
Abstract
Background:
Pectoralis major (PM) tendon tears are common injuries in athletic patient populations, where operative repair is largely recommended for maximum functional recovery. The repair varies in difficulty and technique based on the location of the tear within the muscle-tendon unit. Magnetic resonance imagining (MRI) has been reported to be sensitive and specific for identifying the tear location, but the effect of injury mechanism on tear pattern has not been previously investigated.
Purpose:
To examine PM tears in a military patient population and assess the effect of injury mechanism (weightlifting vs high-energy trauma) on the tear pattern and accuracy of MRI interpretation.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Active duty military servicemembers undergoing operative repair of PM tendon tears with corresponding preoperative MRIs from 2 medical centers were identified. Two musculoskeletal fellowship–trained radiologists reviewed imaging studies, reporting the location of the tear within the muscle-tendon unit and the severity of the tear (sternal head vs clavicular head vs both). Radiographic findings were compared against intraoperative findings. Mechanism of injury and timing from injury to imaging and surgery were assessed to determine whether they affected the accuracy of MRI interpretations.
Results:
A total of 72 patients were included (mean ± SD age, 33.7 ± 7.0 years; 100% male). Mechanisms of injury consisted of 46 weightlifting injuries and 26 high-energy injuries. Interrater reliability was poor for tear location (kappa, 0.162; P = .003) but substantial for extent of tear (kappa, 0.637; P < .0001). MRI had a 51.3% sensitivity and 63.6% specificity for identifying complete tears. MRI had a sensitivity of 73.9% and specificity of 72.2% for avulsion injuries and sensitivity of 75% and specificity of 79.3% for musculotendinous injuries. Mechanism of injury had no effect on extent of the tear but did affect the location of the tear, with a higher rate of avulsion injuries in the high-energy mechanism cohort (81% vs 40%; P = .02).
Conclusion:
The mechanism of injury was found to significantly affect the location of tendon tears. A higher rate of avulsion injuries was found in high-energy injuries than weightlifting injuries. MRI appeared to be less sensitive and specific than previous reports for traumatic PM tendon injuries.
Pectoralis major (PM) tendon rupture is a relatively uncommon injury that affects predominantly young healthy males engaging in sports or recreational weightlifting. 1,5,11,14,15,22 In recent years, the prevalence of reported cases has increased dramatically. 10 Military servicemembers are a specific population disproportionately affected by this injury, primarily affecting junior enlisted and officer personnel. 3
Magnetic resonance imaging (MRI) has emerged as the preferred study for the evaluation of PM tendon tears. 6,18,19,21,23 Several studies have evaluated the ability of MRI to distinguish the extent and severity of tendon tears. 2,6 –8,21 The sensitivity of MRI for identifying PM tendon tears has been reported to range from 67% to 100%, varying according to the acuity of the injury, the location of the tear, and the extent of the heads of the PM involved. 6,7
The vast majority of the literature for PM tendon tears has focused on indirect, or eccentric loading, injuries associated with activities such as weightlifting or sports. 2,12,13,15,21,23 A unique characteristic of the military population is that a considerable number of high-energy traumatic injuries precipitate PM tears. 17 Soldiers are susceptible to both eccentric loading activities such as bench press and direct, high-energy mechanisms such as traction injury sustained when their arm gets caught in the static line while they jump out of an airplane during airborne parachute operations. To date, no study has examined the utility of MRI for evaluating the extent or location of PM tendon tear in a patient population with a high rate of direct, high-energy traumatic injuries or the influence, if any, of mechanism of injury on MRI sensitivity and specificity of PM tears.
The purpose of this study was to examine PM tears in an athletic patient population of active duty servicemembers and assess the effect of injury mechanism on tear pattern by comparing accuracy of MRI interpretation to intraoperative findings. We hypothesized that MRI accuracy and sensitivity for evaluating PM tendon tears in this unique patient cohort would differ based on mechanism of injury.
Methods
After approval was granted from the institutional review board, a retrospective review was performed of all patients undergoing PM tendon repairs at 2 institutions over a 5-year period (February 1, 2012, to August 1, 2017). Patients were considered for study inclusion if they (1) had a PM tendon repair or reconstruction, (2) were active duty military servicemembers, (3) were older than 18 years of age, and (4) underwent a preoperative MRI study to evaluate injury. Patients were excluded if they did not have an operative report confirming the repair details of the PM tendon or if they did not have adequate MRI series available for review.
The medical records of patients who met the inclusion criteria were reviewed in order to gather demographic (sex, age at time of injury) and injury information (date of injury, mechanism of injury). Mechanisms of injury were further segregated as either having an eccentric load during weightlifting or being a high-energy injury. Operative reports were obtained and reviewed to identify anatomic location of the tear, defined as either musculotendinous, intratendinous, or avulsion (with or without osseous avulsion). The extent of tear was also reviewed, defined as involving the sternal head, the clavicular head, or both.
MRI studies were reviewed to quantify the timing of the study relative to the date of injury as well as to characterize the imaging protocol (chest, shoulder, or pectoralis), strength of the magnet (measured in Tesla units), and slice thickness (measured in millimeters). Studies underwent independent review by 2 musculoskeletal fellowship–trained radiologists (A.M.W., M.C.) to characterize location of tear (musculotendinous, intratendinous, or avulsion) and extent of tear (involving the sternal head, clavicular head, or both).
Statistical Analysis
Statistical analysis was performed with the SPSS statistical package (Version 24; SPSS Inc). Significance was set at P < .05. Descriptive statistics were calculated. Interrater reliability was quantified with the kappa statistic for both location of tear and extent of tear. The operative findings for both location and extent of tear were used as the gold standard for comparison to assess the accuracy of radiographic assessment. Univariate analyses of variance were used to determine the effect of mechanism of injury and acuity of MRI study from time of injury and time until surgery on the accuracy for location and extent of PM tendon tears. Chi-square analysis was used for dichotomous variables. Pearson correlations coefficients were used to identify associations between continuous variables.
Results
Review of the operative database identified 79 patients who were reported to have undergone a PM tendon repair. Of these, 1 patient underwent a latissimus dorsi repair and not a PM repair, and 6 patients did not have an MRI scan available for review, leaving a total of 72 patients (mean ± SD age, 33.7 ± 7.0 years; 100% male). Mechanisms of injury consisted of 46 weightlifting injuries, 24 static line injuries sustained during parachuting training, and 2 traumatic injuries (1 fall during military training, 1 motor vehicle rollover).
The 72 patients underwent MRI assessment within 28.5 ± 76.9 days (range, 0-577 days) from the day of injury, and operative repair was performed 33.7 ± 101.15 days (range, 2-725 days) from the day of injury. The majority of patients underwent a PM-specific imaging protocol (69/72 with 3 chest or humerus studies) with 3.0-T magnets (3.0-T, n = 58; 1.5-T, n = 9; unknown, n = 5). MRI interpretation for tear location and extent of involvement is summarized in Table 1. Interrater reliability for tear location was poor (kappa, 0.162; P = .003); however, extent of tear showed substantial agreement (kappa, 0.637; P < .0001).
Location and Extent of Pectoralis Major Tendon Tears Found Upon Magnetic Resonance Imaging (MRI) and Clinical Evaluation a

a Values are numbers of injuries.
Operative reports were available for review in 67 cases (93%). Of these 67 operative reports, detailed tear characteristic information was not uniformly reported. Information pertaining to tear location was available for 51 patients (76.1%; 70.8% of the overall cohort) and extent of tear was provided in 59 patients (88%; 82% of the overall cohort) (Table 1). MRI had 51.3% sensitivity and 63.6% specificity for identifying complete tears.
The majority of PM tears, defined by clinical assessment and MRI, were located at either the musculotendinous junction or tendinous avulsions with a mix between isolated sternal head tears or both tendons. No cases of isolated clavicular head tears were noted. For avulsion injuries, MRI had a sensitivity of 73.9% and specificity of 72.2%, whereas for musculotendinous injuries, MRI had a sensitivity of 75% and specificity of 79.3%. Mechanism of injury had no effect on extent of tear but did affect the location of tear, with a higher rate of avulsion injuries in the high-energy mechanism cohort (81% vs 40%; P = .02).
Overall correlation for MRI interpretation of tear extent compared with clinical findings at the time of surgery was not significantly different for either rater (rater 1, correlation coefficient [CC] = –0.259 [P = .103]; rater 2, CC = 0.143 [P = .371]). When assessing location of tear, rater 1 reported findings that were significantly different from intraoperative findings (CC = 0.267; P = .041); however, no difference was found for rater 2 (CC = 0.145; P = .272).
A subanalysis was performed to assess whether the location of the PM tear affected the accuracy of MRI readings. For the 23 patients with avulsion injuries with corresponding MRI data, MRI interpretation demonstrated a 73.9% accuracy rate (n = 17). For the 12 patients with clinical musculotendinous injuries with corresponding MRI data, the accuracy rate for MRI interpretation was 75% (n = 9). Mechanism of injury was found to have no significant effect on extent of tear (sternal vs both heads; P = .503); however, location of tear was significantly different, with a higher rate of avulsion injuries in the high-energy mechanism cohort (81% vs 40%; P = .02) (Table 2).
Location and Extent of Pectoralis Major Tendon Tears Found During Clinical Evaluation, Listed According to Mechanism of Injury a
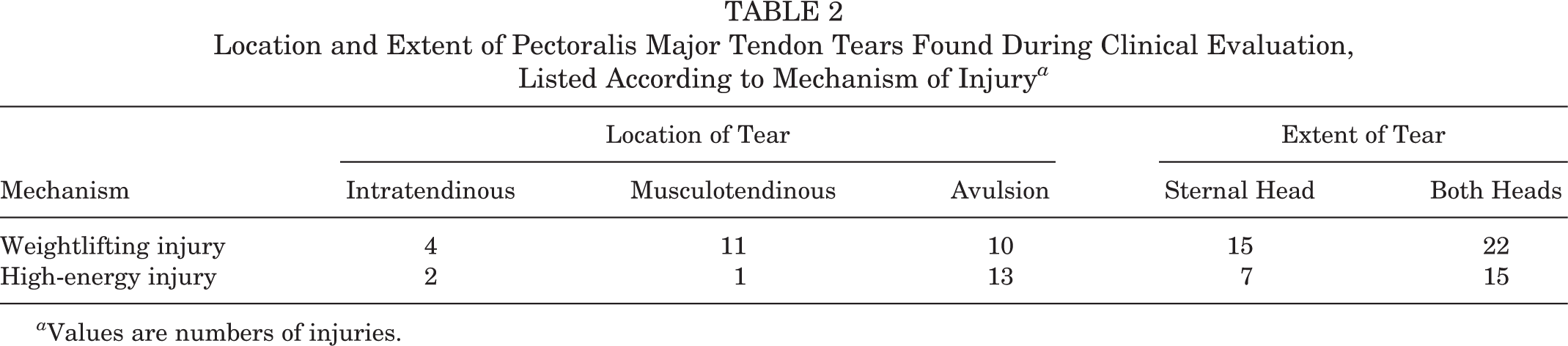
a Values are numbers of injuries.
Patient age at the time of injury had no effect on either clinical tear location (P = .551) or tear extent (P = .773). Time from injury to MRI had no effect on the ability to accurately identify the extent of tear (95% CI, –0.007 to 0.001; P = .163) or location of tear (95% CI, –0.007 to 0.014; P = .510). Additionally, time from injury to surgery did not affect the accuracy of MRI interpretation for tear extent (95% CI, –0.002 to 0.004; P = .448) or tear location (95% CI, –0.12 to 0.005; P = .420).
Discussion
The most important finding of this study was that mechanism of injury was found to significantly affect the location of tendon tears. A significantly higher rate of avulsion injuries was identified in the high-energy traumatic injury cohort compared with that for weightlifting injuries. The military population is subject to unique training requirements, such as airborne operations, that expose soldiers to an increased risk of PM injury. Specifically, PM injuries sustained from the static line while parachuting are the second most common injuries sustained during airborne operations. 16
As described by Labuda et al, 17 the soldier’s arm can become entangled in the static line of the parachute when this line is inadvertently located between the arm and chest at the time the soldier is exiting the plane, causing a violent force to be exerted on a hyperabducted and externally rotated arm. This most commonly results in an injury to the biceps brachii 4 but can also cause injury to the PM. 3 The static line used for airborne operations is a strap connecting the main parachute worn by a soldier to a fixed point in an aircraft and automatically deploys the parachute upon the soldier’s exit from the aircraft.
The PM has 2 distinct divisions: clavicular and sternal. These divisions differ in orientation of their insertions. The sternal division has a greater susceptibility for injury in eccentric loading due to its shortened tendinous length compared with the clavicular division and an increased angle of lateral attachment relative to the overall axis of mechanical force, as described by ElMaraghy and Devereaux. 10 In a cadaveric study, Wolfe et al 24 examined the amount of excursion of the divisions of the PM by measuring the length of fibers in different shoulder positions. Specifically, those investigators found that with a 30° arc of shoulder extension, the lower segments of the sternal division showed twice as much excursion as the rest of the PM fibers. This describes the position seen in the terminal eccentric loading position of a bench press or dip. This would explain why the overwhelming mechanism of injury causing a PM tear is eccentric loading during weightlifting, most commonly during bench press.
Examination of the data from the current study showed a higher rate of avulsion injuries among the high-energy mechanism cohort (81% vs 40%; P = .02). This would seem to suggest that the position of the arm and type of force exerted on it can predispose the arm to a certain type of injury pattern. We surmised that the hyperabducted and externally rotated arm position caused by entanglement in a static line could have created a greater excursion of the PM tendon at the insertion compared with the 30° arc of shoulder extension seen in eccentric loading during bench press. The other possible explanation is that the rate at which the force is applied to the arm accounts for the higher rate of avulsions in the static line cohort.
Large variability was noted in the time from injury to MRI assessment (28.5 ± 76.9 days; range, 0-577 days) and the time from injury to operative repair (33.7 ± 101.15 days; range, 2-725 days). Despite this variability, all PM tears were sufficiently mobilized during surgery to allow for direct repair, and no patients required allograft augmentation for repair. Clinical examination data were not obtained for this study for several reasons: the diagnosis was not in question, operative reports were available for 93% of cases examined, and the focus of the study was on tear extent and location with regard to MRI sensitivity and specificity.
PM tendon injuries are a common condition encountered in the military patient population. MRI has been reported to be both sensitive and specific for identifying these injuries. In this study of a military population of patients treated with PM tendon repair, MRI was found to have a low sensitivity and specificity for identifying the extent of tendon injury (complete vs partial injury). The sensitivity and specificity were improved for locating the type of injury (avulsion vs musculotendinous) but never surpassed a sensitivity of 75%.
MRI has long been reported as an accurate means of identifying PM tendon injuries. 8 Chang et al 7 examined the accuracy of MRI for diagnosis of PM tears by comparing MRI results with intraoperative tear characteristics, finding a high sensitivity for grading of acute PM tendon ruptures: 88% for sternal head avulsions and 85% for clavicular avulsions. For complete tendinous injuries, a 100% sensitivity was reported for both sternal and clavicular injuries, diminishing for partial injuries. A smaller study by Carrino et al 6 showed 100% agreement between MRI interpretation and intraoperative findings.
MRI has been reported to aid in identifying patients indicated for surgical treatment. 8,26 Zvijac et al 26 reported that clinical examination often overestimated the severity of PM injuries as well as the location and extent of the tear. Rather, those investigators reported that MRI was a more accurate assessment of the tear, resulting in a change of treatment plan in 3 of 27 patients who were treated nonoperatively for partial injuries. In contrast to these studies, the current study showed a low sensitivity (51.3%) and specificity (63.6%) for identifying complete tears. The sensitivity and specificity were slightly improved for avulsion (73.9% and 72.2%) and musculotendinous injuries (75% and 79.3%). This study’s finding of a lower sensitivity and specificity of MRI for diagnosis of PM tendon injuries in a military cohort underscores the importance of clinical suspicion given patient history and physical examination. Relying heavily on MRI alone for diagnosis could potentially cause delays in definitive treatment.
Operative treatment of PM tears is recommended for both complete and partial injuries in this population due to occupational requirements and has been reported to result in good clinical outcomes. 9,20,25 Various operative techniques are available for repair depending on the severity of the tear and the location of the tear within the musculotendinous unit. The ability of an MRI to accurately identify these characteristics would lead to improved patient counseling preoperatively as well as improved preoperative surgical planning. It is the senior author’s (S.A.P.) experience that significant variance is observed between tear characteristics seen on MRI and those identified at the time of surgery, an experience represented with the current findings. Whether this is related to the unique injury patterns in this population remains to be elucidated.
Limitations
This study was subject to the inherent limitations of a retrospective design. Operative reports were used as the gold standard for identifying the location and extent of PM tears. However, operative reports were not available for all included patients, and the descriptive information of the PM tear varied among surgeons. Despite this, complete operative data were available in 93% of cases; data regarding extent of tears was available in 88% of cases. There was not a high correlation between musculoskeletal radiology reviewers in this study; however, we believe that this reflects the difficulty in describing the extent and severity of PM tears. Moreover, although the majority of these injuries were imaged acutely, some patients experienced a delay in diagnosis and subsequent imaging, or the responsibilities of their training led to a considerable delay between time of injury and time of imaging.
Conclusion
The mechanism of injury was found to significantly affect the location of tendon tears, with a significantly higher rate of avulsion injuries identified in the high-energy traumatic injury cohort than weightlifting injuries. MRI was found to be less sensitive and specific than previous reports for traumatic PM tendon injuries in this military cohort. Future research should further investigate this difference in injury patterns and investigate how injury mechanism affects surgical and functional outcomes.
Footnotes
Final revision submitted January 27, 2020; accepted February 19, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.A.P. has received consultant fees from Arthrex and Exactech, research support from Exactech, and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Dwight David Eisenhower Army Medical Center Human Research Protections Office (ID No. DDEAMC-18-009/899764).