
Abstract
Objective
To analyze the clinical outcomes, knee function, and activity level of patients after treatment of full-thickness cartilage defects involving the patellofemoral compartment of the knee with cryopreserved osteochondral allograft.
Design
Nineteen patients with cartilage defects involving the patellofemoral compartment were treated. The average age was 31 years (range 15-45 years), including 12 females and 7 males. Patients were prospectively followed using validated clinical outcome measures including Veterans RAND 12-item Health Survey (VR-12), International Knee Documentation Committee (IKDC), Knee Injury and Osteoarthritis Outcome Score (KOOS), and the Tegner activity scale. Graft incorporation was evaluated by magnetic resonance imaging (MRI) or second-look arthroscopy.
Results
The cartilage defects included the patella (n = 16) and the femoral trochlea (n = 3). Mean VR-12 scores increased from 31.6 to 46.3 (P < 0.01), mean IKDC increased from 40.0 to 69.7 (P < 0.01), mean KOOS increased from 53.9 to 80.2 (P < 0.01), and mean Tegner scores increased from 3.0 to 4.9 (P < 0.01), at average follow-up of 41.9 months (range 24-62 months). Of the 3 patients who underwent second-look arthroscopy, all demonstrated a well-incorporated graft. Mean MOCART score for the 6 patients with follow-up MRI was 62.5 (range 25-85). The reoperation rate was 21.1% and 2 patients (12.5%) experienced progressive patellofemoral osteoarthritis requiring conversion to patellofemoral arthroplasty.
Conclusion
Patients with unipolar cartilage defects involving the patellofemoral compartment of the knee can have positive outcomes at minimum 2-year follow-up after surgical treatment with a cryopreserved osteochondral allograft when concomitant pathology is also addressed, but the reoperation rate is high and bipolar cartilage lesions may increase the failure rate.
Keywords
Introduction
Articular cartilage is a highly organized tissue, but it lacks innate regeneration ability due to its paucity of blood supply. 1 Isolated cartilage defects can lead to significant pain and disability. 2 The incidence of these defects has increased over time and may be related to a rise in sports participation by young individuals.3,4 Current cartilage restoration options for isolated full-thickness cartilage lesions include osteochondral autologous transfer (OATS), osteochondral allograft transplantation (OCA), autologous chondrocyte implantation (ACI), and microfracture. OATS is limited to smaller osteochondral defect sizes due to associated donor site morbidity. 5 OCA is indicated for larger lesions, but requires size-matched donor grafts. 6 ACI has shown promising short- and long-term outcomes7,8 and may be used to treat larger lesions. 6 Its use is limited though by its 2-stage nature and high cost.9,10 Microfracture has demonstrated variable outcomes, but has the benefit of being a single-stage procedure.5,11 Cartilage defects involving the patellofemoral compartment present additional challenges for treatment and the ideal surgical technique is often not known. 12
New developments in cartilage restoration include the use of a cryopreserved osteochondral allograft. Cryo-preserved osteochondral allograft is composed of chondrocytes, chondrogenic growth factors and extracellular matrix proteins. Given its thin osseous portion it has similar indications to that of ACI, 13 but is typically used for smaller lesions 14 on the femur or patella in a 1-stage surgery. 7 It is potentially very suitable for treatment of cartilage defects within the patellofemoral compartment. Possible advantages compared to other cartilage procedures are the lack of donor site morbidity and the single-stage procedure using an off-the-shelf implant. It is reported to have the ability to be stored for over 2 years with maintained chondrocyte viability. 15 A single patient case study and an animal study have demonstrated effective treatment of full-thickness chondral defects with cryopreserved allograft. In both cases, histologic assessment showed hyaline-like repair tissue filling the defect within 1-year posttreatment.16,17 To our knowledge, there are currently no published outcomes of patients following surgical treatment of full-thickness cartilage defects using cryopreserved osteochondral allograft.
The purpose of this prospective case series study was to analyze the general health outcomes, knee function, and activity level of patients at minimum 2-year follow-up after treatment of full-thickness cartilage defects involving the patellofemoral compartment with cryopreserved osteochondral allograft (Cartiform, Osiris Therapeutics, Inc., Columbia, MD). The hypothesis was that the use of cryopreserved osteochondral allograft would result in reasonable clinical outcomes at minimum 2-year follow-up.
Materials and Methods
All operations were performed by experienced surgeons at 3 hospital sites. A prospective registry was implemented to collect outcomes on all patients undergoing cartilage restoration procedures. The registry was approved by our institutional review board (IRB ID# 15-000601) as well as the other hospitals’ institutional review board (IRB ID# 1612E02261) and (IRB ID# 0180). There were no external funding sources. All patients provided informed consent before participation. Patients were evaluated preoperatively and were prospectively followed postoperatively.
Inclusion Criteria
Patients were included if they had (1) a full-thickness cartilage defect of the trochlea of the femur or the patellar articular surface, (2) a surgical procedure using cryopreserved osteochondral allograft for treatment, and (3) minimum 2-year follow-up. Patients were excluded if they had (1) subchondral bone loss of more than 5 mm, (2) a femoral lesion with uncorrected malalignment, meniscal deficiency or ligament instability, or (3) an uncontained cartilage lesion. Once the inclusion criteria was met, most patients chose this treatment over others (i.e., ACI, OCA, OATS, microfracture) when they wished to undergo only 1 operation, hoped for repair with hyaline-like tissue, and wanted to avoid the risks and complications associated with the other options. They were informed of the lack of clinical data for this cartilage procedure.
Patients
Nineteen patients with full-thickness cartilage defects involving the patellofemoral compartment who were treated with a surgical procedure between the years 2014 and 2017 using cryopreserved osteochondral allograft were included in this study ( Table 1 ).
Patient Characteristics.
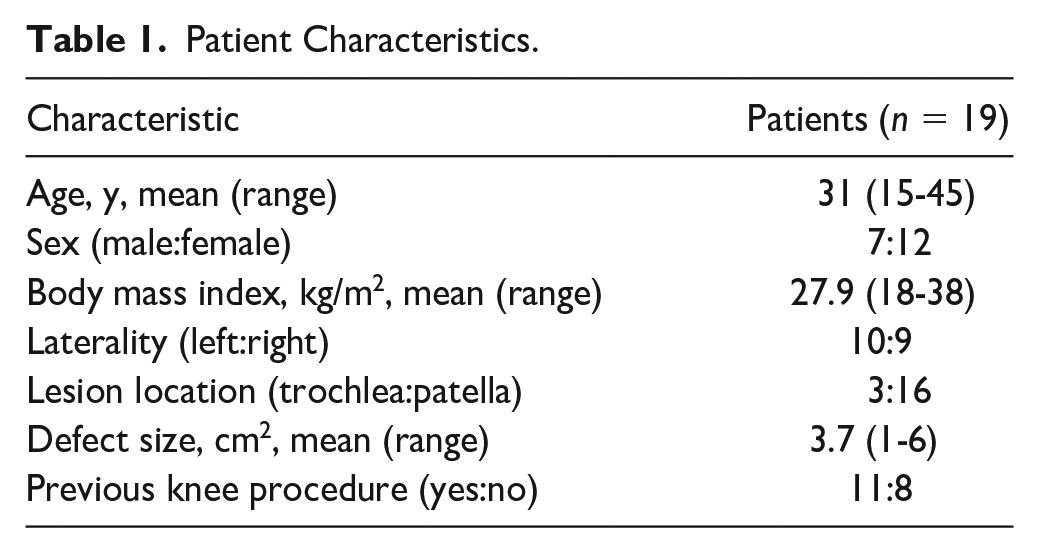
Seven patients were male and 12 were female. The average patient age at time of surgery was 31 years (range 15-45 years) and the average body mass index was 27.9 kg/m2 (range 18-38 kg/m2). Sixteen chondral defects were on the patella and 3 were on the femoral trochlea. One patient had a bipolar lesion of the patella and trochlea that was treated with 2 implants on the patella and a tibial tubercle osteotomy. Seventeen of the 19 patients in this cohort underwent a concurrent procedure to address coexisting pathology such as patellar maltracking or malalignment. Eleven patients had undergone previous procedures involving the operative knee ( Table 2 ).
Previous Procedures.
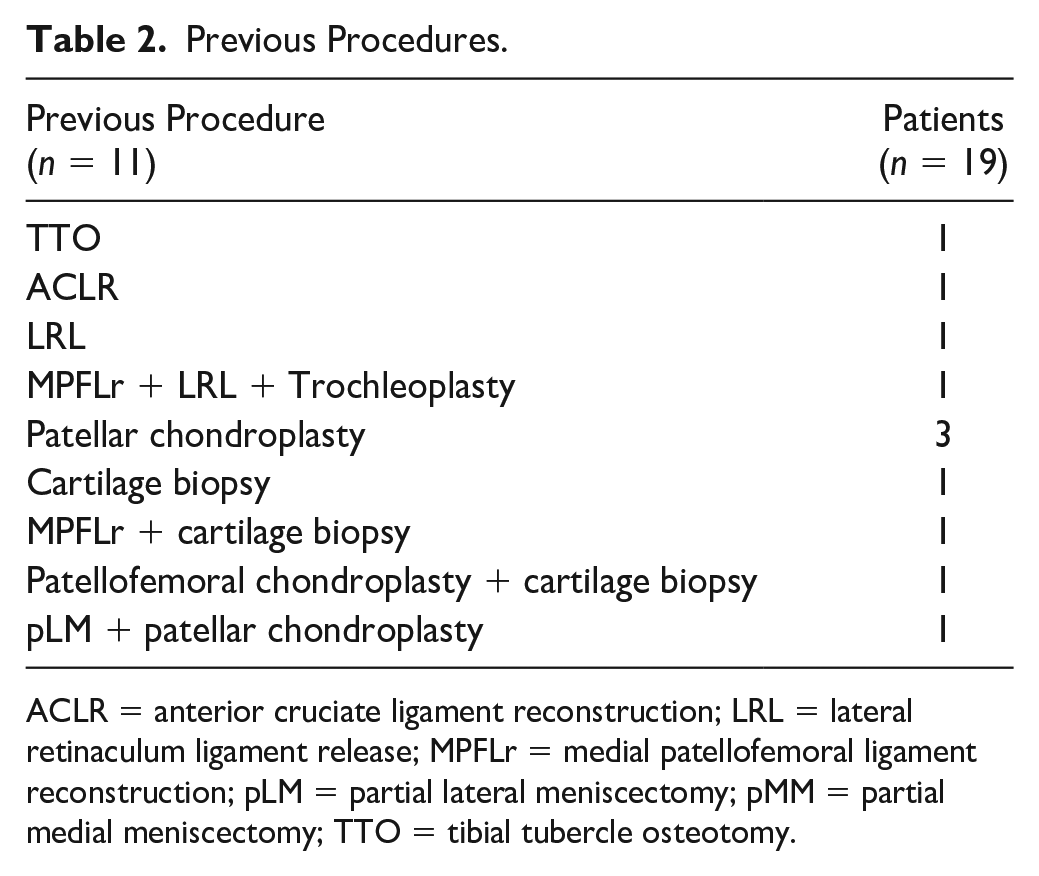
ACLR = anterior cruciate ligament reconstruction; LRL = lateral retinaculum ligament release; MPFLr = medial patellofemoral ligament reconstruction; pLM = partial lateral meniscectomy; pMM = partial medial meniscectomy; TTO = tibial tubercle osteotomy.
None of these were cartilage procedures other than chondroplasty or ACI biopsy only.
Graft Preparation
The cryopreserved osteochondral allografts implanted were harvested from human cadaveric specimens (Cartiform, Osiris Therapeutics, Inc., Columbia, MD). Cartiform is composed of full-thickness articular cartilage and a thin layer of subchondral bone that is tested for sterility and proper cellular composition. The fenestrated allograft allows for flexible conformity and improved integration to the underlying subchondral bone. The chondrocytes are placed in a type II collagen matrix along with extracellular matrix proteins, chondrogenic factors, and a thin osseous portion. They are cryopreserved at −80°C and can remain viable for up to 2 years.15,18,19
Surgical Technique
A diagnostic arthroscopy was performed on all patients to confirm a full-thickness, contained articular defect and to rule out concomitant pathology. All procedures were performed by surgeons with extensive cartilage restoration experience (JAM, MJS, JF, and AJK). The procedure has been previously published. 20 A 6- to 8-cm longitudinal incision was made over the medial or lateral third of the patella depending on the defect location, and a small parapatellar arthrotomy was performed. A No. 15 scalpel blade was used to sharply define the desired peripheral wall of normal cartilage to create a stable border. A curette was used to remove the pathologic cartilage and the calcified cartilage layer throughout the base of the defect ( Fig. 1A ). A 0.9-mm drill was inserted to a depth of 4 mm in multiple locations to access the bone marrow. Holes were initially created along the periphery of the defect followed by sequentially more central positions maintaining an osseous bridge of 2 to 3 mm between each drill hole. The cryopreserved osteochondral allograft implant was then placed over the defect with the bone side down ( Fig. 1B ) and marked for peripheral resection to fit the lesion.
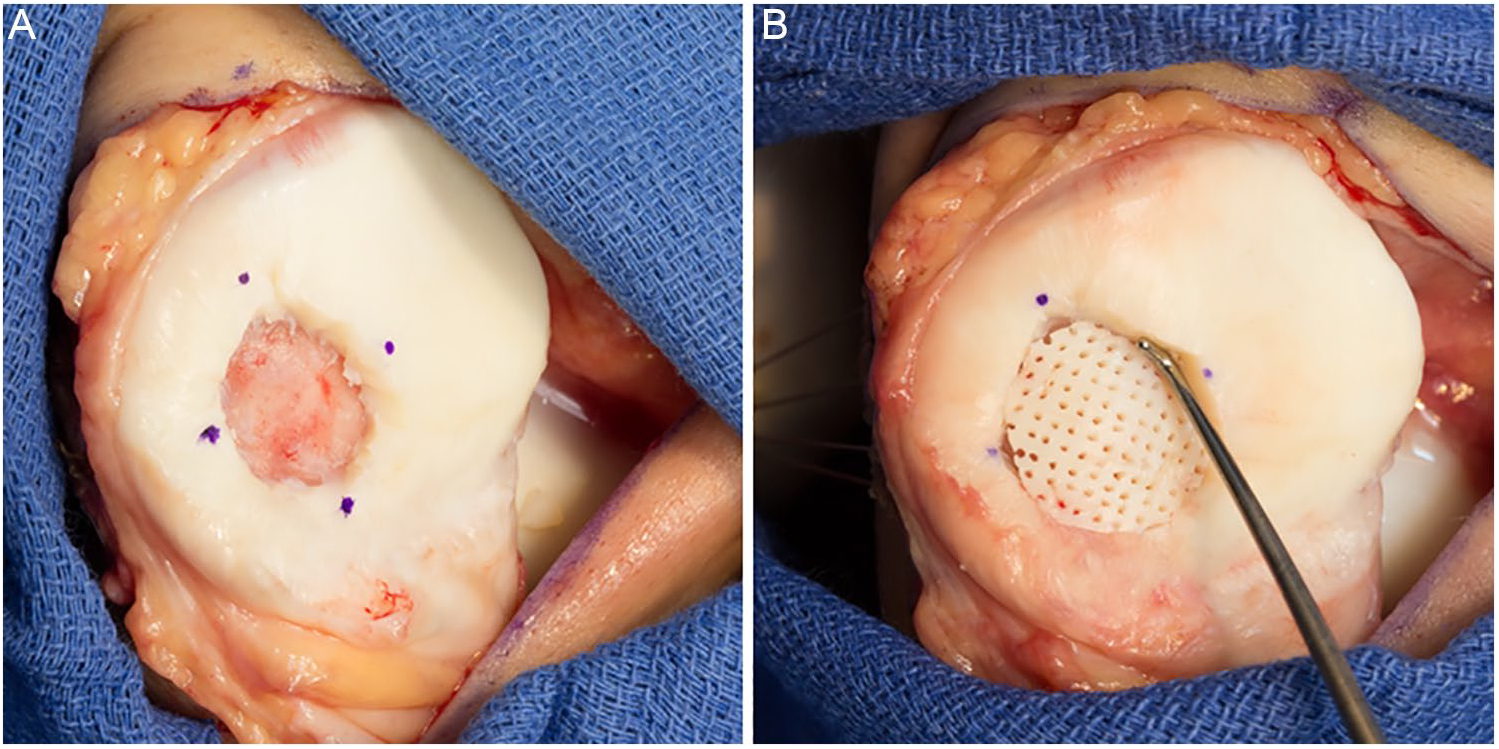
Images demonstrating a full-thickness cartilage defect of the patellar articular surface following removal of the pathologic cartilage with a curette (
4-0 Vicryl sutures were passed in mattress fashion in 4 quadrants of the implant in the location of the anticipated suture anchors. The implant was then anchored with knotless suture anchors (2.5 mm mini-PushLock anchors, Arthrex Inc., Naples, FL). If an unstable edge of the allograft implant was identified, it was secured to the normal cartilage rim with 6-0 absorbable suture. The tourniquet was deflated and the graft was covered with a thin layer of fibrin glue.
Postoperatively, patients were placed in a hinged knee brace and locked in full extension. All patients were kept partial weightbearing in full extension while wearing a knee brace for the first 6 weeks. They were allowed to begin immediate active and passive range of motion as tolerated. Patients began gradual weight bearing as tolerated and the brace was discontinued at 6 weeks after surgery. They were returned to activities as tolerated at four months after surgery.
Outcome Measures
The Veterans RAND 12-item Health Survey (VR-12) was used to assess and report patient general health and well-being. This patient reported outcome tool is made up of both physical and mental component scores, which are compared with a reference population.21,22 Patients were assessed prior to surgery and at postoperative follow-up. Knee function was assessed using the International Knee Documentation Committee (IKDC) subjective knee score and the Knee Injury and Osteoarthritis Outcome Score (KOOS). The IKDC has been shown to be a valid and reliable indicator of knee function 23 and is considered more applicable than KOOS in assessing patient symptoms following articular cartilage repair procedures. 24 Patients were assessed prior to surgery and at postoperative follow up. Patient activity level was assessed using the Tegner activity scale. 25 Patients were assessed prior to surgery and at postoperative follow-up. Graft incorporation was assessed in 9 patients. Three patients underwent second-look arthroscopy and 6 patients underwent magnetic resonance imaging (MRI). The magnetic resonance observation of cartilage repair tissue (MOCART) scoring system was used to report the graft incorporation details found on imaging. 26
Statistical Analysis
Descriptive analyses of the patient data were performed using means and standard deviations for continuous variables and means with ranges for ordinal variables. Comparisons of preoperative versus postoperative clinical scores were conducted using Wilcoxon rank-sum tests. A 2-tailed t test was used for all statistical analysis with a critical α set to 0.05. Analysis was performed using SAS Statistical Discovery JMP version 7.0 (SAS, Inc., Cary, NC).
Results
All 19 patients were treated between 2014 and 2016 with cryopreserved osteochondral allograft. All had at least 2 years of follow-up. The mean time to follow-up was 41.9 months (range 24-62 months). Baseline clinical scores are shown in Table 3 . Seventeen patients had a concurrent procedure ( Table 4 ).
Pre- and Postoperative Clinical Scores.
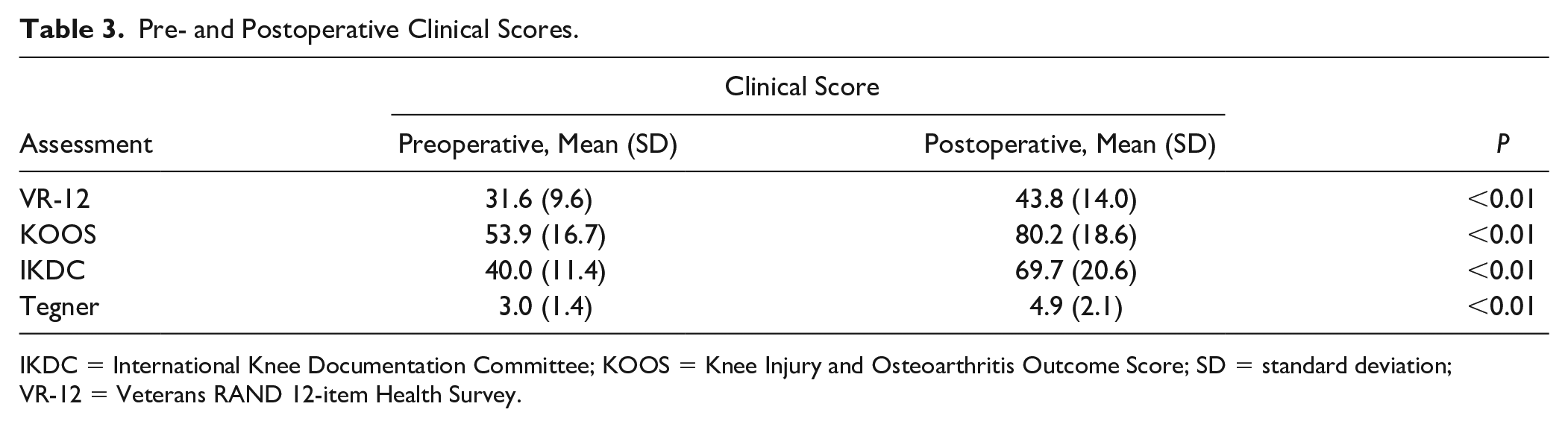
IKDC = International Knee Documentation Committee; KOOS = Knee Injury and Osteoarthritis Outcome Score; SD = standard deviation; VR-12 = Veterans RAND 12-item Health Survey.
Surgical Details.
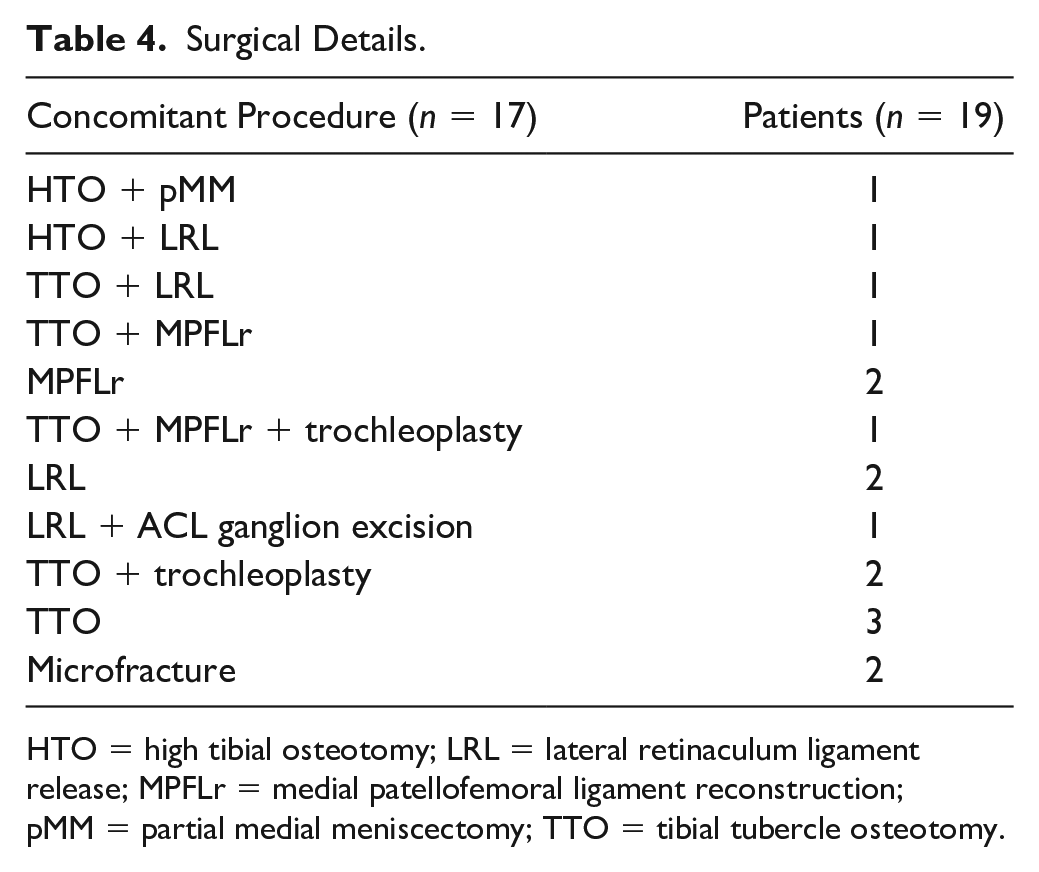
HTO = high tibial osteotomy; LRL = lateral retinaculum ligament release; MPFLr = medial patellofemoral ligament reconstruction; pMM = partial medial meniscectomy; TTO = tibial tubercle osteotomy.
Two patients required the use of 2 allografts for larger defect size while all others only used 1 allograft.
General Health Outcome
The mean VR-12 score improved significantly from baseline to postoperative follow-up (P < 0.01) ( Fig. 2 ).
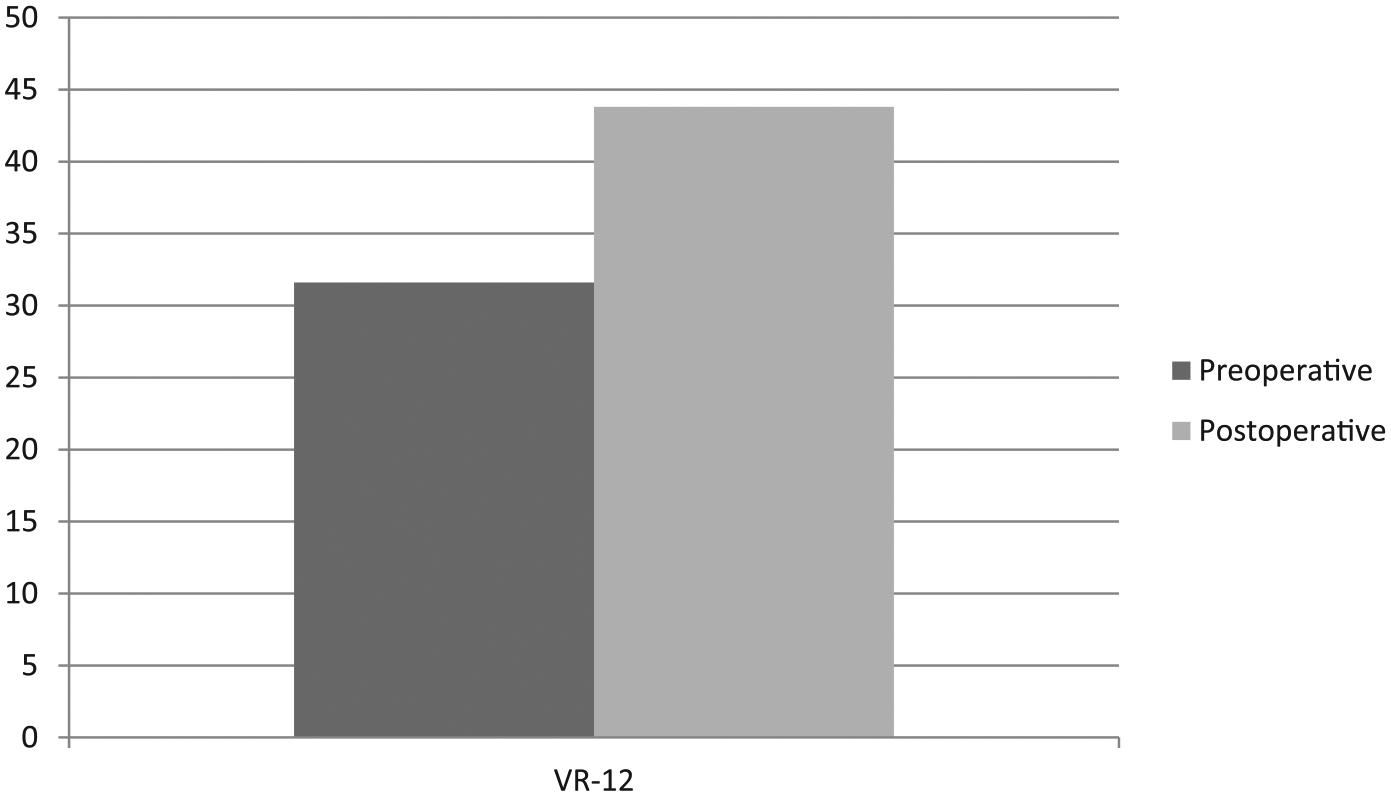
Pre- and postoperative clinical outcomes. VR-12 = Veterans RAND 12-item Health Survey.
Knee Function
The mean KOOS and IKDC scores improved significantly from baseline to postoperative follow-up (P < 0.01 for both) ( Fig. 3 ).
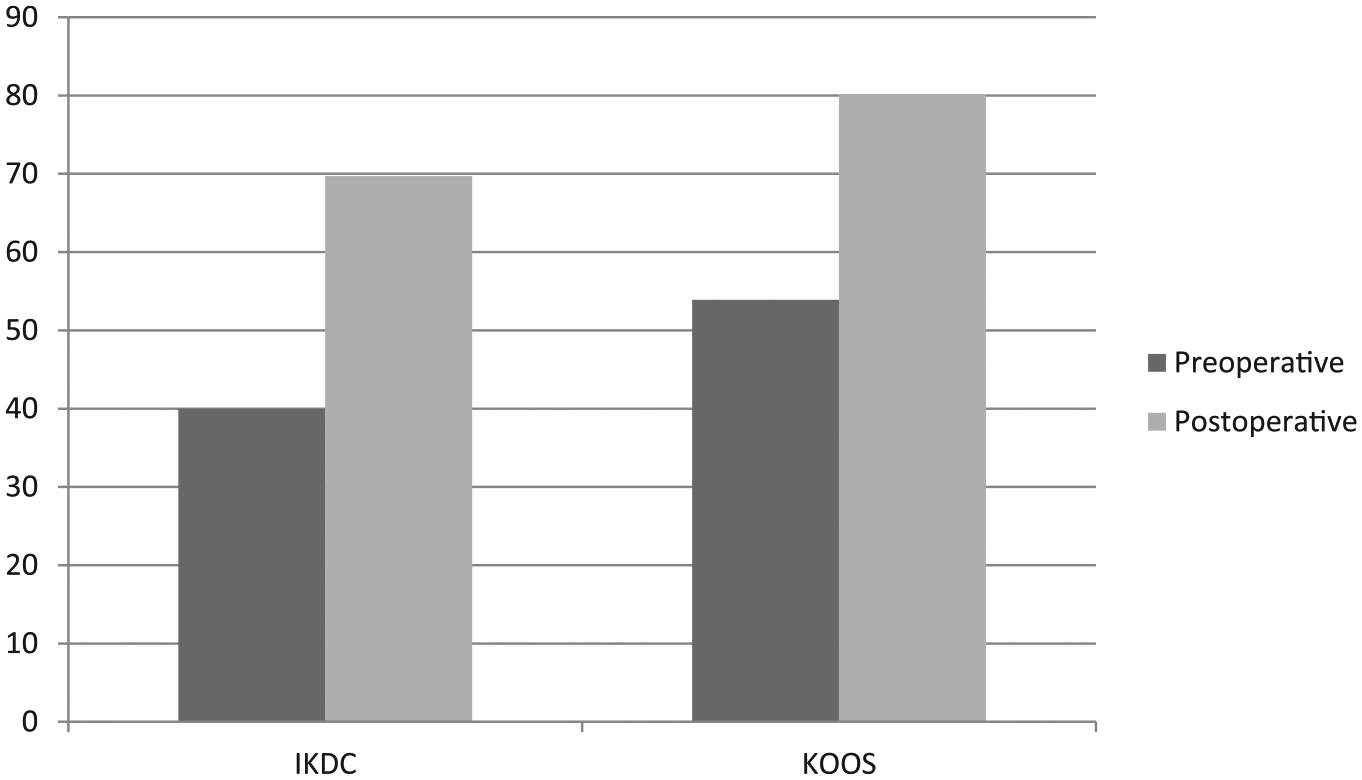
Pre- and postoperative knee function. IKDC = International Knee Documentation Committee; KOOS = Knee Injury and Osteoarthritis Outcome Score.
Activity Level
The Tegner score increased significantly from baseline to postoperative follow-up (P < 0.01) (
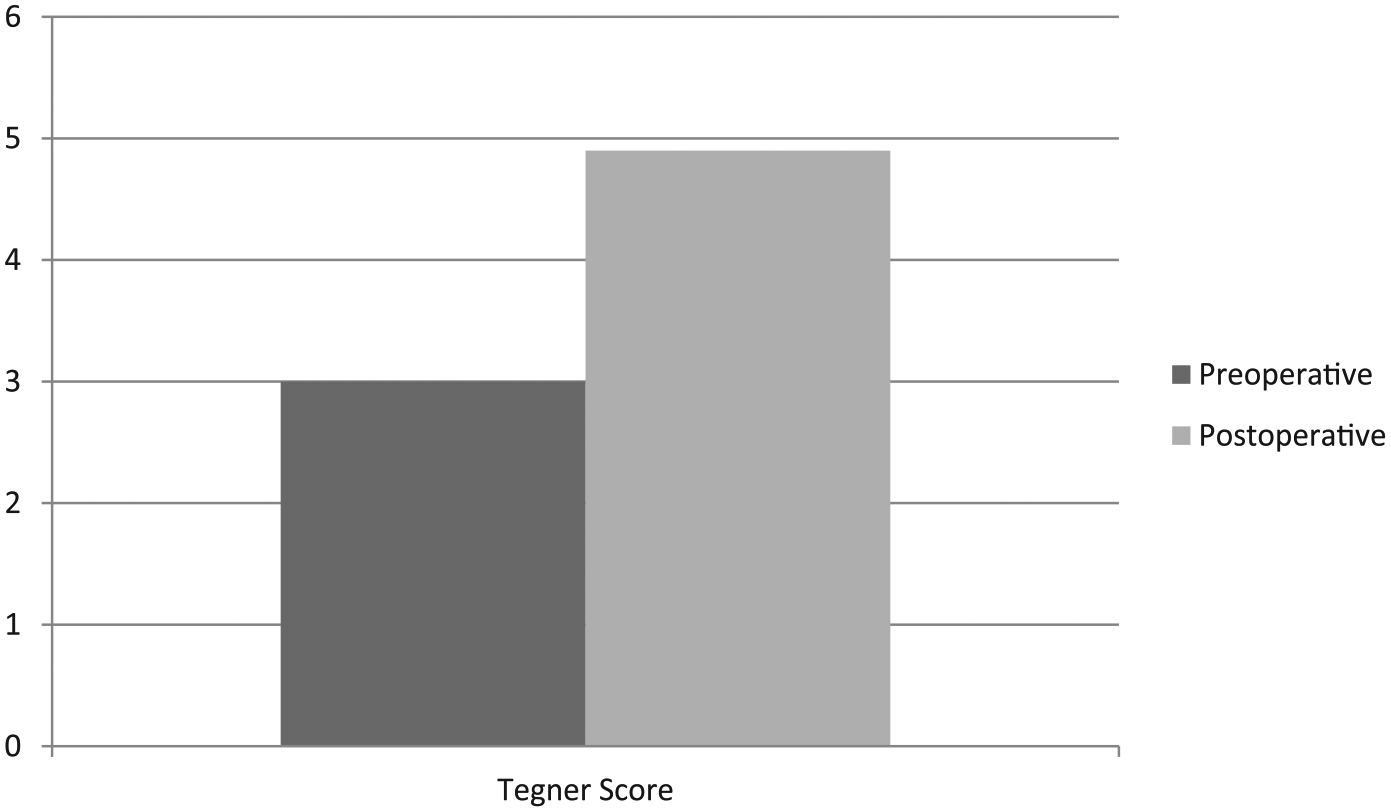
Pre- and postoperative activity level.
Graft Incorporation
Graft incorporation was evaluated by MRI or second-look arthroscopy on 9 patients. Six patients underwent follow-up MRI and 3 patients underwent second-look arthroscopy. On second-look arthroscopy at 8 weeks to 1 year postoperatively, all patients demonstrated a well-incorporated graft ( Fig. 5 ).
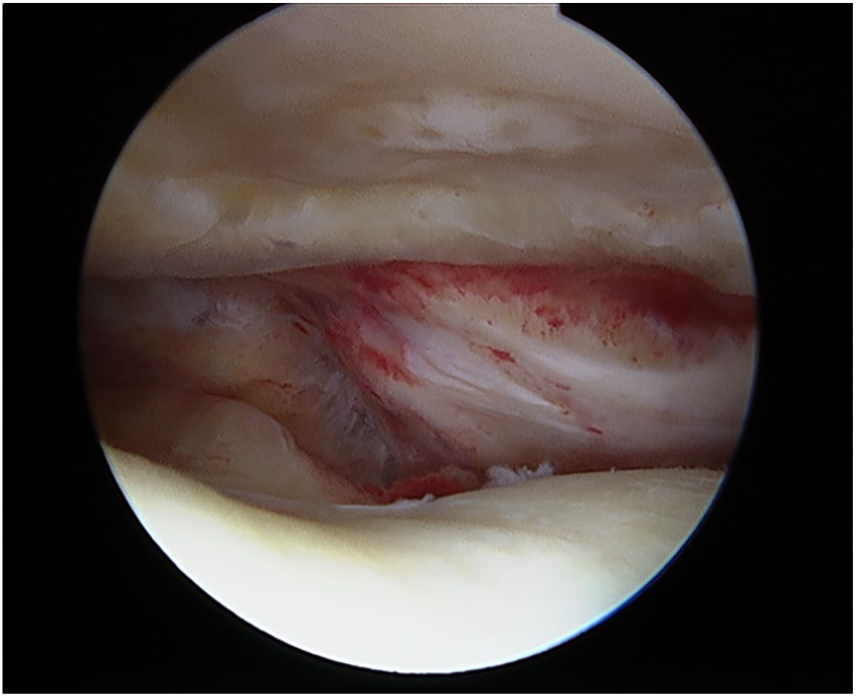
Arthroscopic image demonstrating a well fixated cryopreserved osteochondral allograft in the patella with intact opposing trochlear articular cartilage.
The mean MOCART score was 62.5 (range 25-85).
Complications and Failures
Two patients developed arthrofibrosis requiring arthroscopic lysis of adhesions at 2 and 3 months postoperatively. Both patients had concurrent procedures including tibial tubercle osteotomy (TTO) + trochleoplasty and medial patellofemoral ligament (MPFL) reconstruction, respectively. An additional patient developed painful tibial tubercle screws at 1-year postoperation and another required repeat arthroscopy with chondroplasty and partial meniscectomies at 42 months. Finally, 2 patients went on to failure with progressive patellofemoral osteoarthritis and were ultimately converted to a patellofemoral arthroplasty. One of these was the patient with a treated bipolar lesion. When including reasons related to concurrent procedures, such as hardware removal, the reoperation rate was 21.1%.
Discussion
Cartilage restoration options continue to evolve, but there is still no gold standard for treating patellofemoral defects. The purpose of this study was to analyze the general health outcomes, knee function, and activity level of patients at minimum 2-year follow-up after treatment of full-thickness cartilage defects involving the patellofemoral compartment of the knee with cryopreserved osteochondral allograft. Overall, this study demonstrates good clinical outcomes at minimum 2-year follow-up, with significant improvements in preoperative pain and function.
Currently, there is a paucity of research analyzing the clinical outcomes of patients treated with cryopreserved osteochondral allograft, but in vivo and in vitro studies have demonstrated promising results. A cryopreserved, viable osteochondral allograft was shown to heal osteochondral defects in a goat model. At 12 months, the defect was filled with highly cellular, hyaline-like repair tissue by histologic assessment. 16 Hoffman et al. 17 reported a case study where a patient with a femoral trochlea defect was treated with a 1 cm by 1 cm cryopreserved osteochondral allograft implant. At 9 months, the patient demonstrated full range of motion, reported no pain and had returned to sports. MRI showed that the graft was isointense compared with surrounding cartilage and repeat arthroscopy revealed a well-integrated graft. The graft site was biopsied and it demonstrated 85% hyaline cartilage.
In the present study, the VR-12 was used to assess and report patient general health and well-being as a measure of general health outcomes. The VR-12 scores increased significantly from baseline to postoperative testing. In a randomized trial comparing ACI and microfracture, Knutsen et al. 14 found a significant difference in general health outcome as measured by the 36-item Short Form Health Survey (SF-36) at 2-year follow-up. Microfracture showed more improvement than ACI. At 5 years, no difference was detected between the 2 procedures, although microfracture continued to show significant improvements. These improvements in general health are similar to those seen in the current study.
In the present prospective study, knee function improved significantly from baseline to postoperative follow-up as measured by KOOS and IKDC scores. IKDC has been shown to be very applicable in assessing patient symptoms following articular cartilage repair procedures. 24 Similar improvements in knee function have been seen following other treatment options for chondral lesions. Krych et al. 5 demonstrated significant improvements in IKDC scores for treatment of smaller cartilage lesions at 1, 2, 3, and 5 years postoperatively for both microfracture and OATS. At 1 year, IKDC scores improved from 43.7 to 71.8 and 49.7 to 65.4 for OATs and microfracture, respectively. Looking specifically at ACI for cartilage defects involving the patellofemoral compartment, Farr et al. 27 reported comparable postoperative improvements in subjective knee scores.
Activity level did increase significantly from baseline to postoperative follow-up in the present study. In a randomized trial 14 evaluating Tegner scores following ACI and microfracture at 5 years postoperation, significant improvements were seen. For ACI, mean Tegner scores increased from 3.3 to 4.1 and in the microfracture patients the scores increased from 3.2 to 4.4. The increases seen in this previous study evaluating other treatment options are comparable to those seen in this present study.
Graft incorporation was evaluated on 9 patients in this study. Three patients underwent second-look arthroscopy and all demonstrated well-incorporated grafts. Six patients underwent follow-up MRI and the MOCART scoring system was used to grade graft incorporation. Welsch et al. 28 and Trattnig et al. 29 reported MOCART scores of 70 (collagen-based scaffold used) at 2 years and 73 at 1 year. The mean score in this present study was comparable but slightly less than that of the studies evaluating ACI.
Although improvements in postoperative knee function scores and activity level were appreciated, the reoperation rate was high at 21.1% and 2 (12.5%) patients were converted to patellofemoral arthroplasty. One was converted to arthroplasty at 53 months postoperatively at the age of 37 years. The other patient developed progressive patellofemoral osteoarthritis postoperatively and was ultimately converted 2 years postoperatively. This patient was 20 years old and had bipolar lesions. Because of her young age and significant symptoms, it was decided to attempt treatment using the cryopreserved osteochondral allograft; however, the presence of bipolar lesions may be a relative contraindication to the use of cryopreserved osteochondral allograft. The 3 other complications, including 2 patients with arthrofibrosis and 1 with painful hardware, may be related to concurrent procedures rather than the allograft implantation.
Cryopreserved osteochondral allograft also has potential limitations to use. It is relatively restricted to lesions less than 2 cm in diameter as this is currently the largest implant available. However, multiple implants can be used if necessary. Given its thin osseous portion, the allograft cannot be used in lesions with significant subchondral bone loss as these typically require treatment with traditional fresh-stored OCA. 30
The results of this study should be considered with its limitations. The series consisted of a rather small number of patients, but this is because of the fact that this is a relatively new procedure and has only been performed at our institution since 2014. There was a high percentage of concurrent procedures in this series, which is a confounding variable, but this is standard in cartilage restoration surgery. In fact, Brophy et al. 12 discuss the necessity of concurrent operations in their review of patellofemoral compartment cartilage restoration options. Nevertheless, the improvements appreciated in this study likely cannot be completely attributed to the presented technique as the majority of patients underwent a concurrent realignment procedure. It is known that realignment procedures may be performed in isolation for the treatment of patellofemoral cartilage lesions. 31 There was no control and the patients were not randomized. Despite its limitations, to our knowledge this is the first study evaluating the 2-year minimum outcomes in patients following treatment with cryopreserved osteochondral allograft.
In conclusion, patients with unipolar cartilage defects involving the patellofemoral compartment of the knee can have positive outcomes at minimum 2-year follow-up after surgical treatment with a cryopreserved osteochondral allograft when concomitant pathology is also addressed, but the reoperation rate is high and bipolar cartilage lesions may increase the failure rate.
Footnotes
Investigation performed at the Mayo Clinic, Rochester, MN; University of Minnesota, Minneapolis, MN; and OrthoIndy Hospital, Greenwood, IN.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The registry was approved by our institutional review board (IRB ID# 15-000601) as well as the other hospitals’ institutional review board (IRB ID# 1612E02261) and (IRB ID# 0180).
Informed Consent
All patients provided informed consent before participation.
Trial Registration
Not applicable.