
Abstract
Background:
Chondral-only fragments of the knee have traditionally been treated with excision, with or without cartilage restoration procedures. This is because of the historical assumption that cartilage has limited ability to heal to cancellous or subchondral bone. There is now a growing body of evidence supporting surgical fixation of these fragments.
Hypothesis:
We hypothesized that surgical fixation of chondral fragments would result in acceptable rates of healing with improvement in clinical outcome scores.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data were collected on 15 surgically fixed chondral-only fragments in 14 patients. We retrospectively collected participant demographic information, lesion characteristics, primary mechanism (osteochondritis dissecans vs traumatic shear injury), fixation methods, reoperation information, second-look arthroscopic information, and clinical outcome scores. The mean clinical follow-up was 3.96 years, with a minimum of 1-year follow-up. All patients underwent follow-up magnetic resonance imaging at a mean of 2 years after the index procedure.
Results:
The mean age of our cohort was 17.7 years. We found an 80% survival rate for fixation of the fragments at a mean 4-year follow-up. There were statistically significant improvements in postoperative Knee injury and Osteoarthritis Outcome Score and Tegner scores compared with preoperative scores. Follow-up magnetic resonance imaging scans showed complete healing in 10 knees, partial healing in 2 knees, and loss of fixation in 3 knees. Second-look arthroscopic surgery of 3 knees for reasons other than fragment symptoms showed healing of the fragment, while arthroscopic surgery of 3 symptomatic knees showed loss of fixation.
Conclusion:
Surgical fixation of chondral-only lesions showed an 80% success rate with improvements in the KOOS and Tegner scores.
Cartilage lesions in the knee are both common and, at times, debilitating injuries with lifelong consequences including a subset that progresses to osteoarthitis. 22,25 These lesions have high clinical failure rates when treated nonoperatively. 8 The majority of these injuries are osteochondral, while the minority are chondral only. Chondral-only lesions can either be created through a shear mechanism or by osteochondritis dissecans (OCD). Fixation of osteochondral lesions demonstrates a high rate of bone-to-bone healing with improved clinical outcomes. 4,9,13,20,24,27,29 However, if the fragment lacks subchondral bone, most textbooks advise removal, with the rationale being that cartilage is not able to heal to bone in light of its avascular nature and the previously held belief that chondrocytes are unable to participate in the healing process because they are “locked” in their lacunae. 23,35
Several studies have demonstrated poor long-term outcomes after surgical excision of moderate to large fragments, whether they were chondral or osteochondral. 1,5,12,15,21,44,45 For this reason, most surgeons elect to treat unstable, symptomatic chondral-only lesions using removal and treat the resultant defects using restorative procedures. These well-known procedures, including marrow stimulation, 19,40 osteochondral autograft transfer, 43 autologous chondrocyte implantation (ACI), 26,32,33,36 –38 and osteochondral allograft transplantation, 14,34 have demonstrated acceptable results. Interestingly, there has been a recent challenge to traditional teaching. There is growing evidence in the literature that cartilage possesses some ability to heal. Both minced autograft cartilage and particulated juvenile cartilage have been used successfully to fill cartilage lesions with “hyaline-like cartilage.” 10,17,18,41,42 Preclinical and clinical studies have demonstrated the ability of surface chondrocytes to escape from their lacunae, migrate, multiply, and form a cartilage extracellular matrix. 3,7,28,31 In both techniques, there is basilar integration of new hyaline-like cartilage to bone. This suggests a possible inherent ability of cartilage-to-bone healing.
Despite the dogma that cartilage-to-bone healing leads to biomechanically insufficient repair, a slowly growing number of case series have shown successful outcomes after open reduction and internal fixation (ORIF). These case studies have shown efficacy in fixing the cartilage-only fragment in both OCD lesions with necrotic subchondral bone and traumatic shear injuries, which typically have an intact subchondral plate. 6,11,16,39
Surgical fixation of the cartilage fragment has several advantages over cartilage restoration procedures. It restores the local architecture of hyaline cartilage unlike microfracture, which replaces the defect with biomechanically inferior fibrocartilage. 2,30 It also prevents donor-site morbidity as with osteochondral autograft transfer; the need for 2 surgical procedures as with ACI; and the removal of normal bone as with osteochondral allograft transplantation, which also involves the cost of the allograft. Importantly, if surgical fixation of the fragment were to fail, no bridges have been burned, and standard cartilage restoration procedures would still be viable salvage options. These attributes make surgical fixation of chondral-only fragments an attractive treatment option.
While there are promising case reports supporting fixation of chondral-only fragments in both OCD and traumatic shear injuries, the total number of reported cases is limited. The purpose of this case series was to add to this growing body of evidence supporting ORIF. This case series presents a large collection of follow-up magnetic resonance imaging (MRI) and second-look arthroscopic data after fixation as well as a discussion of patient factors and fixation methods that may predispose to failure. We hypothesized that surgical fixation of chondral fragments would result in acceptable rates of healing with improvement in clinical outcome scores.
Methods
This was a single-center retrospective case series investigating ORIF of chondral-only fragments of the knee. Institutional review board approval was obtained. Included patients had undergone surgical fixation of a chondral-only fragment of the knee between 2013 and 2015. Patients were identified using operative codes for internal fixation of a fragment in the knee. Both patients with chondral-only OCD fragments and patients with traumatic chondral fractures were included in this study, regardless of the characteristics of the underlying lesion bed. This is because both types of lesions have the capacity to show that a loose cartilage fragment may heal to a bony base, whether that is the native subchondral plate or supplemented with bone grafting. Exclusion criteria were the presence of bone on the fragment and a follow-up of less than 1 year. The definition of a chondral-only fragment for the purposes of this study was the lack of subchondral bone visualized both on MRI scans and on a direct inspection intraoperatively.
There were 26 patients identified using operative codes for internal fixation of a fragment of the knee; 12 patients were excluded for the presence of subchondral bone on the fragment. This left a final cohort of 15 knees in 14 patients that met inclusion criteria. None of these 14 patients was excluded for insufficient follow-up. Overall, 9 of the 14 patients had completed both preoperative and postoperative patient-reported outcome (PRO) measures.
All patients underwent standard preoperative imaging including alignment radiographs and MRI of the knee (Figure 1). Patient demographic information; lesion characteristics; fixation techniques; follow-up MRI scans; and, when available, second-look arthroscopic information were collected via a retrospective chart review (Figures 2 and 3).

Preoperative magnetic resonance imaging scans of a chondral-only lesion of the medial femoral condyle.

Intraoperative photographs of an unstable chondral-only fragment and fixation. (A) Arthroscopic visualization of the lesion on the medial femoral condyle. (B) Two separate chondral-only fragments measuring approximately 3 cm2. (C) Defect base debrided and drilled to promote fragment healing. (D) Fixation of a large fragment onto the lesion bed using PDS absorbable suture.

Postoperative magnetic resonance imaging scans showing a healed fragment.
Postoperatively, patients were immobilized in a straight knee brace removed intermittently throughout the day to permit gentle limited range of motion. Rehabilitation for femoral condyle lesion repair procedures consisted of minimal weightbearing using 2 crutches for 6 weeks, and rehabilitation for patellar lesion repair procedures comprised weightbearing as tolerated in a straight knee brace. At 6 weeks, formal physical therapy was initiated with progression to full range of motion and weightbearing as comfort allowed. Muscle rehabilitation was performed using a “core to floor” approach. Preoperative and postoperative PROs including the International Knee Documentation Committee score, Knee injury and Osteoarthritis Outcome Score (KOOS), 36-Item Short Form Health Survey score, Marx score, and Tegner score were collected in 9 patients. All patients underwent postoperative T1-, T2-, and proton density–weighted MRI of the knee at a mean of 2 years postoperatively to evaluate healing of the fragment, unless indicated earlier by new symptoms. Failure was defined as loss of fragment fixation requiring excision or conversion to a cartilage restoration procedure.
Statistical Analysis
Demographic, lesion, and surgical data were compared among all of the patients meeting inclusion criteria and the 9 patients with completed PRO measures to ensure that they were similar. This was done using the t test, Fisher exact test, and chi-square analysis. Log-rank (Mantel-Cox), Breslow (generalized Wilcoxon), and Tarone-Ware statistical tests were conducted to compare the survival of fixation methods (suture, screws, or combination of both). A paired t test was performed on the 9 patients with complete preoperative and postoperative outcome data. Statistical significance was set as a P value of .05 (IBM SPSS Statistics for Windows, Version 25; IBM Corp).
Results
Table 1 outlines patient, lesion, and surgical characteristic data. Overall, 3 of the fragments were fixed using screws alone, 9 were fixed using PDS suture (DePuy Mitek, Inc) alone, and 3 were fixed using a combination of screws and suture. A total of 2 patients had metal compression screws (Mini Acutrak 2 Bone Screw; Acumed, LLC), and the rest of the screws were bioabsorbable (Biotrak Mini Screw; Acumed, LLC). A cancellous bone graft from the distal femur (proximal to the physis) was used in cases with a bone base defect in 10 of the 15 knees, and bone base drilling was performed in all patients. Also, 1 patient underwent concomitant high tibial osteotomy to correct 7° of varus.
Descriptive Data a
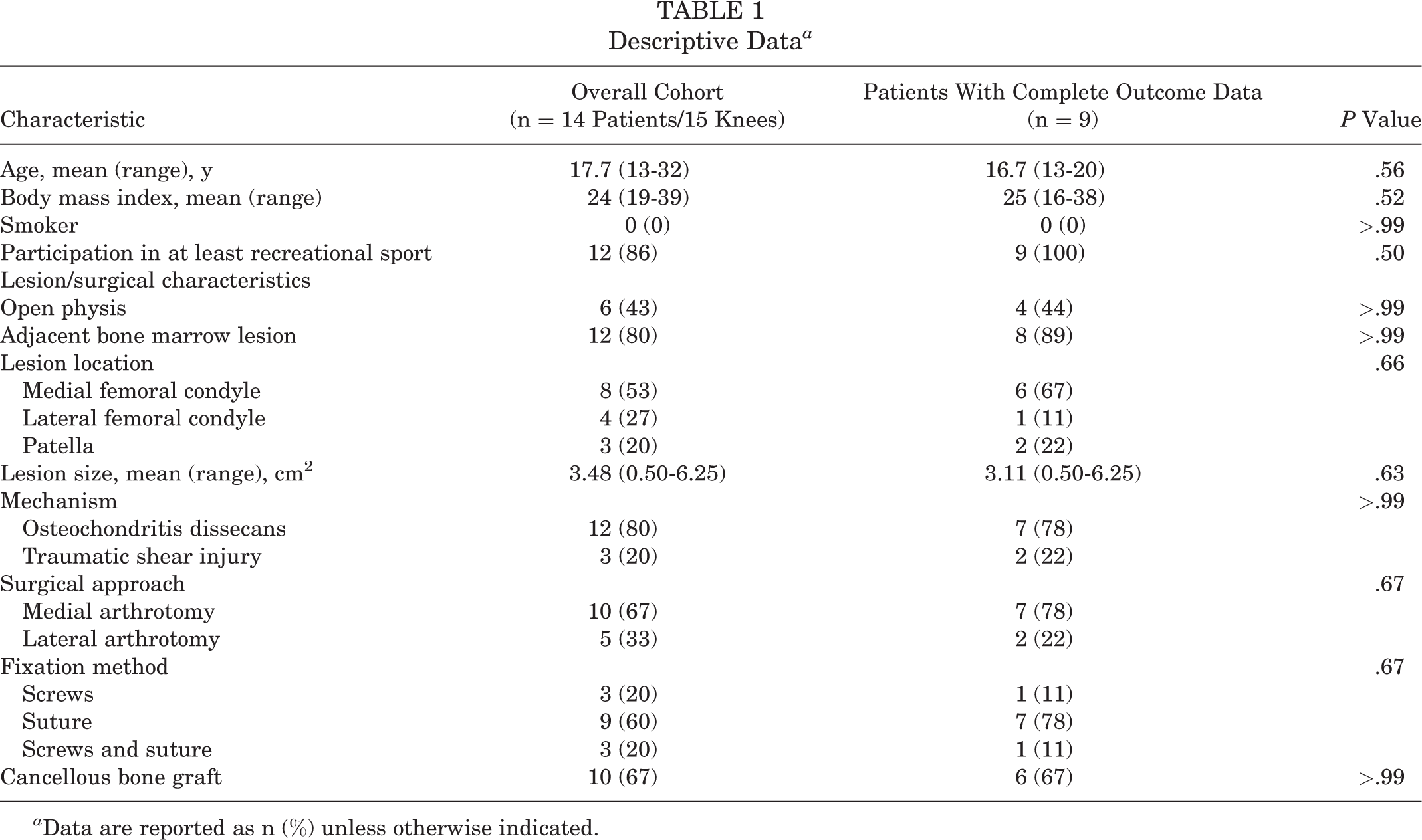
a Data are reported as n (%) unless otherwise indicated.
The mean follow-up was 3.96 years, with a range from 1 to 6 years. The overall complication rate was 33% including 1 case of postoperative stiffness requiring lysis of adhesions, 1 superficial wound infection, and 3 cases of loss of fixation. The overall survival rate of fragment fixation was 80%. The survival of suture-only fixation was significantly longer than that with a combination of suture and screws on all 3 statistical tests (P < .025). There were no failures with the use of screw-only fixation. The mean follow-up was 3.33 years in the 9 patients who had completed postoperative outcome questionnaires. Additionally, 1 patient completed PRO measures at 6 months after a failed fixation and did not complete additional questionnaires; the rest completed PRO measures between 1 and 6 years postoperatively. There were no differences in any demographic, lesion, or surgical characteristics of the PRO group compared with all included patients. There were statistically significant improvements in both KOOS (P < .001) and Tegner (P = .023) scores when comparing latest follow-up scores with preoperative scores. No statistically significant differences were found in the 36-Item Short Form Health Survey and Marx scores (Table 2).
Preoperative and Postoperative Patient-Reported Outcome Data a
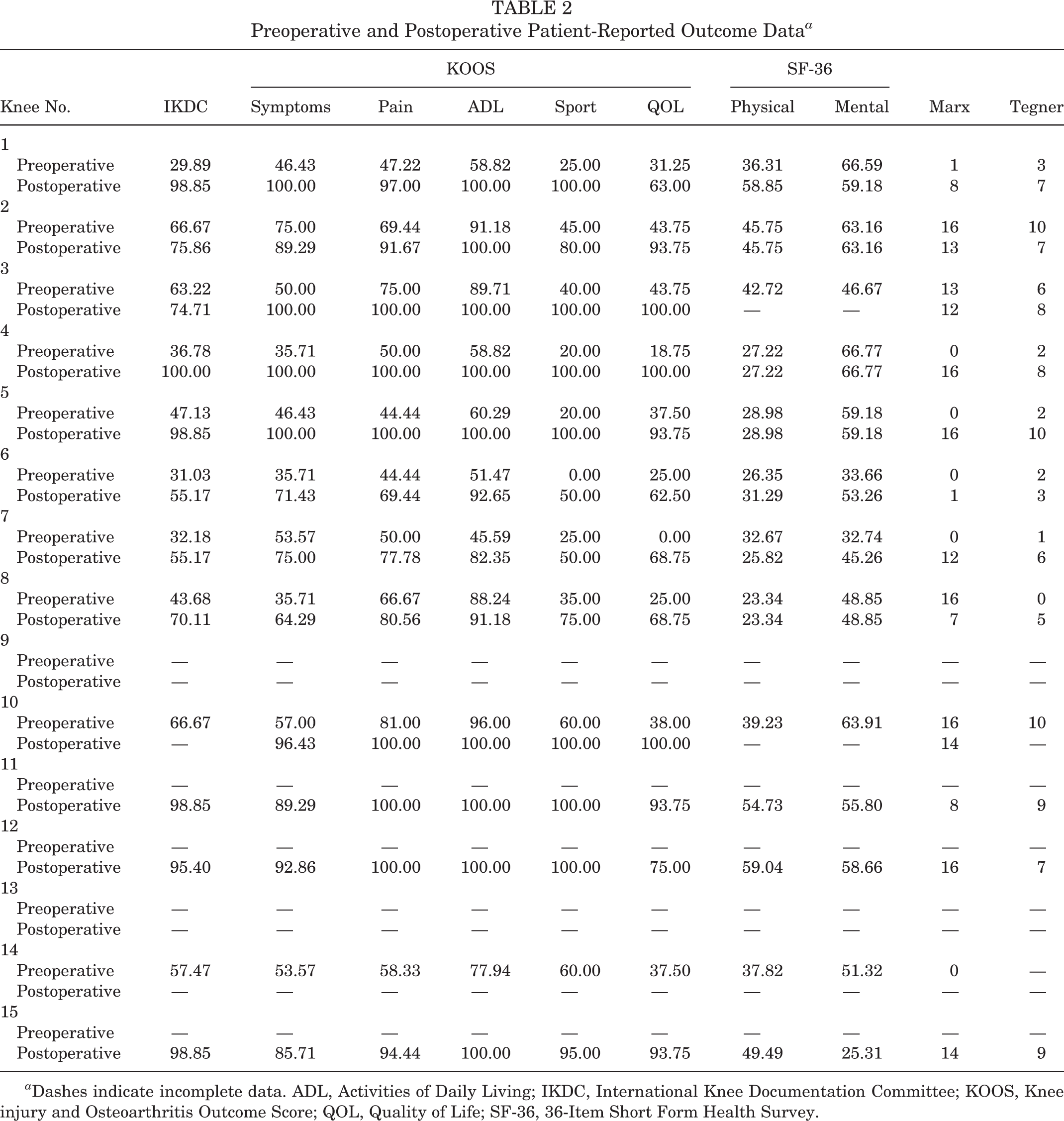
a Dashes indicate incomplete data. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; SF-36, 36-Item Short Form Health Survey.
Follow-up MRI scans were obtained in all patients at a mean of 24 months postoperatively. We found that 10 of the 15 fragments had completely healed. Moreover, 2 of the MRI scans showed a small area of chondral delamination of the fragment; however, both of these patients were asymptomatic and underwent no further intervention. Furthermore, 3 of the MRI scans showed loss of fixation of the fragment, and all 3 patients underwent revision surgery. OCD was the underlying abnormality in all 3 failures. There were no failures in patients with traumatic shear injuries.
A total of 6 knees underwent repeat arthroscopic surgery: 2 for planned screw removal at 6 weeks postoperatively, 1 for lysis of adhesions for postoperative stiffness, and 3 for symptomatic lesions requiring excision or conversion to cartilage restoration. The 2 planned reoperations for implant removal at 6 weeks postoperatively and the reoperation for lysis of adhesions showed a healed chondral fragment. Of the 3 patients with failed primary fixation, 1 patient had the procedure converted to ACI, and the remaining 2 patients had the fragment excised and are being followed for symptom development. Details of these clinical failures can be found in Table 3.
Descriptive Data for 3 Patients Who Had Failed Primary Fixation a

a F, female; M, male; OCD, osteochondritis dissecans.
Discussion
Our case series expands on the existing literature and, to our knowledge, is the first study to report on follow-up MRI of all knees undergoing fragment fixation as well as to report on 6 second-look arthroscopic procedures. In total, 10 of the 15 knees showed complete healing on postoperative MRI scans. Additionally, 2 patients had partial delamination of less than 50% of the fragment but were asymptomatic from their lesions. The remaining 3 patients showed loss of fixation as discussed above. Regarding PROs, we found a statistically significant improvement in both KOOS and Tegner scores when comparing final follow-up scores to preoperative scores, with a mean PRO follow-up of 3.33 years.
With regard to the patients with clinical failures, 2 of the patients were older with closed physes. Both screws and suture were used in their repair procedures because of instability of their fragments when fixed using screws in isolation, and therefore the repair may have been inherently more likely to fail. While these 2 patients had several possible risk factors for failure, there was also a failure in a young female patient with an open physis. Her fragment was stable using suture fixation alone. Eventually, her fixation failed, and her resulting chondral defect was addressed successfully using membrane-associated ACI. This highlights the fact that, even in an ideal patient, loss of fixation is still possible and patients should be counseled accordingly. It is our impression that patients with unstable fragments and closed physes may be at an even greater risk for failure.
We included all patients who underwent fixation of chondral-only fragments of the knee, regardless of whether the indication was OCD or a traumatic chondral fracture. There were no failures in the 3 patients with traumatic shear injuries, with all failures occurring in the OCD group. This was a somewhat unexpected finding, as we speculate that OCD fragments are more likely to have microscopic bone and therefore more likely to have the added benefit of bone-on-bone healing. However, OCD also typically has necrotic subchondral bone requiring bone grafting, which may be a less favorable healing interface. Larger comparative studies between these 2 indications for chondral-only fixation would be needed to determine if they have a significant effect on union rates.
Previous studies have looked at outcomes of fixing chondral-only fragments using either traumatic shear or OCD mechanisms and have shown favorable results. Siparsky et al 39 published a case series of 3 patients who had healed chondral shear fragments on postoperative MRI scans; 2 of the patients underwent repeat arthroscopic surgery, which demonstrated reintegration of the fragment within the defect. Churchill et al 11 reported on 10 male patients, with 8 who had follow-up MRI scans that demonstrated healing of the chondral shear fragment. Also, 1 patient underwent second-look arthroscopic surgery for hardware removal, which also demonstrated healing of the fracture. Fabricant et al 16 published a similar case series of 15 patients with traumatic shear fragments. There was 1 patient (7%) who had loss of fixation requiring fragment excision; 9 of the remaining 14 patients underwent follow-up MRI, with only 5 showing complete healing. Anderson et al 6 published a series of 5 patients who underwent primary fixation of chondral-only OCD fragments. A total of 4 of the 5 patients had completely healed fragments at second-look arthroscopic surgery, and 1 patient demonstrated healing of two-thirds of the fragment, which was treated using debridement and drilling. Patients had no substantial difference in pain or function in activities of daily life compared with controls but had worse sport function and knee-related quality of life.
There were several limitations to our study. First was the small overall sample size of 15 operative lesions and an even smaller sample size of 9 with complete PRO measures. Yet, given the rarity of this injury and novelty of the fixation method, these data are useful to expand on the existing literature. Additionally, there is inevitable selection bias when performing a retrospective case series. Not all purely cartilage lesions over the time course of this study were treated using surgical fixation. Patients with comminution of the fragment and older patients were typically treated using fragment excision and staged cartilage restoration procedures and were not included in this study. This could potentially lead to selecting patients and lesions that are more likely to have successful surgical fixation. The results from these patients treated nonoperatively or using cartilage restoration are outside the scope of this case series but would be valuable in future cohort or randomized controlled investigations. To definitively confirm healing and restoration of the native architecture, a follow-up biopsy would need to be performed, which was not done in this case series. Last, although the mean follow-up in our study was 4 years, this may be an insufficient amount of time to track the possible progression of these lesions. Future studies should include prospective data collection with a long-term follow-up and possible biopsy or thin-section high-quality MRI of the cartilage-bone interface to evaluate healing of the fragment.
Conclusion
Purely chondral fragments of the knee are rare and involve challenges in their management. Recent studies have suggested surgical fixation of the fragment as a viable treatment option. Our study showed that 80% of these fragments survived at a mean of 4 years, with 67% demonstrating complete union on MRI scans. Overall, surgical fixation of cartilage lesions of the knee remains a viable treatment option that could potentially reduce the need for cartilage restoration procedures.
Footnotes
Acknowledgment
The authors acknowledge Vicki Snodgrass for her assistance and coordination.
Final revision submitted April 23, 2020; accepted May 11, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.F. has received consulting fees from Aastrom Biosciences, Aesculap/B. Braun, Arthrex, CartiHeal, Ceterix Orthopaedics, Cook Biotech, DePuy Synthes, Exactech, ISTO Technologies, MedShape, Moximed, Organogenesis, Osiris Therapeutics, Regentis Biomaterials, RTI Surgical, Samumed, Vericel, Zimmer Biomet, and ZKR Orthopedics; has received research support from Active Implants, Arthrex, Episurf Medical, Fidia Pharma, JRF Ortho, Moximed, Novartis, Organogenesis, Samumed, Vericel, and Zimmer Biomet; has received nonconsulting fees from Aastrom Biosciences, Arthrex, Moximed, Organogenesis, Vericel, and Zimmer Biomet; has received royalties from Arthrex, BioPoly, DePuy Synthes, Organogenesis, Springer, and Thieme Medical Publishers; and has stock or stock options in MedShape and Ortho Regenerative Technologies. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Indiana Orthopaedic Hospital (study No. 0179).