
Abstract
Background:
Standard knee arthroscopy portals are frequently used to address retropatellar chondral pathology. Alternative portals may offer a safe and simple substitute, particularly when reaching the base of deep lesions is required.
Purpose:
To describe and assess the safety of accessory retropatellar portals.
Study Design:
Descriptive laboratory study.
Methods:
An anatomic study was performed on 10 fresh-frozen cadaveric knees. Medial and lateral retropatellar portals were created, and the distance to adjacent neurovascular structures (common peroneal nerve [CPN] and infrapatellar branch of the saphenous nerve [IPBSN]) and bony landmarks (medial and lateral epicondyles and margins of the midpatella) was recorded. A clinical account of portal use is provided through a retrospective chart review.
Results:
The medial and lateral retropatellar portals were a mean 15.8 ± 15.5 mm and 53.8 ± 7.2 mm from the IPBSN and CPN, respectively. No nerves were contacted in any specimens. Clinically, the portals have been used in 109 cases over a 7-year period without complication.
Conclusion:
The high level of IPBSN variability poses some risk to medial portal use; however, there is little to no risk laterally. Clinical experience with portals suggests that they can be used safely. We recommend careful blunt dissection to minimize chance of iatrogenic nerve injury.
Clinical Relevance:
Retropatellar portals may offer improved access to chondral lesions of the patella, thereby safely allowing one to maintain an arthroscopic approach.
Keywords
Chondral and osteochondral patellar defects are a common orthopaedic problem. According to an influential retrospective analysis of 25,124 symptomatic knees undergoing arthroscopic examination, the highest portion (36%) of knees in which lesions were observed had patellar pathology presenting as an isolated chondral defect, osteochondritis dissecans lesion, osteoarthritis, or as another uncategorized lesion. 36 While patellar chondral lesions may vary in location and thickness, the majority are elliptically shaped and centrally located. 13 When present, patellar lesions can produce knee pain, swelling, or clicking and create instability that demands surgical intervention. 22,27 Arthroscopic surgery is often the first surgical approach chosen, as it is relatively quick, easy, and minimally invasive.
Arthroscopy for patellar chondral lesions most commonly involves the use of standard anterolateral and anteromedial portals (Figure 1, A and C), while only occasionally drawing on accessory portals. 10 Some may have found suprapatellar portals useful, for example, but these are not intended for patellar chondral lesions and have significant risks associated with their use, such as injury and subsequent atrophy of the vastus medialis muscle. 32 Given the confined nature of the patellofemoral and retropatellar spaces, use of standard portals limits the surgeon’s ability to approach deep, centralized lesions in a perpendicular fashion and reach their base, 2 factors that are critical to several modern-day arthroscopic techniques (Figure 2). 6,19,20,25,29,30 Curved shavers and bent awls of varying degrees have been designed in response to this problem, but both may have difficulty addressing deep lesions safely, and the latter can clog. 35
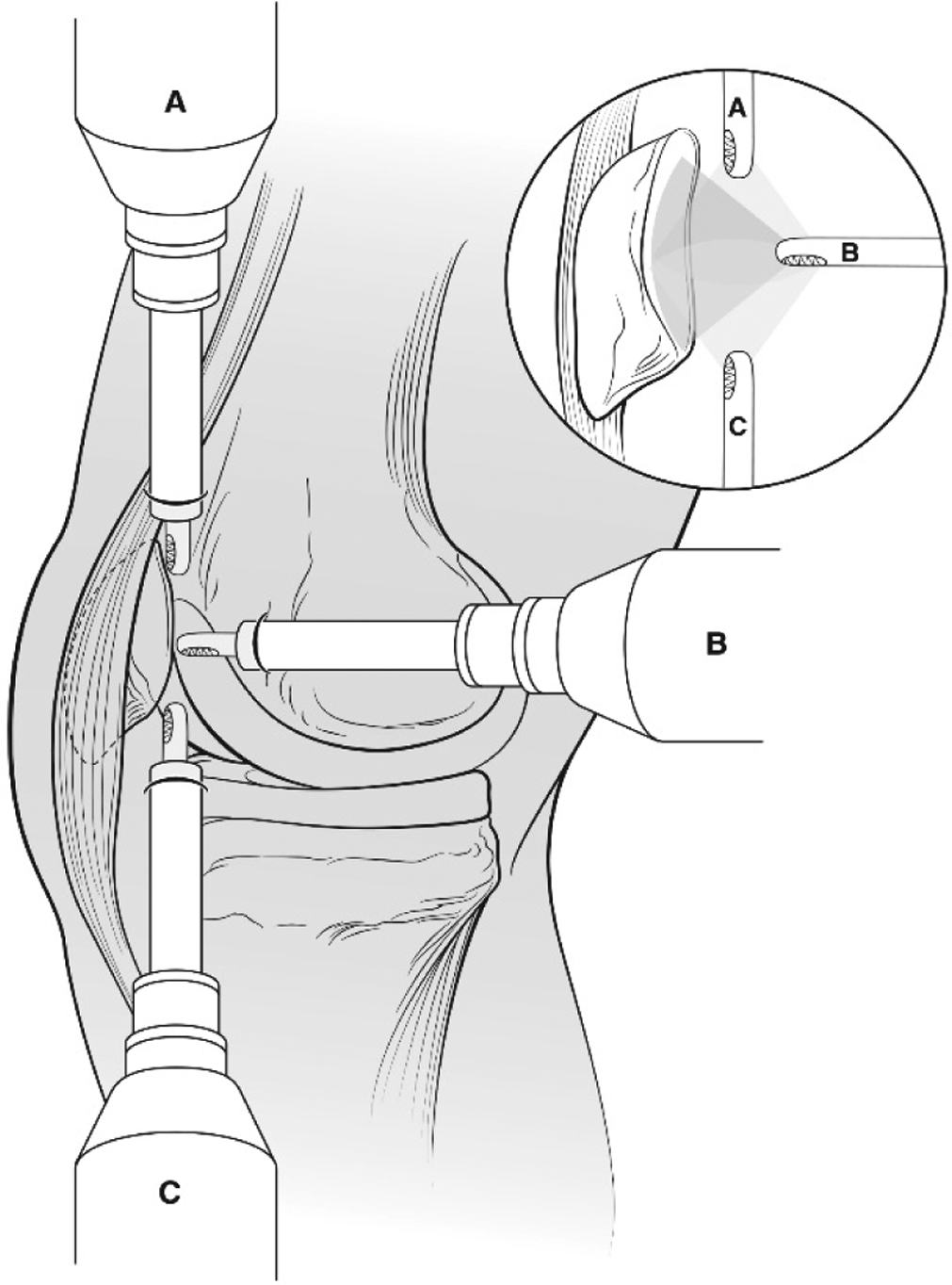
The medial retropatellar portal (B) offers improved perpendicularity to the posterior patella in comparison with the (A) standard superomedial or (C) anteromedial portals.
Use of straight shaver and standard portals makes it difficult to achieve perpendicularity to the undersurface of the patella, particularly for treating deep chondral defects.
We believe that current techniques could benefit from a safe portal designed specifically for the purpose of addressing retropatellar chondral pathology. By using more posteriorly located portals and aiming anteriorly toward the patellar undersurface, we believe these portals allow easier manipulation and improved visualization (Figure 1, B). The angle of approach can be enhanced further through concomitant patellar manipulation (Figure 3). Similar portals have been described briefly as part of a larger technical note by Kim and Kim. 17 These authors appreciated the value of “face-to-face” positioning of arthroscopic equipment to the patellar undersurface but did not elaborate further. 17
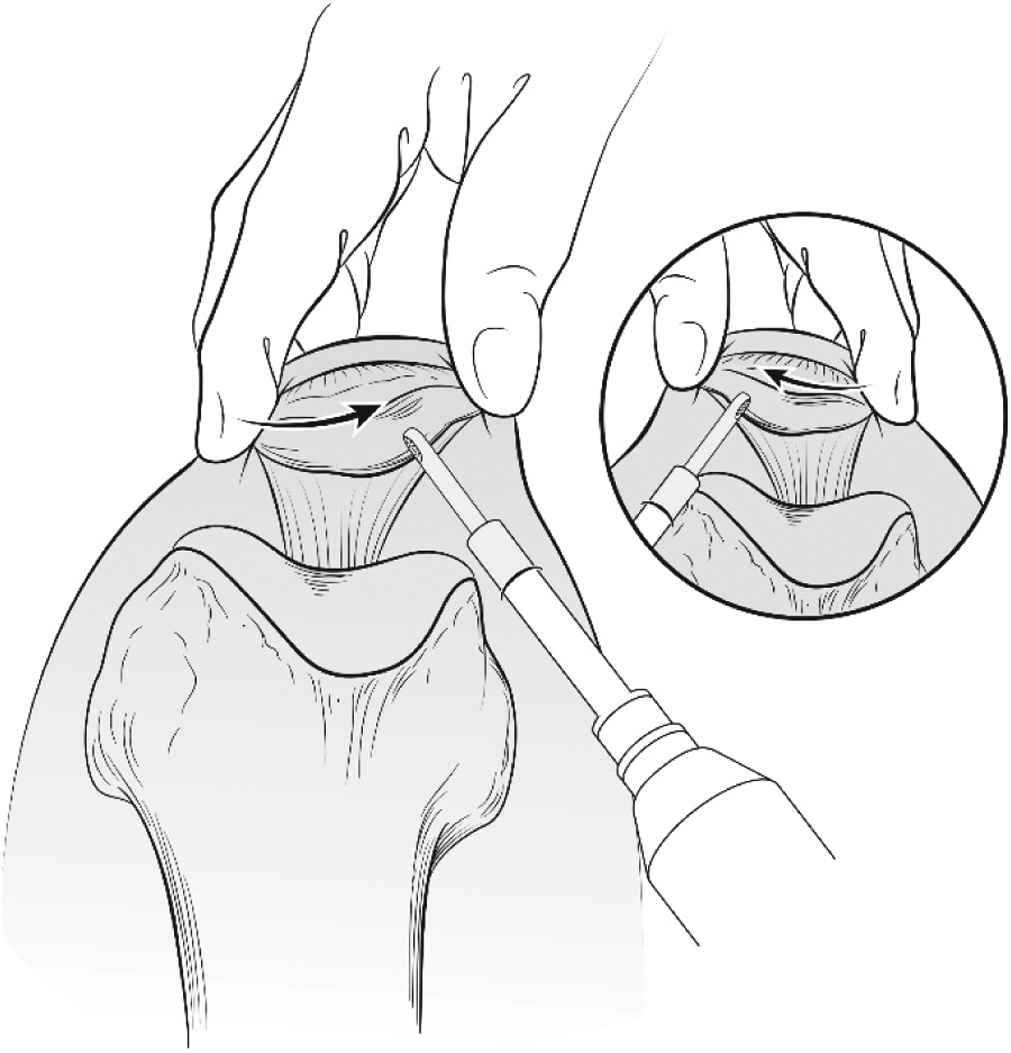
Manual displacement of the patella toward the side of entry facilitates optimal positioning of equipment during arthroscopic surgery with retropatellar portals.
The present study aimed to describe portals specifically designed to address retropatellar chondral pathology, hereinafter referred to as retropatellar portals, while also describing their location, evaluating their safety, and providing a clinical account of their use. We hypothesized that the aggregate cadaveric and clinical data will demonstrate low clinical risk of retropatellar portal use.
Methods
Dissection
Ten fresh-frozen cadaveric knees (Biological Resource Center of Illinois) were used after approval from the NorthShore University HealthSystem Institutional Review Board. Knees were approximately 42 cm in length, an average of 22 cm proximal and 20 cm distal to the joint line. The study sample included 3 right, 7 left, 5 male, and 5 female adult knees ranging from 37 to 91 years of age (mean ± SD, 57.9 ± 16.1 years). Original patient height and weight ranged from 61 to 72 inches (mean, 67.8 inches) and 58.97 to 104.33 kg (mean, 74.62 kg), respectively. All knees were thawed in room temperature water (approximately 23°C) approximately 7 hours before arthroscopy. All arthroscopies and dissections were carried out by a skilled orthopedic surgeon (J.L.K.) to ensure consistency of procedure and performance. A single 3-L bag of fluid hung 1 m above the surgical table for gravity inflow irrigation.
All arthroscopies were performed with the knee in complete extension. A standard arthroscopic technique was used to establish an anterolateral viewing portal. A 30°, 4.0-mm arthroscope (Hopkins; Karl Storz) was inserted to visualize the internal architecture of the knee. Knees included in this study had no significant intra- or extra-articular abnormalities. Ten knees were screened, and all were included. A grade 2 chondromalacia was the most significant finding, seen in 1 specimen.
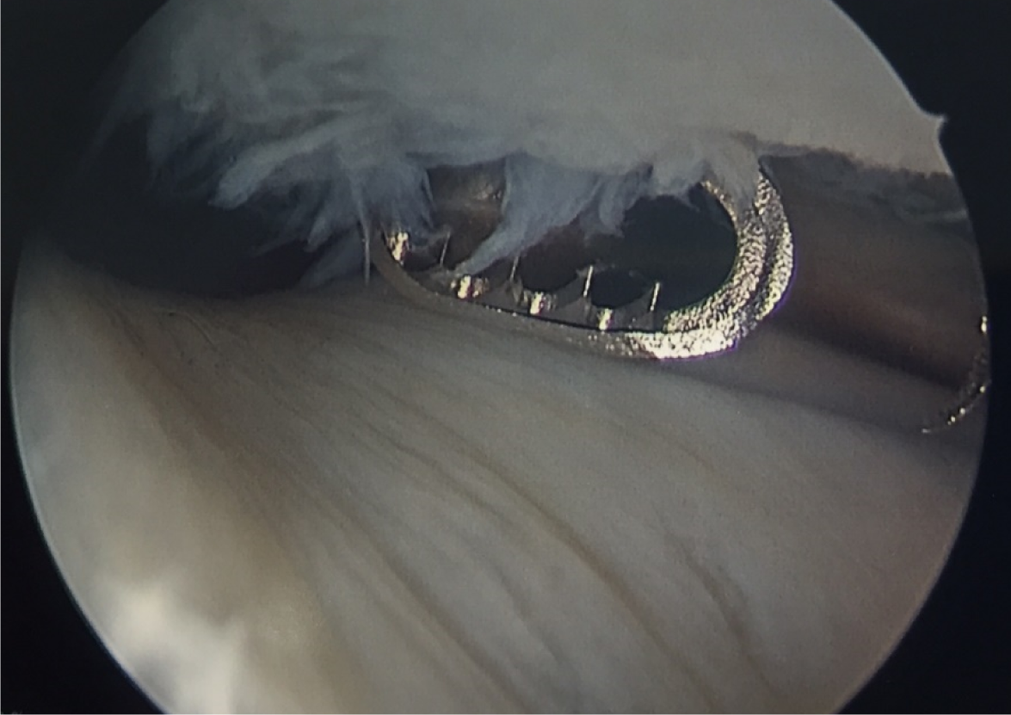
A spot roughly between the midpatella and lateral epicondyle of the femur was used to approximate the lateral portal site, while a point approximately 1 cm distal to this location, using the medial epicondyle of the femur, was used for the medial portal. An 18-gauge spinal needle was inserted and aimed anteriorly under direct visualization with the knee still in extension. The patella was maximally translated by manual displacement toward the spinal needle for optimal placement (Figure 3). Optimal placement was determined to be the location where the spinal needle reached the furthest aspect of the contralateral undersurface in a perpendicular or near-perpendicular fashion (Figure 4). A superficial skin incision was made to permit joint capsule entry by a 5.15-mm cannula and blunt-tipped trocar. The cannula was left in place for dissection and recording of measurements. All measurements were taken from where the cannula entered the skin.

An 18-gauge spinal needle aimed anteriorly toward the patellar undersurface was used to determine optimal portal placement. Optimal placement was determined to be the location where the spinal needle reached the furthest aspect of the contralateral undersurface of the patella in a perpendicular or near-perpendicular fashion. The intra-articular view of the spinal needle oriented virtually perpendicular to the medial facet of the patella is shown.
Dissection was performed with great care to preserve the underlying anatomy. Bony landmarks and relevant neurovascular structures were used to describe portal location and assess risk, respectively. Portals were identified as being anterior to the larger branches of the superior genicular arteries at this time, thus we prioritized the risk posed to the surrounding nerves. The midpatella, epicondyle, and closest branch of the infrapatellar branch of the saphenous nerve (IPBSN) served as medial reference points (Figure 5A), while the midpatella, epicondyle, and common peroneal nerve (CPN) were used laterally (Figure 6A). A digital precision caliper (Tool Shop; Menards) was used to take 3 sets of measurements from each of the landmarks. The nearest point to the landmark in a straight line was used in all cases except for the epicondyles, in which the midpoints were used. All measurements were recorded with the knees in complete extension and were agreed upon by both authors (J.L.K. and A.L.L.) before being recorded. The distances were averaged to the nearest 1/10 mm, and standard statistical analyses were performed (mean ± SD, median, and range). Two-sample t tests were used in some instances to evaluate relevant left-versus-right anatomic relationships and compared with another published study. 24 The level of significance for these tests was always α < 0.05.

(A) Left knee specimen shown rostrally to caudally from left to right. Placement of medial retropatellar portal maintained by cannula for dissection and measurements to follow. Medial femoral epicondyle is marked (purple circle). (B) Left knee specimen shown rostrally to caudally from left to right. The infrapatellar branch of the saphenous nerve (IPBSN) was a mean 15.8 ± 15.5 mm from the medially chosen portal site. Proximal blue arrowhead, IPBSN; distal blue arrowhead, medial epicondyle.

Left knee specimen shown caudally to rostrally from left to right. Safe placement can confidently be established on the lateral aspect of the knee guided by palpation of bony landmarks. Lateral retropatellar portal site is maintained by cannula for dissection and measurements to follow. Lateral femoral epicondyle (purple circle) and fibular head (purple semicircle) are marked. (B) Left knee specimen shown caudally to rostrally from left to right. The common peroneal nerve (CPN) was a mean 53.8 ± 7.2 mm from the laterally chosen portal site (blue arrowhead). Lateral femoral epicondyle (purple circle) and fibular head (purple semicircle) are marked.
Clinical Use
The senior author (J.L.K.) has incorporated retropatellar portals into 3 procedures (osteochondral autograft transplantation [Figure 7], chondroplasty with drilling [Figure 8], and drilling of an osteochondritis dissecans lesion) since 2009. When retropatellar portals are used, the anterolateral and anteromedial portals are used for lateral and medial viewing of the patellar facets, respectively. After institutional review board–exempt submission approval was obtained, deidentified data from this time period was retrospectively collected from patient medical records. Data obtained for the purposes of this study included patient age, sex, and body mass index (BMI).

Intraoperative view of osteochondral autograft transplantation surgery (OATS) being performed in near-perpendicular alignment to the undersurface of the patella through the use of retropatellar portals.

Intraoperative drilling of a focal chondral defect on the undersurface of the patella. Retropatellar portals allow access to the base of deep chondral lesions in a perpendicular or near-perpendicular fashion.
Results
Dissection
The medial retropatellar portal pierced the skin going subcutaneously. The mean distance from the portal to the IPBSN was 15.8 ± 15.5 mm (Figure 5B), to the midpatella was 49.9 ± 10 mm, and to the medial epicondyle was 14.6 ± 4.7 mm (Table 1). The mean distance from the IPBSN to the midpatella was 57.6 ± 17.6 mm and to the medial epicondyle was 13.5 ± 9.3 mm (Table 2).
Results of Measurements Taken From Base of Cannula a

a CPN, common peroneal nerve; IPBSN, infrapatellar branch of the saphenous nerve.
Results of Additional Measurements Taken From IPBSN a

a IPBSN, infrapatellar branch of the saphenous nerve.
The relationship between the IPBSN and the midpatella was not significantly different when comparing measurements from left knees (mean, 57.7 ± 19.3) to right knees (mean, 57.3 ± 16.4) in this study (t(8) = 0.03; P = .98) nor when compared with the study by Mochida and Kikuchi 24 (left knees: mean, 52.2 ± 12.4; t(71) = 0.86; P = .39; right knees: mean, 54.2 ± 12.3; t(64) = 0.68; P = .68). The relationship between the IPBSN and the medial epicondyle was also not significantly different when comparing measurements from left knees (mean, 12.7 ± 11.1) to right knees (mean, 15.5 ± 3.3) in this study (t(8) = 0.43; P = .68).
The lateral retropatellar portal pierced the skin going subcutaneously. It entered the proximal half of the iliotibial band and traveled through the lateral retinaculum to enter the joint capsule. The mean distance from the lateral retropatellar portal to the CPN was 53.8 ± 7.2 mm (Figure 6B), to the midpatella was 46.6 ± 4.7 mm, and to the lateral epicondyle was 13.3 ± 3.8 mm (Table 1).
The medial retropatellar portal was posterior to the IPBSN in 3 specimens and anterior to it in 7 specimens. The lateral retropatellar portal was consistently located posterior to the CPN. No nerve contact or transection occurred in any cases.
Clinical Use
The portals have been used in a total of 109 cases over 7 years. Cases consisted of 7 osteochondral autograft transplantations, 99 drillings of focal chondral defects, and 3 drillings of osteochondritis dissecans lesions. There were 47 male and 62 female patients with a mean age of 47 years (range, 16-72 years) and BMI of 28.38 kg/m2 (range, 18.08-53.26 kg/m2). In all cases, the bone at the base of the lesion could be drilled in a perpendicular or near-perpendicular fashion. There were no reported complications or evidence of iatrogenic nerve injury related to portal use.
Discussion
Injury to the IPBSN is likely the primary concern with retropatellar portal use. The IPBSN is a purely sensory branch of the saphenous nerve that supplies the inferomedial capsule, patellar tendon, and anteromedial aspect of the knee. 5,9,15 After piercing the sartorious and deep fascia, it follows a highly variable path curving medially and anteroinferiorly over the knee. 14,15,24 Iatrogenic damage to the IPBSN has been reported after many procedures, including total knee arthroplasty, arthrotomy, anterior cruciate ligament reconstruction, open meniscectomy, resection of the prepatellar bursa, retrograde femoral nailing, tibial nailing, and even arthroscopy using standard portals. 9,14,16 Mochida and Kikuchi 24 recognized the precarious position of the IPBSN during standard knee arthroscopy and were the first to evaluate the risk its variable branching pattern imposed. Finding consistency within IPBSN branching has been the aim of many studies since. 2,9,14,16,18,34
Despite our relatively small sample size of 10 cadaveric knees, the relationship between the IPBSN and bony landmarks was no different than those reported in the large seminal study by Mochida and Kikuchi. 24 In their study of 129 knees, these authors reported an insignificant difference in the mean distance from the IPBSN to the midpatella in left (52.2 mm) and right (54.2 mm) knees. 24 Our study revealed comparable distances (left, 57.7 mm; right, 57.3 mm) that were not significantly different from each other or those of Mochida and Kikuchi. 24
Authors have attempted to mitigate risk of IPBSN transection by providing operating surgeons with relative zones of safety when incising on the anterior knee. Mochida and Kikuchi 24 used the mean distance of the nerve ± 2 SDs to suggest an area safe enough for blind puncture. The area they describe extends from the midpatella to approximately 30 mm medially. 24 Despite using the junction between the medial patellar tendon and the midpatella, a slightly more distal landmark than that used by Mochida and Kikuchi 24 or the present study, Ebraheim and Mekhail 9 found a similar safe zone extending to 31 mm in their study of 28 knees.
Our average site for portal placement relative to the midpatella was 49.9 mm. While this distance is beyond the suggested guidelines of “no risk” described by both Mochida and Kikuchi 24 and Ebraheim and Mekhail, 9 it is well within the gray zone (31-60.7 mm, “unlikely place to find the nerve”) defined by the latter authors 9 and the low-risk zone described by Kerver et al, 16 extending from the patellar apex medially and cranially. All medial portal–to-IPBSN measurements were also within the most recently reported guidelines of Kalthur et al, 14 who described a safe zone of <4 mm or >10 mm from the midpatella in their study of 32 knees. We believe these studies provide a reliable map of the proposed region we intend for retropatellar portal placement and collectively suggest minimal risk.
We recognize there is always some risk; risk of IPBSN transection exists even with standard arthroscopy. 9,14,24 Additional precautions can be taken to minimize this risk. Transillumination of the medial knee allows one to observe the veins accompanying the saphenous nerve. 4 Ultrasound with or without Doppler can be used to preidentify the nerve. 2,18 We personally recommend a superficial-only skin incision and the use of a blunt-tipped trocar. Additionally, structures such as the superior medial and lateral genicular arteries and the medial patellofemoral ligament occur at the region under investigation. The larger branches of the genicular arteries were not felt to be at significant risk during dissection, and we have not seen any iatrogenic injury clinically. Iatrogenic patellar instability caused by this portal has also not been seen; given the position of the medial portal it is likely that this portal passes through a portion of the medial patellofemoral ligament. Ultimately, the decision to perform any knee arthroscopy should include careful deliberation weighing the undesirable complications with resolution of the patient’s presenting symptoms.
An additional finding of the present study was that the margin for safe portal placement was much wider on the lateral knee. The relationship between the lateral portal location and the CPN was measured in this study because it is the only laterally located structure critically important to avoid and is used as a landmark in other anatomic studies. 4,21 Nonetheless, the nerve proved to be reliably distal (minimum, 39.4 mm) to any portal site. When accessing the posterior patella is the surgeon’s end goal, safe portal placement can be achieved with utmost confidence on the lateral knee.
Complications of IPBSN injury are purely sensory in nature and include numbness, paresthesia, pain with kneeling, painful neuromas, and, rarely, reflex sympathetic dystrophy. 1,8,12,28,33,34 Our clinical study of 109 patients revealed no such complications. Our anatomic study showed that the medial and lateral epicondyles can serve as dependable landmarks for portal placement (± 4.7 mm and ± 3.8 mm, respectively). When placed at this site, these portals have allowed us to achieve perpendicular or near-perpendicular access to the undersurface of the patella, and particularly, to the base of chondral defects without damage to adjacent cartilage. Perpendicular or near-perpendicular drilling without injury to native cartilage is important for osteochondral plug alignment, microfracture procedures, and in addressing osteochondritis dissecans lesions. This portal location has allowed us to maintain an arthroscopic approach and avoid everting the patella during these procedures.
Limitations
We believe the advantage of our portals is in their practicability of accessing and viewing the posterior patella, but given the design and findings of the present study, some limitations do exist. The most apparent limitation is the small cohort used. Our findings do not offer a complete picture of the adult population undergoing arthroscopy considering the immense variability that exists in joint size, compliance, and anatomy. The comparability of our results with other larger studies does offer some reassurance. 2,9,14,16,18,24,34 Second, the portals were all established on cadaveric limbs in isolation. We do believe, however, that the full joint extension and patellar laxity needed to manipulate the patella and establish the portals is as easy to achieve on a true patient. Indeed, the senior author’s use of these portals in practice reaffirms it. Finally, while intraoperative images and clinical examples were provided, the purported superior working and viewing angle the portals permit was not objectively studied. While important, we felt description of such would be secondary to demonstrating portal safety.
Conclusion
The objective of the present study was to evaluate the safety of the described retropatellar portals for treating chondral lesions of the patellar undersurface. While the IPBSN is exposed to some risk during portal creation, we believe that even medial portal use is clinically acceptable, particularly when aimed at treating problematic pathologies; lateral neurovasculature, conversely, poses little to no reason for caution. While not objectively evaluated in the present study, we believe retropatellar portals offer uninhibited entry to the retropatellar space and a more perpendicular alignment of arthroscopic instruments. Such orientation is essential in properly executing a number of chondral resurfacing and restorative techniques, namely microfracture, mosaicplasty, and autologous matrix-induced chondrogenesis. 3,7,11,23,26,31 Thus, the findings of the present study are valuable in providing the arthroscopist with an alternative portal option that may allow him or her to address deep, centralized chondral lesions of the patella effectively while maintaining an arthroscopic approach.
Footnotes
Acknowledgment
The authors thank the Grainger Center for Simulation and Innovation for their accommodations and acknowledge Jin-Cheng Zhao, MD, for his assistance with study preparation.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.