comprehensive classification of pectoralis major tears. J Shoulder Elbow Surg. 2012;21(3):412-422. ©2012, Elsevier Ltd.)
Comprehensive Classification System for Pectoralis Major Tendon Tears a

a Classification system by ElMaraghy and Devereaux. 9
Surgical Technique
With the patient in the beach-chair position, a vertical incision was made just superior to the axillary fold and roughly halfway between the humeral insertion and the torn and retracted PM fibers. The fascia was incised vertically and preserved for closure at the completion of the repair. The deltopectoral interval was identified first, then the PM muscle fibers of the clavicular head and upper sternal head segments were followed laterally toward their normal contribution to the anterior tendon layer insertion, and their integrity and/or the location and extent of the partial-thickness tear were identified. Next, the muscle fibers of the lower sternal head segments were followed laterally toward their normal contribution to the posterior tendon layer insertion, and their integrity and/or the location and extent of the partial-thickness tear were identified. If no continuity of any muscle segments could be identified, the location of the full-thickness tear was identified.
Especially in the chronic setting, accurate tear classification can be difficult owing to scarring and tendon retraction, which results in blurring of the usual tissue planes. To accurately classify each tear, 3 steps were followed. First, any intact fibers tracking toward the anatomic insertion of the PM tendon lateral to the bicipital groove were identified, keeping in mind their direction. Fibers coursing in an inferolateral direction contribute to the anterior tendon layer, whereas fibers coursing in a superolateral direction contribute to the posterior tendon layer. Although the visible external tendon of the PM is quite short, our previous anatomic study 12 found that the total length of the external and intramuscular internal tendon averaged 5.4 cm from the humeral insertion, and any tear within this zone was classified as being in location 2. Second, any intact fibers at the level of the insertion were then pinched in an anteroposterior direction. Each tendon layer is approximately 2 mm thick; therefore, anything <4 mm strongly suggests a partial-thickness tear. Finally, the width (craniocaudal extent) of each tendon layer attachment was examined. Considering that the normal width of each tendon layer is approximately 4 cm, tears were classified as complete or incomplete in width. In this way, the tear location and extent in terms of both thickness and width were systematically identified intraoperatively.
After identification of the torn tendon, a circumferential mobilization was performed, ensuring that the dissection stayed superficial to the conjoint tendon and pectoralis minor. After the release, if the residual visible and intramuscular tendon tissue was of adequate quality and could be brought to the native insertion site, a primary repair was performed. Depending on the extent of the tear, each tendon repair was accomplished using four to six No. 2 FiberWire (Arthrex) sutures with tapered needles attached to each end. Each suture end was woven through the tendon in a tissue-grasping, Krackow-type fashion, working sequentially from medial to lateral and cranial to caudal. One limb from each No. 2 FiberWire suture was loaded into a unicortical titanium anchor (Pec Button, 2.6 × 10.9 mm; Arthrex). Two suture limbs were loaded per Pec Button, and repairs therefore used 2 or 3 Pec Buttons depending on tear severity. After preparation of the native tendon insertion with a Howarth elevator to expose scored cortical bone, 3.2-mm unicortical drill holes were made, and each Pec Button was introduced into the intramedullary canal via a dedicated inserter and deployed (flipped). Each button limb of a suture pair was then sequentially tensioned to reapproximate the torn PM tendon to the prepared bony bed. Tension and apposition were maintained in all sutures by assistants while the last pair was tied by use of simple surgeon’s knots. A layered closure followed.
A specific standard rehabilitation protocol was instituted postoperatively (see Appendix 1, available as supplemental material). A modified rehabilitation protocol was used for chronic primary repairs that were tight after repair and did not comfortably allow 30° of passive external rotation on the operating table, as well as for chronic reconstructions with dermal allograft (see Appendix 2, available as supplemental material). A dermal allograft was believed to be necessary for chronic reconstruction when primary repair was not possible without excessive tension. If we could not comfortably reduce healthy tissue to its native insertion site (defined as the inability to reduce the tear in at least 30° of abduction and neutral rotation of the humerus), a previously described reconstruction technique using a dermal allograft was performed. 6
In cases treated before the advent of the Pec Button (in 2013), threaded bioabsorbable suture anchors were used. A similar final construct was used that entailed 2 high-strength No. 2 braided nonabsorbable sutures per anchor or fixation point.
Statistical Analysis
Descriptive statistics used to describe the data included mean and standard deviation for continuous measures and frequency and percentage for categorical variables. All statistical analyses were performed using SPSS Statistics Version 20.0 (IBM Corp).
Results
Clinical Characteristics
A total of 110 patients met the inclusion criteria for the study, of whom 104 wished to have a surgical repair or reconstruction of their PM tendon. Baseline demographic characteristics of the 110 included patients are presented in Table 2. The mean age at referral was 36.5 ± 9.2 years, and the age range was 16 to 71 years. All patients were male. Mechanism of injury was classified into 5 categories; the most common category was bench press or a similar weight-training exercise with the arms in an abducted and externally rotated position, representing 53.6% of cases. PM tears occurred almost equally on the dominant and nondominant extremity, at 46.4% and 49.1%, respectively. The majority of patients performed sedentary work (47.3%), although personal trainers, police officers, and laborers made up a significant proportion of the study population at 14.5%, 13.6%, and 11.8%, respectively. Tobacco use and anabolic steroid use were recorded in the study population at 10.9% and 9.1% of patients, respectively.
Demographic Characteristics of the Study Population (N = 110)

Operative Characteristics
The majority of PM tears encountered were chronic (63.6%). The majority of the chronic tears, however, had tissue quality receptive to secure suture purchase and enough mobility after release to facilitate a primary repair. Only 4 of the 70 chronic cases required tendon reconstruction with dermal allograft. The intraoperative findings observed for the 104 patients who had surgery are described in Tables 3 and 4. Both chronic and acute tears were most commonly classified as occurring in location 2 (at or between the musculotendinous junction and tendinous insertion), and entailed partial-thickness, complete-width involvement of the posterior tendon layer.
Operative Characteristics of the Study Population (n = 104)

Tear Patterns of the Study Population (n = 104)

Of the 4 patients who needed reconstruction with dermal allograft, all had chronic, location 2 tears. Two were partial-thickness, complete-width tears of the posterior tendon layer, and the remaining 2 were full-thickness, complete-width tears. Of these 4 cases, 1 was a revision repair for a traumatic rerupture; the primary repair was performed at an outside hospital from which records could not be obtained. One case was so chronic and medially retracted that primary repair could not be achieved without excessive adduction or internal rotation of the humerus. Furthermore, 2 additional reconstructions were performed for patients whose primary injury was an open major traumatic workplace-related injury with tissue loss.
Discussion
This single-surgeon case series confirmed the study hypothesis that in a community nonmilitary population, in both acute and chronic settings, PM tears occurred primarily at or between the musculotendinous junction and tendinous insertion and most commonly involved the posterior tendon layer. Furthermore, with only 4 of the 70 chronic cases requiring surgical reconstruction, this study reaffirmed that primary repair is a viable option for the majority of patients, regardless of chronicity. This is of particular clinical significance given the favorable results regarding strength and overall patient satisfaction with operative (versus nonoperative) treatment of PM tears that was demonstrated in previous studies. 1,4,5,21,23,24 Although chronicity certainly makes surgical repair technically more challenging, its overall impact on final clinical outcome remains controversial. Bak et al, 1 in a meta-analysis, recommended surgical repair within 8 weeks of injury, citing a higher likelihood of excellent results. Multiple studies, however, have shown no difference in terms of rerupture rate and return to activity and either minimal or no difference in strength or peak torque when comparing acute and chronic repairs. 5,13,19,23 The definition of a chronic tear varies from 3 to 8 weeks across studies. 4,13 We continue to use 6 weeks as the definition of chronic tear, given the clinical experience of the senior author and the added surgical releases necessary for these tears after this time point. Further, 6 weeks has been used to define chronic PM tears by other authors and chronic tears of other tendons across the body. 11,14,16,20,28
The strength of this case series lies in its size and the involvement of a single surgeon, which helps ensure accurate tear classification given the senior author’s significant experience treating PM ruptures. Recently, Balazs et al 2 and Nute et al 19 published a large case cohort and a case series of 291 and 257 patients, respectively. These studies, however, described the incidence, risk factors, and operative results exclusively in military personnel across a multitude of centers. In contrast, the current study documents findings in a nonmilitary population and was performed in a community-based teaching hospital. The study findings are more likely to be representative of structurally significant PM injury in the general public, with respect to demographic factors such as age, activity levels, and mechanism of injury, and therefore should be more widely applicable to most surgeons’ practices. We included all structurally significant ruptures in our case series, to highlight that only 6 of 110 patients chose nonoperative treatment. This is an important finding and illustrates that the desire to improve axillary contour and pectoralis strength with surgical treatment is shared by individuals in the military and civilian populations.
In comparison with existing literature, the current study used a more comprehensive classification system to describe the morphologic features of PM tendon ruptures. The most commonly used classification, by Tietjen, 25 does not account for the bilaminar tendinous insertion of the PM and therefore describes partial-thickness tears, particularly, in poor detail. The comprehensive classification system used in the current study details the timing, location, and extent (thickness and width) of PM tears and can be reproduced systematically by other surgeons at the time of surgical exploration and repair. 9 Taking these factors into account may provide insight into PM tear propagation.
In the current study, among location 2 tears, only a single partial-thickness tear involved the anterior tendon layer in isolation. Upon exclusion of full-thickness, complete-width tears, the most common pattern among both acute and chronic tears was complete-width rupture of the posterior tendon layer, accounting for 34.6% of all tears. Among location 2 ruptures, partial-thickness, incomplete-width tears of the posterior tendon layer were also commonly encountered in the chronic setting, but only 4 of such tears were noted acutely. It is likely that in the acute setting, such a tear pattern is less symptomatic and/or visually obvious and is considered a minor injury by patients, making them less likely to seek immediate medical attention. With time, however, the structural significance of this tear pattern becomes more evident. The posterior tendon layer is made up of the lower sternal head segment muscle fibers (Figure 3), which represent roughly 40% (or about half of the overall sternal head at 81%) of the total PM muscle volume. Furthermore, these lower sternal head muscle segments are most often targeted and therefore hypertrophied with common chest strengthening exercises. 12 Therefore, it is not surprising that even an injury exclusive to the posterior tendon layer muscles often results in appreciable deformity, weakness, and discomfort.

(A) Inferior continuity of the anterior tendon (AT) and posterior tendon (PT) layers distally. (B) The most inferior 2-3 segments of the sternal head (s5-s7) contribute to the PT layer. (Image reprinted with permission from ElMaraghy AW, Devereaux MW. A systematic review and comprehensive classification of pectoralis major tears. J Shoulder Elbow Surg. 2012;21(3):412-422. ©2012, Elsevier Ltd.)
With respect to tear morphologic features, the findings of the current study reflect the findings of earlier studies. 9,18,19 Although using different classification systems than that of the current study, both Nute et al 19 and Mooeres et al, 18 in their respective case series, reported that nearly all partial-thickness PM tendon tears involved either incomplete or complete rupture of the sternal head at the level of the musculotendinous junction. This is consistent with a location 2 involvement of the posterior tendon layer. 18,19
With regard to PM ruptures requiring allograft reconstruction, this study identified only 4 such cases. As previously mentioned, 1 case was a revision repair and 2 cases were major open traumatic ruptures with tissue loss. The average time from injury to surgery was >2 years. Furthermore, 3 of the patients requiring reconstruction were steroid users and smokers. This case series was not designed to identify preoperative factors that dictate the necessity for allograft reconstruction; however, when a patient has a history of very remote PM injury, visibly excessive medial retraction, or major open trauma with possible tissue loss or has undergone revision PM repair, the treating surgeon should consider the possibility that reconstruction may be necessary. We suggest obtaining magnetic resonance images to confirm that there is enough intramuscular collagen in the medial tissue to allow for suture purchase at the medial graft-host junction.
Taken in conjunction with the findings of previous anatomic and biomechanical studies, the current study supports the theory that tearing of the PM tendon initially occurs distally at the most inferior sternal head segments of the posterior tendon layer before moving proximally to involve the entire sternal head. 12,21,28 Electromyographic (EMG) studies conducted during the bench-press maneuver have shown that peak activity in the PM tendon occurs at the initiation of the lift, when the humerus is in extension. 8 It is in this position that the muscle fibers originating from ribs 5 and 6, which correspond to the most caudal fibers of the posterior tendon sheath (sternal head), are disproportionally stretched relative to their resting fiber length when compared with muscle fibers in more cephalad portions of the tendon. 12,28 Further EMG studies have shown that during the bench-press maneuver with heavier weights and in the setting of fatigue secondary to increased repetitions, PM recruitment further increases at the so-called sticking point of the lift, in an effort to successfully complete the lift. 26,27 The sticking point corresponds to the instant at which the upward barbell velocity decelerates or even stops completely for a period of time; this frequently occurs when the humerus is extended at the bottom of the lift. 8,15,26 At this point in time of maximal muscle recruitment, the muscle fibers of the caudal portion of the posterior tendon layer are at their greatest mechanical disadvantage because of arm position and inherent lateral pennation angle. 12 A PM tear is most likely to occur at this time, propagating in a caudal-to-cranial direction though the entirety of the posterior tendon layer. 28 If enough force is present, rupture of the anterior tendon layer corresponding to the clavicular head then occurs, culminating in a full-thickness, complete-width PM tear. The detailed tear patterns reported in the current study provide the most convincing evidence supporting the above theory of tear propagation.
A weakness of the current study is the retrospective design aiming to investigate demographic characteristics and tear morphologic features as well as the lack of clinical results. Documented measurements of peak torque, overall patient satisfaction according to the Bak et al 1 criteria, and, most important, rates of return to preinjury activity would be of particular value in chronic cases of PM tear. Furthermore, a small percentage of patient records had incomplete reporting of demographic characteristics, limiting complete assessment of both tobacco use and steroid use in this population.
The current clinical results reflect the findings of a single surgeon who has considerable experience with PM tendon repair and reconstruction in a community teaching hospital. Despite the increased number of cases reported in the recent literature, PM ruptures remain relatively rare. The high incidence of chronic tears in the current study also emphasizes the need for clinicians to maintain a high index of clinical suspicion for these injuries, and clinicians are advised to use the Pectoralis Major Index to rapidly identify structurally significant PM tears. 10 This can potentially eliminate the delay in surgical management that results from obtaining confirmatory imaging and thus allow for a technically easier, more acute repair to be performed, especially if the patient requires referral. Future studies evaluating and validating this comprehensive classification system for PM tears must be prospective in nature and include long-term follow-up of clinical and patient-reported outcomes. Patient results should be measured both qualitatively and quantitatively, as mentioned above. Furthermore, we acknowledge that although the classification system described by ElMaraghy and Devereaux 9 is comprehensive, it is not widely used. With continued uptake and use of this classification system to accurately describe the morphologic features of PM tendon ruptures, future studies will be able to make the necessary meaningful comparisons between techniques, outcomes, and tear patterns.
Conclusion
In a general, nonmilitary population, the majority of PM tendon tears were partial thickness in nature, they chiefly involved rupture of the posterior tendon layer, and they occurred at or between the musculotendinous junction and tendinous insertion. Chronic tears are common but can be safely treated with primary repair in the vast majority of cases with meticulous surgical technique and a thorough understanding of the surrounding anatomic characteristics.
Supplemental Material
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/2325967120969424
Supplemental Material
Supplemental Material, Appendix_1_-_Pec_Major_Rehab_Protocol - Pectoralis Major Ruptures: Tear Patterns and Patient Demographic Characteristics
Supplemental Material, Appendix_1_-_Pec_Major_Rehab_Protocol for Pectoralis Major Ruptures: Tear Patterns and Patient Demographic Characteristics by Marcin Kowalczuk, Luc Rubinger and Amr W. Elmaraghy in Orthopaedic Journal of Sports Medicine
Supplemental Material
Supplemental Material, Appendix_2_-_Modified_Pec_Major_Rehab_Protocol - Pectoralis Major Ruptures: Tear Patterns and Patient Demographic Characteristics
Supplemental Material, Appendix_2_-_Modified_Pec_Major_Rehab_Protocol for Pectoralis Major Ruptures: Tear Patterns and Patient Demographic Characteristics by Marcin Kowalczuk, Luc Rubinger and Amr W. Elmaraghy in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted May 19, 2020; accepted June 11, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.W.E. has received consulting fees and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from St Joseph’s Health Centre (study No. 2005-014).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.