
Abstract
Background:
The optimal surgical treatment of delayed avulsion fractures of the posterior cruciate ligament (PCL) is still controversial.
Purpose:
To evaluate the clinical results of arthroscopic suture fixation of tibial avulsion fractures of the PCL with autograft augmentation reconstruction.
Study Design:
Case series; Level of evidence, 4.
Methods:
From January 2013 to February 2017, we treated 15 patients with delayed tibial avulsion fractures of the PCL arthroscopically through posteromedial and posterolateral portals. The PCL and avulsion bone fragment were fixed with No. 2 nonabsorbable FiberWire sutures that were pulled out through a single tibial bone tunnel and fixed on a small Endobutton. Concomitantly, anatomic PCL augmentation reconstruction was performed, and the graft was pulled out through the same tunnel and fixed with an interference screw. Knee stability was assessed using the posterior drawer test, and the side-to-side difference was determined using a KT-1000 arthrometer with 134 N of posterior force at 30° of knee flexion. The International Knee Documentation Committee (IKDC) 2000 subjective form and Lysholm scale were used to evaluate clinical outcomes at follow-up. Overall, 12 patients were enrolled for analysis. The mean follow-up period was 34.4 months (range, 26-49 months).
Results:
At the final follow-up, 2 patients encountered 10° terminal flexion limitations. All patients had negative posterior drawer test results. The KT-1000 arthrometer side-to-side difference was significantly decreased from 8.25 ± 1.96 mm preoperatively to 1.08 ± 0.86 mm at the last follow-up (P < .001). The mean IKDC and Lysholm scores, respectively, increased from 54.67 ± 7.13 and 53.50 ± 7.90 preoperatively to 91.13 ± 3.78 and 94.25 ± 3.32 at the final follow-up (P < .001 for both).
Conclusion:
Arthroscopic suture fixation with autograft augmentation reconstruction for delayed tibial avulsion fractures of the PCL showed good clinical stability and function in this study.
Keywords
Residual knee laxity of posterior cruciate ligament (PCL) avulsion fractures is often attributed to fracture nonunion. 13 When a bone fragment is avulsed and displaced, nonoperative treatment is invalid, as reported by a nonunion rate of 80%. 13 Many authors advocate operative treatment of a PCL tibial avulsion fracture if the bone fragment emerges above the joint line on lateral knee radiographs and the fracture has been displaced more than 5 mm on magnetic resonance imaging (MRI). 4,16 However, the optimal surgical treatment of isolated PCL tibial avulsion fractures remains controversial. In some cases, a large fragment can be anatomically reduced and held with a screw though an open posterior approach. 8,13 When the fragment is comminuted or too small to accommodate a screw, suturing the ligament in position arthroscopically is also a good treatment option. 4,8,16
Another reason for residual knee laxity may be that the PCL had been stretched at the time of injury and that the mechanical properties of the ligament were reduced. 6,7 Some authors have reported that a certain percentage of their patients still had significant knee instability even though the bone fragment had been anatomically reduced and rigidly fixed in the treatment of PCL avulsion fractures. 6,7
In spite of acute tibial avulsion fractures of the PCL being widely reported, 4,16 delayed avulsion fractures also occur because of a neglected diagnosis or the failure of nonoperative treatment. 4,8 Arthroscopic suture fixation for delayed PCL avulsion injuries is considered a complex orthopaedic intervention because scar conglutination and bony callus formation complicate the anatomic structure and result in avulsed fragment malreduction. 1,9 The purpose of the present study was to evaluate the efficacy and clinical results of arthroscopic suture fixation with autograft-enhanced reconstruction for delayed tibial avulsion fractures of the PCL.
Methods
This was a retrospective case series study. Institutional review board approval was obtained to perform this study. From January 2013 to February 2017, a total of 15 consecutive patients with delayed tibial avulsion fractures of the PCL were treated by arthroscopic suture fixation with anatomic PCL reconstruction. Of those included, 3 patients were lost to follow-up: 2 changed their contact information, and 1 patient was unwilling to be reviewed because she lived too far away. The other 12 patients (8 male and 4 female) were followed up for more than 24 months (mean, 34.4 months [range, 26-49 months]).
Standard anteroposterior and lateral radiographs and computed tomography scans were routinely obtained to verify the diagnosis (Figure 1). MRI was performed preoperatively to better evaluate concomitant intra-articular injuries.

Preoperatively, (A) an anteroposterior radiograph showed that a large bone fragment was avulsed from the tibial eminence (red arrow), and (B) bony callus formation was seen on a computed tomography scan in the posteroanterior view (yellow arrow).
The indication for surgery was that the elevated bone fragment was above the joint line on lateral radiographs, with a more than 5-mm displacement on MRI. Patients with tibial plateau fractures, osteochondral lesions, and anterior cruciate ligament or multiligament injuries were excluded. Patients treated with meniscal partial resection or suture repair at the same time were not excluded.
The mean time from injury to surgery was 37.8 ± 10.2 days (range, 27-61 days). The posterior drawer test was performed under anesthesia before surgery. The KT-1000 arthrometer (MEDmetric) side-to-side difference was measured with 134 N of posterior force at 30° of knee flexion to evaluate posterior displacement of the knee. Lysholm and International Knee Documentation Committee (IKDC) 2000 scores were also recorded before surgery, at 3 and 6 months postoperatively, and yearly thereafter.
Surgical Procedures
All surgical procedures were completed by the same team of 3 experienced orthopaedic surgeons (Q.B., C.Z., M.B.). The patient was placed in the supine position under general anesthesia, and a support pad was placed next to the proximal femur to keep the bended knee stable. Standard anteromedial and anterolateral portals were established, and diagnostic arthroscopic surgery was performed. Then, an arthroscope was inserted from the interval between the PCL and the medial condyle of the femur. An additional posteromedial portal was established, and a switch stick was passed through this portal, viewing from the anterolateral portal, and inserted toward the posterolateral space through the posterior septum. After that, an additional posterolateral portal was established via an outside-in technique, viewing from the additional posteromedial portal.
Partial debridement of the posterior septum was performed until the PCL was exposed. The avulsed fragment was reduced by a probe to regain tension of the PCL after debridement of scar tissue and bony callus in the posterior articular cavity (Figure 2A). A 45° SutureLasso (Arthrex) was passed through the front region of the base of the PCL from the posteromedial portal, while the posterolateral portal was used to observe. Then, a No. 2 nonabsorbable FiberWire suture (Arthrex) was pulled into the knee, and the same sequence was performed to encircle the PCL at least 2 times (Figure 2B). After that, a 7-mm tibial tunnel was established using a 55° PCL tibial guide underneath the bone fragment (Figure 2C), and the ends of the FiberWire suture were pulled forward from the tunnel. Approximate anatomic reduction was achieved by pulling down the 2 ends of the FiberWire suture. The suture was tied on a small Endobutton (Smith & Nephew) at 60° of knee flexion and with tibial anterior translation to decrease tension of the PCL and reduce the fragment.

Left knee and view from the posterolateral portal. (A) Scar tissue and bony callus were totally removed to expose the bony bed of the avulsion fragment. (B) The FiberWire suture was used to bundle the neck of the posterior cruciate ligament (PCL) by a lasso. (C) A small distal tibial bone tunnel was created to allow sufficient fracture reduction. B, fracture bed; F, avulsion bone fragment; T, bone tunnel.
We used a folded autograft from the semitendinosus and gracilis for enhanced reconstruction. The mean diameter of the graft was 7 mm, and the mean length was 11 cm (range, 10-12 cm). The femoral tunnel was drilled on the medial femoral condyle based on the identified PCL footprint through the anterolateral portal with 90° of knee flexion. The center of the tunnel was placed at the anterolateral bundle and posteromedial bundle junction site (Figure 3A). During the process of the graft being pulled into the tibial bone tunnel, the 2 ends of the FiberWire suture were pulled tightly to tension the PCL (Figure 3B). Usually, we tried to make the substance of the graft lie above the avulsion fragment to obtain a downward force when we pulled and fixed the tibial-side autograft after we pulled the graft into the femoral tunnel at least 20 mm. A TightRope (Arthrex) and 7 × 25–mm interference screw were, respectively, used to fix the grafts on the femoral and tibial sides (Figures 4 and 5).

Left knee and view from the anteromedial portal. (A) The center of the tunnel was placed at the anterolateral (AL) bundle and posteromedial (PM) bundle junction site. (B) The FiberWire suture was tightly tensioned when the autograft was introduced into the bone tunnels. FB, FiberWire suture.
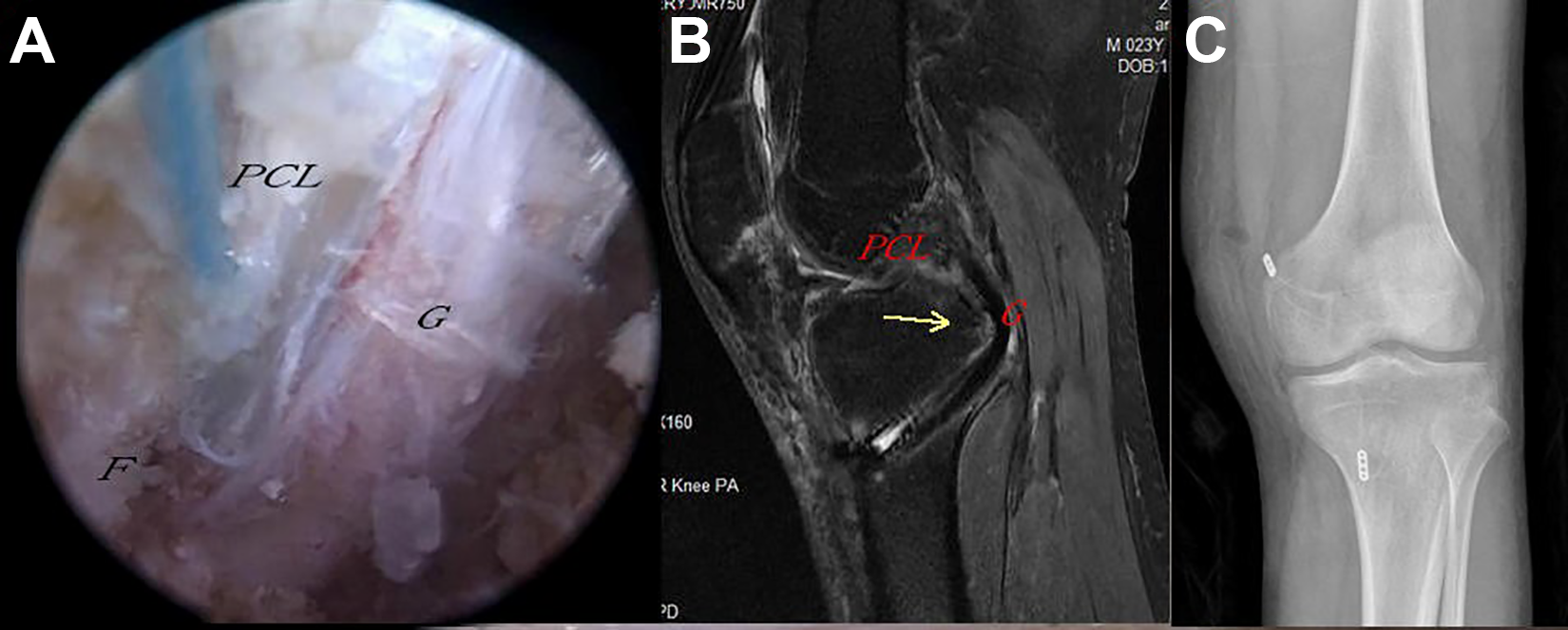
Left knee and view from the posterolateral portal. (A) Arthroscopic suture fixation with anatomic autograft augmentation reconstruction was achieved. (B) The bone fragment (yellow arrow) was sufficiently reduced and pressured by the graft. An interference screw was used to fix the graft. (C) An Endobutton at the tibial side was used to tension the FiberWire suture (anteroposterior view immediately after surgery). F, avulsion bone fragment; G, autograft; PCL, posterior cruciate ligament.

Schematic drawings of suture fixation and autograft augmentation reconstruction of a bone fragment. (A, B) The FiberWire suture (black arrow) was used to encircle the posterior cruciate ligament, and then the ends of the FiberWire suture were pulled forward from the tibial tunnel. Approximate anatomic reduction was achieved by pulling down the 2 ends of the FiberWire suture, and the suture ends were tied on a small steel plate to fix the bone fragment. (C) Then, autograft augmentation reconstruction was performed. The substance of the graft lay above the avulsion fragment to obtain a downward force. An interference screw was used to fix the graft in the same tibial tunnel. BF, bone fragment; G, graft; P, steel plate; PCL, posterior cruciate ligament; S, interference screw; T, bone tunnel.
Postoperative Protocol
Ice was used immediately after surgery to decrease surgical swelling and pain. The key point of the early rehabilitation protocol was to protect against PCL tension. During the first 4 weeks, the involved knee was kept in full extension in a hinged knee brace. A small cushion was put in the brace under the lower leg to prevent tibial posterior translation, which increased tension of the autograft. Straight-leg raising exercises were strictly limited during the immobilization process and were replaced by ankle pump exercises and isometric quadriceps contractions as a precaution against disuse atrophy. Continuous passive motion was allowed at 3 weeks to prevent postoperative stiffness. For the next 4 weeks, the brace was adjusted to permit motion from 0° to 90°, and partial weightbearing with crutches was initially allowed at 6 to 8 weeks. The brace was routinely continued for 3 months. Weightbearing walking with the brace unblocked was allowed from 12 weeks after surgery. Yet, return to sports was not recommended until at least 12 months after surgery.
Follow-up
Patients were followed up at 4 weeks, 6 weeks, 3 months, 6 months, and annually thereafter, during which they were evaluated using the IKDC form and Lysholm scale. All clinical evaluations were performed by 2 independent observers who were blinded to the surgical procedure (Z.H., J.C.). PCL laxity was classified into 4 levels: grade 0, 1-2 mm; grade I, 3-5 mm; grade II, 6-10 mm; and grade III, >10 mm. The KT-1000 arthrometer side-to-side difference was determined with 134 N of posterior force at 30° of knee flexion to evaluate posterior displacement of the knee. The medical record for each patient was reviewed for any postoperative complications or reoperations.
Statistical Analysis
Continuous variables were described as mean ± standard error and assessed using a paired t test (normally distributed). For analyses, a 2-sided P value <.05 was considered significant.
Results
Demographics of Enrolled Patients
The demographic information of the 12 study patients is summarized in Table 1. There were 9 patients who initially underwent nonoperative treatment. However, the fracture still had more than 5 mm of displacement on MRI after nonoperative treatment. In the remaining 3 patients, the injury was initially misdiagnosed from radiographs by local hospital doctors (Table 1). Dysfunction and instability of the involved knee were the main complaints of all patients at the time of the subsequent visit.
Patient Demographics a

a F, female; LM, lateral meniscus; M, male; MM, medial meniscus; MVA, motor vehicle accident; SRA, sports-related activity.
Clinical Findings
Imaging
The fracture fragments were usually shown to have healed according to radiographs at 10 to 15 weeks (mean, 3.2 months) postoperatively. No failure of fixation, refracture, or PCL rupture was found at follow-up.
Knee Range of Motion
Postoperative arthrofibrosis occurred in 9 patients at 3 months after surgery. At 1-year follow-up, 7 patients recovered to a normal range of motion of the knee when compared with the healthy side. Yet, the other 5 patients had various degrees of arthrofibrosis, with 10°, 15°, 15°, 20°, and 30° terminal flexion limitations. Rehabilitation was encouraged, and no arthroscopic release was performed. At the last follow-up, among those with initial flexion limitations, 3 patients returned to a normal range of motion of the knee. The remaining 2 patients still had 10° terminal flexion limitations but no complaints of any discomfort from daily activity.
Stability
Before surgery, 8 patients had 1° positive posterior drawer test results, and 4 patients had 2° positive results. We measured only knee posterior displacement from the resting position by using the KT-1000 arthrometer. The KT-1000 arthrometer showed that the side-to-side difference was 6 to 14 mm (mean, 8.25 ± 1.96 mm). At the last follow-up, all patients had negative posterior drawer test results. The KT-1000 arthrometer showed that the side-to-side difference was 0 to 3 mm for all 12 patients (mean, 1.08 ± 0.86 mm). This change was statistically significant (P < .001) (Table 2).
Clinical Results Preoperatively and at Last Follow-up a

a Data are presented as mean ± SD (range) unless otherwise specified. IKDC, International Knee Documentation Committee.
Knee Function
At the last follow-up, the mean IKDC score was 91.13 ± 3.78, and the mean Lysholm score was 94.25 ± 3.32, significantly improved from the baseline of 54.67 ± 7.13 for the IKDC score and 53.50 ± 7.90 for the Lysholm score (P < .001). The preoperative data and results at the last follow-up are summarized in Table 2.
Complications
No complications such as donor site morbidity, infection, thrombosis, bony nonunion, neurovascular injury, or implant failure were encountered during follow-up.
Discussion
The major finding of our study was that arthroscopic suture fixation with autograft augmentation reconstruction for patients with delayed tibial avulsion fractures of the PCL showed good clinical stability and function. In spite of acute tibial avulsion fractures of the PCL being widely reported, 16 delayed avulsion fractures of the PCL are not rare. 4,8,9 The reason for delayed surgery is often a neglected diagnosis or noneffective nonoperative treatment. To the best of our knowledge, operative procedures for delayed bone fragments are more difficult under arthroscopic surgery in terms of ligament retraction and fibrosis. 8 Potential factors are as follows: first, callus formation around the fracture makes the bone bed uneven. Microstep of the fracture line indicates malreduction of the fragment, making anatomic reduction troublesome. Second, the bone fragment of PCL avulsions is located deep within the posterior tibial plateau, so it is technically challenging to operate through arthroscopic surgery because the surgeon cannot manipulate across the board under direct vision as with an open approach. Third, as Inoue et al 6 reported, plastic deformation of the PCL still contributes to residual knee instability, even though the avulsion bone fragment has been anatomically fixated. Based on biomechanical tests, stress deprivation created by plastic deformation may reduce the mechanical properties of the ligament. 10
For avulsion fractures of the PCL, a surgical intervention is advocated if the bone fragment emerges above the joint line on lateral knee radiographs and exceeds more than 5-mm displacement on MRI. 4,16 Fixation of the bone fragment can be performed by using screws, toothed plates, Kirschner wires, and sutures. 8,11,15 Recently, suture fixation was used in arthroscopic surgery of PCL avulsion fractures, and good postoperative outcomes were reported. 5,17 Nonabsorbable suture fixation can have many advantages. First, suture fixation for an avulsion fracture of the tibial spine or plateau is elastic and also netlike, which is superior to rigid fixation, especially in some comminuted fracture cases 13 and in adolescents whose epiphysis is not closed. 14 Moreover, hardware needs to be removed with a second operative procedure.
We believe that arthroscopic suture fixation is a useful method to fix avulsion bone fragments. However, because suture fixation is an elastic fixation procedure as opposed to rigid fixation, we worried that suture fixation alone would not be enough for delayed tibial avulsion fractures of the PCL. First, compared with acute avulsion fractures, arthroscopic surgical treatment of delayed avulsion fractures of the PCL is considered to be a relatively difficult procedure to obtain anatomic reduction. In addition, on the basis of previous clinical observations, we found that delayed avulsion fractures of the PCL had a longer healing time than acute injuries. Second, the PCL itself has higher intrinsic tension than the anterior cruciate ligament. 3 Thus, the fragment may encounter much shear force when functional exercise is started. Thus, we performed an augmented reconstruction procedure for delayed avulsion fractures of the PCL based on 2 considerations. On one hand, the graft provides additional downward pressure to help fix the bone fragment. On the other hand, establishing a new bone tunnel provides a blood supply to promote healing.
Arthroscopic suture fixation with tibial tunnel techniques has been successfully performed by many surgeons, although the design of the established bone tunnel has varied. Zhao et al 16 used Y-shaped tibial bone tunnels, Kim et al 12 used a double bone tunnel, while Gui et al 4 used a single bone tunnel. Although good clinical outcomes and postoperative knee stability were attained in these studies, we believe that it may be needlessly complicated to establish double or Y-shaped tunnels to shuttle the sutures via arthroscopic surgery when compared with a single tibial tunnel. 4 In addition, complications of arthrofibrosis may increase when expanding the operative procedure. 4 In the study by Gui et al, the authors used only 2 posteromedial portals to create a single bone tunnel to fix the avulsion bone fragment, and at the last follow-up, the KT-1000 arthrometer side-to-side difference was 0 to 2 mm in 96% (23/24) of patients, and there was no statistical difference between the preinjury and postoperative Tegner activity score.
Compared with the single bone tunnel technique by Gui et al, 4 we have introduced some improvements. First, in contrast to their 2 posteromedial portals, we used a posteromedial portal and a posterolateral portal to fix the bone fragment. Because the posterior knee compartment is relatively narrow, creating 2 portals on the same side may cause crowding and interfere with manipulation of the instruments. Second, Gui et al stated that the high posteromedial portal that they used was helpful in viewing the PCL insertion site, but the posteromedial portal may be suboptimal because it is realistically difficult to view the overall perspective of the posteromedial compartment from the same side. The posterolateral trans-septal portal that we used seems to provide a broader arthroscopic view. Third, instead of suture shuttling from the posteromedial and anterolateral sides, we reduced the steps for suture passage, using only 1 step to pass the suture from the posteromedial side to the tibial bone tunnel. Although we used a more simplified technique to fix the PCL, the clinical outcomes of the IKDC score, the Lysholm score, and knee stability of patients in our study were comparable with those of Gui et al and Zhao et al. 16 We thus provide a simple, convenient, reliable, and microinvasive method to treat tibial avulsion fractures of the PCL.
This study has some limitations. First, the sample size in the present study was relatively small, which may increase the possibility of type II errors. Second, we used the posterior drawer test as a method to evaluate laxity of the PCL. This is a subjective test that is prone to interexaminer variation. In addition, we used the KT-1000 arthrometer to measure simple posterior displacement of the knee from the resting position. Measurement bias is a possibility, as posterior sag of the tibia at the resting position was not accounted for. 2 Thus, total anteroposterior displacement would be more meaningful than simple posterior displacement. 2 Third, an important limitation is that there was no radiological follow-up such as MRI, an imaging parameter. Moreover, this was a case series study with no comparison group. Thus, subgroup analysis was not possible.
Conclusion
In the current study, arthroscopic suture fixation with autograft augmentation reconstruction for delayed tibial avulsion fractures of the PCL showed good clinical stability and function.
Footnotes
Acknowledgment
The authors express their sincere gratitude to Jieling Fang for her linguistic assistance during the preparation of the revised article. In addition, they thank all of the patients who agreed to participate, who made the completion of this study possible.
Final revision submitted March 10, 2020; accepted March 19, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of Zhejiang Provincial People’s Hospital.