
Abstract
Keywords
Introduction
The posterior cruciate ligament (PCL) is one of the major ligaments of the knee joint to stabilize the tibia on the femur. It is estimated that the morbidity of PCL can reach 3%–23%.1,2 As a special type of PCL injury, avulsion fracture of the tibial insertion of PCL is relatively rare. At present, surgery is recommended for the treatment of the displaced avulsion fracture of the tibial insertion of PCL.3,4 It is well accepted that both the conventional open posterior surgery and arthroscopic reduction and internal fixation (ARIF) can clinically achieve the therapeutic purpose. However, there are still controversies concerning the choice of different surgical methods.3,5
Compared with traditional open posterior surgery, ARIF allows simultaneous treatment of combined intra-articular injuries.3,4 Moreover, for the surgical treatment of the avulsion fracture of the smaller bone pieces, ARIF has considerable advantage.6,7 However, the involved operation is relatively complicated with a long learning curve as well as high requirements of arthroscopic technique, which limits the application of ARIF for the treatment of avulsion fracture.8,9 Therefore, we have improved the existing arthroscopic high-strength fixation for the treatment of the avulsion fracture of the tibial insertion of PCL. Additionally, we retrospectively analyzed 16 cases of PCL tibial avulsion fracture in 15 patients who underwent the improved arthroscopic high-strength suture fixation.
Patients and methods
Patients
A total of 15 patients with PCL avulsion fracture were included in this retrospective study. They underwent high-strength suture fixation under arthroscopy in our hospital from December 2017 to November 2019. There were 16 cases of PCL avulsion fracture. According to the Meyers-McKeever classification, the 16 cases were divided into Type II group (2 cases) and Type III group (14 cases). All patients underwent arthroscopic high-strength suture fixation, and the procedure was shown in Figure 1. Conservative treatment was applied to the patients with medial and lateral collateral ligament injuries. The procedure of high-strength suture fixation under arthroscopy. (a) Intraoperative positioning of the posterior medial high and low approach; (b) The view of the avulsion fracture; (c) The view of the tibia bed; (d) The view of the reduced and fixed bone. The red arrow points to the blue fixed suture.
Surgical methods
After general anesthesia, the patient was placed in a supine position. A pelvic fixator was installed outside the tourniquet. A pillow was placed at the end of the operating bed. Routine disinfection and draping were conducted in the operating area.
Examination of the anterior internal and anterolateral knee joints were conducted for the treatment of co-occurring injuries. The median approach to the knee patella was prepared for the insertion of the arthroscope. The shaving instrument was inserted through the lateral approach. The spatium between anterior and posterior cruciate ligaments was opened followed by opening the posterior median septum to facilitate the entrance of the arthroscope to the posteromedial compartment. The arthroscope was inserted through the anterolateral approach with the assistant of 1.5 mm Kirschner wire for precise positioning. The arthroscope was extended to the opening between the anterior and posterior cruciate ligaments until to the posterior medial space. The posterior medial higher and lower approaches were then created. Under the surveillance of the posterior medial higher approach, the posterior mediastinum and bone bed were further cleaned by inserted shaving equipment through the low-position approach. The double-stranded PDS suture was introduced into approximately 1/3 of the junction of posterior cruciate ligament and tendon-bone using joint suture hooks. The PDS suture was then pulled out of the body through the median patellar approach. Two 5-0 surgical sutures were passed through the PDS suture. After inserting the Arthrex FlipCutter through the posteromedial low position of the knee joint to determine the angle and position, an incision about 2 cm long was made on the anterior and inner side of the knee joint, which was exposed to the bone surface. A Kirschner wire (2.0 or 2.5 mm) was injected into the inner and outer cortex of the distal tibial bed about 4–5 mm respectively. Then the Kirschner wire was removed. Spinal needles for lumbar puncture with double-stranded PDS sutures were inserted into the bone tunnel. The above-mentioned fixation sutures were threaded through the posterior cruciate ligament and pulled out of the tibial tunnel with the double-stranded PDS suture. The knee was bent to 90°, the fracture was reduced in the anterior drawer state, and the fixation sutures were tightened. Under direct vision of arthroscope, the reduced fracture was satisfactory. One suture was knotted and fixed on the plate, and the other was directly knotted and fixed on the bridge.
After the operation, the lower limbs were pressure-wrapped with elastic cotton roll cotton pads, and the knee joint was externally fixed with a brace.
Postoperative treatment
All patients underwent the reexamination of the postoperative knee joint anteroposterior film, and computed tomography (CT) scan, three-dimensional reconstruction and magnetic renascence imagining (MRI) of knee joint. All patients started functional exercises at the next day after surgery, including ankle pump exercises, four-head isometric contraction training, running on the spot, etc. Postoperative knee extension with external fixation lasted for 3 weeks followed by knee flexion exercises.
Follow-up
The healing and stability of knee joint, the range of motion and the functional recovery of affected limb were conducted regularly. The Lysholm score was used to assess the functional recovery. The last follow-up was completed after the button plate was taken out. At the last follow-up, the front and side views of the knee were re-examined.
Results
The patients in this study included 7 males and 8 females. Among them, one female patient had injuries on both knees. Their age ranged from 24 to 66 years old with an average age of (44 ± 17.5). In the 16 cases, there were six cases on the left knees and ten on the right knees. The patients underwent surgery 4–31 days after the injury, with an average of (13 ± 3.7) days. There were four cases of meniscus injury, four cases of Outerbridge of Grade III and higher, five cases of medial collateral ligament damage, and one case of lateral collateral ligament injury.
Knee flexion reached about 90° at the 4th week after surgery, and over 120° at the eighth week after surgery. Partial weight-bearing activities with crutches started at the sixth week after surgery and full weight-bearing activities at the eighth week after surgery.
The representative imaging of the knee joint before and after operation were shown in Figure 2. All 16 cases of PCL avulsion fractures of the knee joint were completely healed, in which six cases were positive in the posterior drawer test within Degree I, and the others were negative. All patients had no knee extension limitation, and the knee flexion range reached 120° or more, with an average of (132.4 ± 3.6)°, and the Lysholm score averaged (93.1 ± 4.7). The comparison of the imaging before and after the operation. (a) Preoperative lateral view of knee joint; (b) Three-dimensional CT of the knee joint before the operation; (c) MRI of knee joint before the operation; (d) Postoperative lateral view of knee joint; (e) Three-dimensional CT of the knee joint after operation; (f) MRI of the knee joint after operation.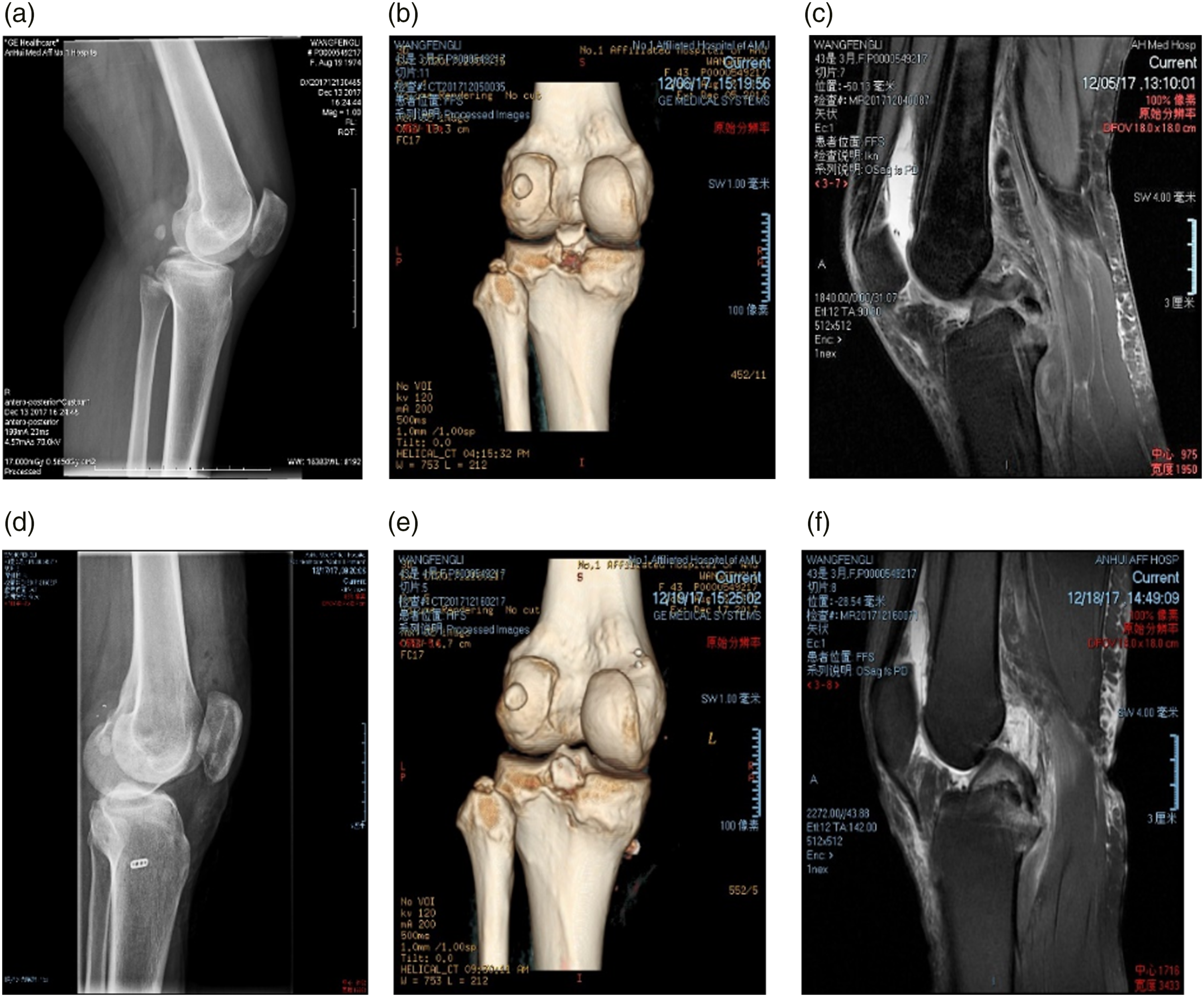
The knee flexion angles of 16 patients were compared at different time points
Followed-up bend angles of 16 patients at different time points.

Note:
aP = 0.000 compared with the knee flexion angle in the 4th week after operation.
bP = 0.000 compared with the knee flexion angle at the 8th week after operation.
cP = 0.000 compared with the knee flexion angle in the 6th month after operation.
Comparison of Lysholm scores of 16 patients at different time points
Lysholm scores of 16 patients at different time points were followed up.
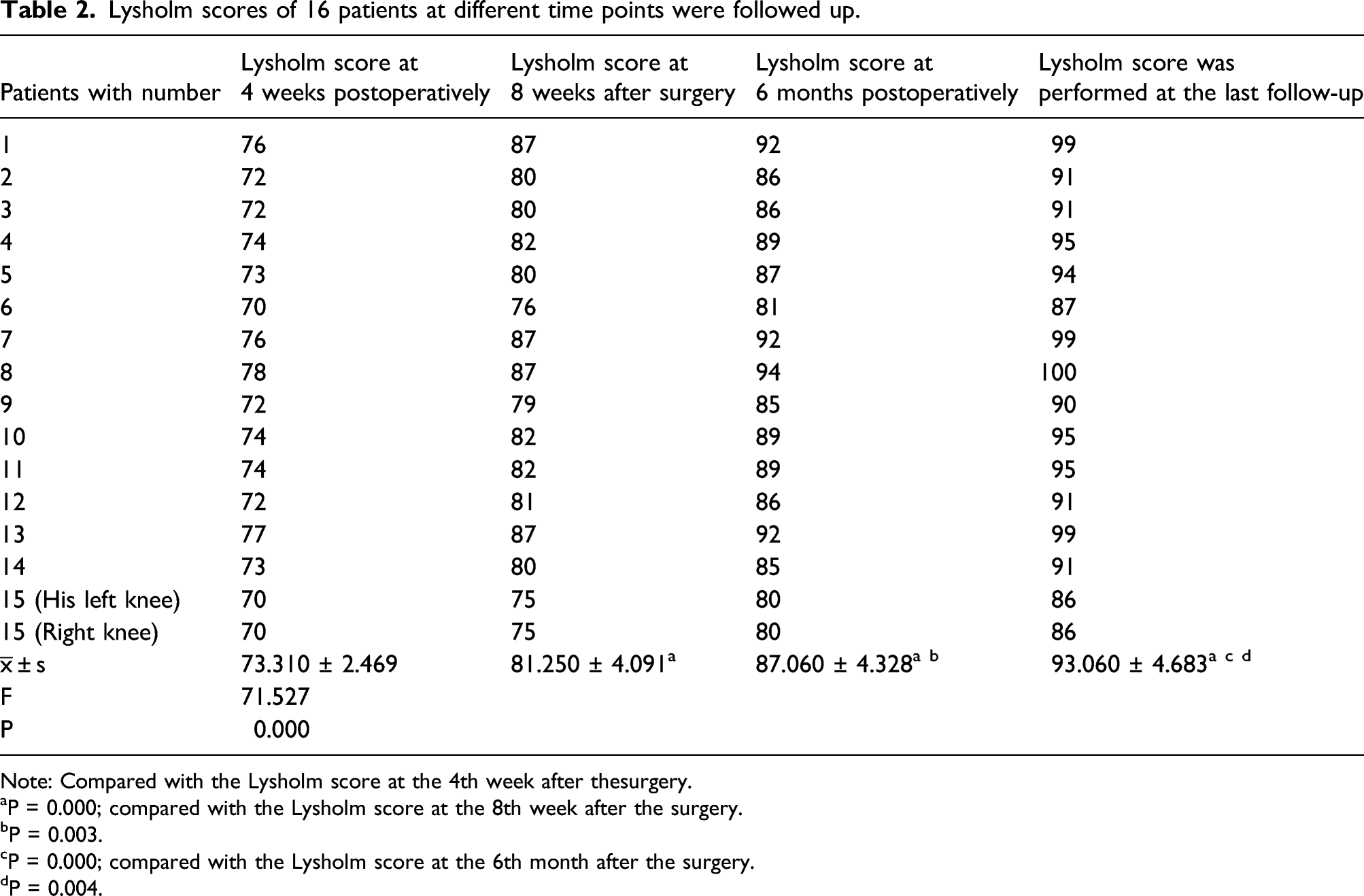
Note: Compared with the Lysholm score at the 4th week after thesurgery.
aP = 0.000; compared with the Lysholm score at the 8th week after the surgery.
bP = 0.003.
cP = 0.000; compared with the Lysholm score at the 6th month after the surgery.
dP = 0.004.
Discussion
The posterior cruciate ligament is the main structure that maintains the posterior stability of the knee joint, which plays an important role in maintaining the stability of the knee joint. 10 If the injury is not treated in time, it will cause severe knee instability, and further lead to secondary knee osteoarthritis.9,11 PCL tibial avulsion fracture is a special type of PCL injury, which is more properly subjected to surgical treatment than conservative treatment. Surgical treatment for PCL tibial avulsion fracture is considered to produce better outcomes than conservative treatment, even for those with the mild displacement of PCL tibial avulsion fracture.9,12
Traditionally, reduction and internal fixation of PCL tibial avulsion fractures through open posterior surgery have achieved satisfactory clinical outcomes.3,4,8,12,13 However, co-occurring intra-articular injuries cannot be treated at the same time, and some patients require further secondary arthroscopic surgeries. Hooper et al. 3 have performed a systematic review of the literature on PCL tibial avulsion fractures, and they find that the incidence of PCL tibial avulsion fractures with meniscus injury is 16.5%, and the incidence of co-occurring ligament injury is 19.1%. Pardiwala et al. 4 report that in a comparative study of 50 patients with PCL avulsion fractures under opening and arthroscopic fixation when examined with preoperative nuclear magnetic resonance imaging (NMRI), 28% of the patients have meniscus/cartilage injury or loose body of osteochondral in the joint. Moreover, of the 25 patients in the open reduction group, three underwent secondary arthroscopic surgery due to meniscus injury or cartilage injury. In our study, among the 16 cases of knee joints, four cases were co-occurring with a meniscus injury and four cases with cartilage damage of Outerbridge grade III and above, leading to the incidence rate as high as 27%. After treatment, the second arthroscopic surgery was avoided. Compared with traditional opening surgery, arthroscopic fixation has a huge advantage, especially for patients with meniscus/cartilage injury revealed by NMRI.
After treatment, the patient’s knee bend Angle and Lysholm score at the last follow-up were significantly better than those at week 4, week 8 and month 6 after surgery. High strength suture and fixation under modified arthroscopy for avulsion fractures of posterior cruciate ligament can significantly improve Lysholm score and joint function.
In recent years, with the rapid development of arthroscopic technology and continuous updating of surgical instruments, a variety of arthroscopic reduction and fixation methods for PCL tibial avulsion fractures with good clinical outcomes have been reported.3–7,9,14 Kim et al. 14 have first reported the use of posteromedial and posterolateral arthroscopic approachs to treat PCL avulsion fractures or comminuted fractures with a suture of the diameter less than 10-mm, and it has achieved satisfactory outcomes. At the same time, biomechanical experiments on cadavers also show that for PCL avulsion fractures, high-strength suture fixation can provide the same initial fixation strength as screw fixation, providing a theory for high-strength suture fixation to treat PCL avulsion fractures. 15 However, because of the depth of the posterior cruciate ligament tibia, the joint space on the posterior side of the knee is narrow, and the adjacent structures are complicated, which make it extremely difficult to perform arthroscopic surgery. Therefore, there is still controversy about the treatment of PCL avulsion fractures. Therefore, we have improved the existing PCL arthroscopic technique and summarized a standard operating procedure.
Our surgical method has exhibited the following advantages. (1) No special equipment is required, and it can be completed with conventional arthroscopy. (2) We have developed a novel method to establish the posterior medial high and low approach, and the approach is not affected by the medial femoral condyle, which facilitates the establishment of an ideal approach position. (3) This method can facilitate the clearance of soft tissues in the fracture and bone bed well and the visualization of the reduced fracture under direct vision, which leads to the ideal reduction effect. (4) After the arthroscope is placed in the posterior medial high-position approach for monitoring, there is no need to repeatedly change the approach for observation, which saves the operation time. (5) The posterior compartment can be directly entered through the median patellar approach, and it can be used as the third approach to other lines.
However, there are also some limitation in our study. For example, the sample size was small. In future, studies with more sample size are need to observe the advantages of this technology.
Conclusion
In conclusion, the improved arthroscopic high-strength suture fixation is easy to operate, reliable in fixation, and reproducible in the treatment of posterior cross tibial avulsion fractures. The knee joint functions after surgery have been significantly improved compared with the situation before surgery. However, due to the small sample size, it is more convincing if this technique can be applied to more cases of PCL tibial avulsion fractures. As a result, further research requires larger sample sizes and control studies, and it is necessary to compare the advantages and disadvantages of different surgical methods to solidify our results.
Supplemental Material
Supplemental Material - Improved arthroscopic high-strength suture fixation for the treatment of posterior cruciate ligament avulsion fracture
Supplemental Material for Improved arthroscopic high-strength suture fixation for the treatment of posterior cruciate ligament avulsion fracture by Lei Wu, Honggang Xu, Bo Li and Bin Xu in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.