
Abstract
Background:
Although posterior cruciate ligament (PCL) reconstruction is often performed for grade 3 PCL injuries, the effectiveness of different surgical techniques and rehabilitation protocols is a topic of debate.
Purpose/Hypothesis:
The purpose of this study was to evaluate and compare functional outcomes and residual instability in patients who underwent PCL reconstruction with versus without suture tape augmentation. It was hypothesized was that adding high-resistance suture tape to PCL reconstruction would improve functional scores and reduce postoperative laxity.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 48 patients were included in the study; all patients underwent PCL reconstruction with an autologous quadriceps tendon graft and had a minimum follow-up of 2 years. Overall, 23 patients were treated with a graft only, while 25 were treated with a graft and suture tape. Patients in the suture tape augmentation group also underwent an accelerated rehabilitation program with earlier range of motion and weightbearing. Patient characteristics, Lysholm scores, posterior tibial laxity on stress radiographs at 90° of knee flexion, and postoperative complications were compared between treatment groups.
Results:
No statistically significant differences were found between groups in terms of patient characteristics. Similar results were seen in both groups in terms of postoperative complications. Furthermore, on average, the Lysholm score increased from 1- to 2-year follow-up by 6.99 points (standard error = 0.97 points; P < .001), indicating progressive functional improvement, and posterior tibial laxity decreased from preoperatively to postoperatively by 7.55 mm (standard error = 0.24 mm; P < .001), indicating an improvement in knee stability. Patients in both treatment groups saw significant improvements during the follow-up period in the Lysholm score and posterior tibial laxity (P < .001 for both).
Conclusion:
PCL reconstruction with suture tape augmentation and an accelerated rehabilitation protocol did not result in significantly improved functional scores or postoperative laxity compared with isolated PCL reconstruction. The results showed no disadvantage of a more aggressive rehabilitation protocol.
Keywords
Posterior cruciate ligament (PCL) injuries are more frequent in patients with polytrauma (56.5%) than in those with sports injuries (32.9%), and PCL injuries in isolation are rare (3.5%) and are usually associated with multiligamentous injuries of the knee (96.5%). 3 The most common mechanism of a PCL injury is high-energy trauma, 6 such as in sports or motor vehicle accidents (57%). In car accidents, dashboard trauma is the most common, while in sports injuries, a fall with hyperextension of the knee is the main cause. 16
PCL injuries can cause knee instability, the progression to osteoarthritis, and an increased risk of concomitant injuries to other important structures, such as the menisci, other ligaments, and cartilage. 8 Recent reports with a long-term follow-up have identified a 6-fold higher rate of symptomatic osteoarthritis in patients with a PCL injury compared to patients with an intact PCL. 15
The treatment of PCL injuries is based on the degree of involvement of the ligament, inferred through a clinical examination and imaging. The initial treatment method is nonoperative because of the high regeneration potential of the PCL. Surgical treatment is reserved for high-grade injuries in active patients, symptomatic knee instability after nonoperative treatment, and associated multiligamentous injuries. 15
PCL injuries can be surgically treated with several techniques described in the literature, including transtibial, tibial inlay, and single- and double-bundle reconstruction.5,17 One of the most common problems associated with PCL reconstruction is residual laxity, which can lead to a relatively high rate of graft failure, ranging from 5% to 21% according to some studies. 17
A promising approach to reduce residual laxity and decrease the failure rate of PCL reconstruction is the use of reinforcement with suture tape on the ligament graft (Figure 1). This technique makes it possible to gain strength and decrease graft laxity, without altering postoperative physical therapy protocols that require a rapid gain in range of motion (ROM) and joint mobilization. Several biomechanical studies on cadaveric specimens have shown that the use of reinforcement with internal tape improves initial stability, decreases posterior translation of the tibia to levels similar to those of the intact knee, reduces total graft elongation, and increases final strength.2,4,9,14,15

Quadriceps tendon graft with a bone plug and suture tape augmentation.
The objective of this study was to evaluate functional outcomes and residual instability in patients undergoing PCL reconstruction with versus without suture tape augmentation. Our hypothesis was that suture tape augmentation would allow an accelerated rehabilitation protocol and would result in improved outcome scores and lower rates of failure or residual laxity.
Methods
After the study protocol received ethics committee approval, a retrospective review was conducted of the medical records of all patients from a trauma hospital who were surgically treated with PCL reconstruction using an autologous quadriceps tendon graft with a bone plug between 2017 and 2021. Some of the patients underwent surgery with only a graft, and some underwent surgery with a graft and suture tape augmentation (InternalBrace; Arthrex) (Figure 2). All patients were operated on by the same experienced surgeon. The decision to utilize suture tape augmentation was determined by the availability of surgical materials provided by the health care provider. This decision-making process, constrained by insurance coverage limitations, highlights the impact of logistical and economic factors on the selection of surgical techniques, thus aligning with the principles of pragmatic clinical trials.
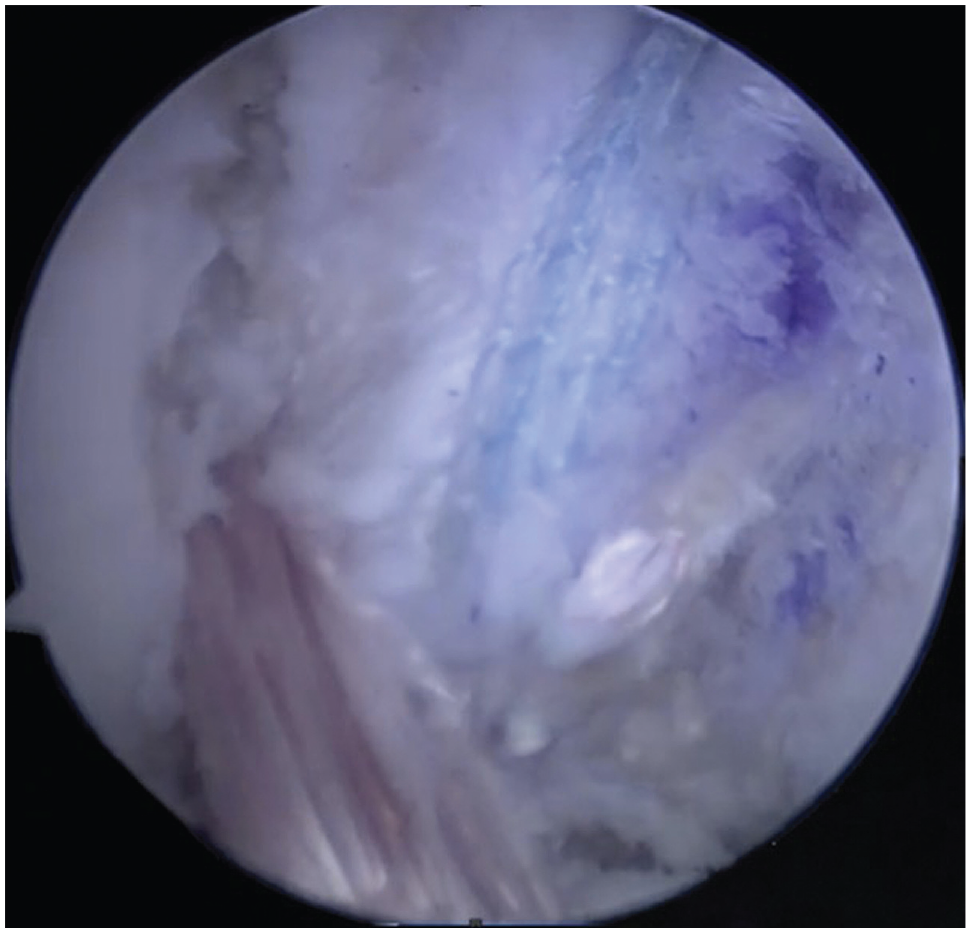
Arthroscopic image of a graft with suture tape augmentation.
Included were patients with a minimum follow-up of 2 years, with surgery taking place between 2017 and 2021. Patients with incomplete medical charts were excluded, as were patients who did not have a minimum follow-up of 2 years. We also excluded patients who were objectively detected with posteromedial, posterolateral, or anterior instability as well as those diagnosed with multiligamentous injuries. In this retrospective cohort, patients who concurrently underwent meniscus root repair, autologous osteochondral transplantation, or any other type of chondral or meniscal procedure that could interfere with the postoperative rehabilitation process were not evaluated.
Postoperative rehabilitation was carried out differently between the groups, with a more aggressive rehabilitation protocol for patients who underwent PCL reconstruction with suture tape augmentation. Patients in both groups were permitted to be weightbearing from day 0, with a different load intensity for each group. Immobilization in full extension was advised for both groups using a long, rigid immobilizer, which was removed only for daily rehabilitation activities. The rehabilitation protocols used by our team on patients are shown in Table 1.
Rehabilitation Protocols a

ROM, range of motion; SLR, straight-leg raise.
For the functional assessment, 1- and 2-year postoperative Lysholm scores 11 and preoperative and postoperative posterior tibial laxity (in mm) as measured on stress radiographs were used. All patients underwent preoperative and postoperative stress radiography with the knee at 90° of flexion according to Louisia et al. 10 Patients knelt on a padded bench, supported up to the tibial tubercle, with their hands placed on a high table for stability. Radiographs were acquired using a specialized jig that positioned the x-ray plate between the patient's legs, ensuring consistent high-quality lateral images without altering the patient's position (Figure 3A). Measurements were performed by tracing the distance between a line parallel to the posterior cortex of the tibia and the most posterior point along the Blumensaat line (Figure 3B). This methodology allowed for a precise assessment of tibial displacement relative to the femur. 1
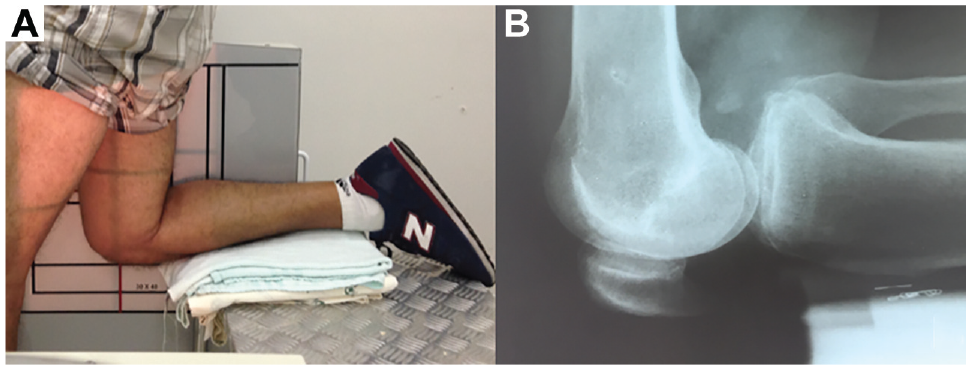
(A) Patient with knee at 90° of flexion for stress radiography. (B) Radiograph showing the measurement of posterior laxity.
Statistical Analysis
The quantitative parameters were described using summary statistics (mean with standard deviation, median with interquartile range) and compared with the Student t test, and the qualitative parameters were described using absolute and relative frequencies and compared with the chi-square test or Fisher exact test. 7 Generalized estimating equations were used with a normal distribution and identity link function, assuming an AR(1) correlation matrix (continuous-time first-order autoregressive correlation structure) between follow-up time points. 12 Analyses were followed by the Bonferroni correction of multiple comparisons to identify which group or time point pointed to different results when significant. 13
To conduct these analyses, we used SPSS for Windows (Version 22.0; IBM), and for the tabulation of data, we used Excel (Version 2013; Microsoft). The threshold for significance was set at P < .05.
Results
In this study, the eligible population consisted of 48 patients who underwent PCL reconstruction. Of these, 23 patients underwent reconstruction that included a graft only, while 25 patients underwent reconstruction with a graft in combination with suture tape. Table 2 presents the patient characteristics and surgical outcomes between the graft-only and graft + suture tape groups. Statistically, there were no significant differences regarding patient characteristics or surgical outcomes between the groups.
Patient Characteristics and Surgical Outcomes a
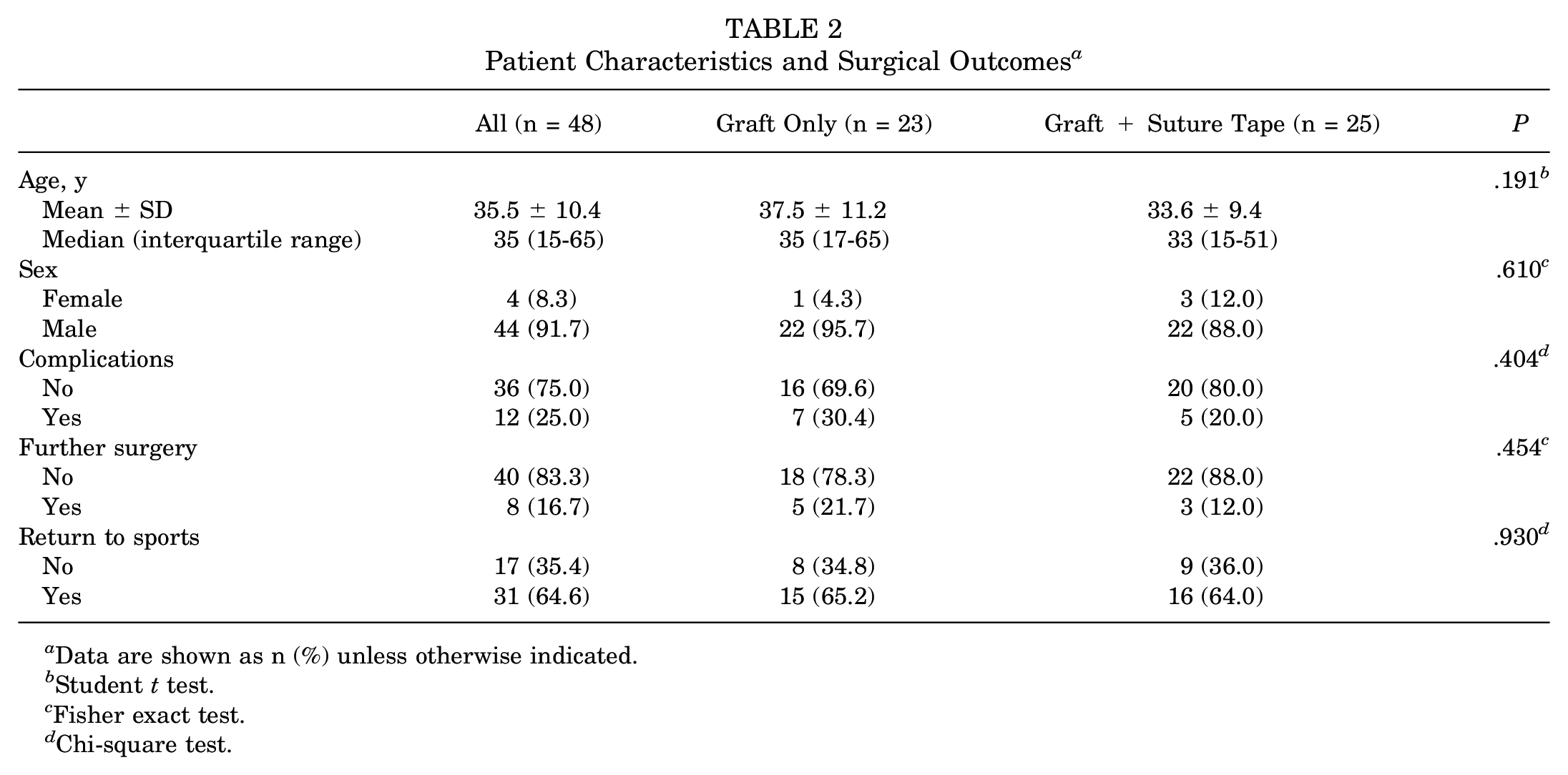
Data are shown as n (%) unless otherwise indicated.
Student t test.
Fisher exact test.
Chi-square test.
Table 3 presents the Lysholm scores and radiographic outcomes for each group. Regarding the Lysholm score and posterior laxity, there were no significant interactions between groups over time (PGroup×Time = .797 and .261, respectively), and regardless of the time of assessment, no significant differences were observed between groups (PGroup = .285 and .090, respectively). However, both groups saw significant improvements according to time point in both the Lysholm score and posterior laxity (PTime < .001 for both). On average, the Lysholm score increased from 1 year to 2 years postoperatively by 6.99 points (standard error = 0.97 points), and posterior laxity decreased from preoperatively to postoperatively by 7.55 mm (standard error = 0.24 mm).
Lysholm Scores and Radiographic Outcomes a

Generalized estimating equations were used with a normal distribution and identity linkage function, assuming an AR(1) correlation matrix between time points.
The complications observed in this study included arthrofibrosis in 7 patients, pain in 4 patients, and deep vein thrombosis in 1 patient. Of these complications, 3 cases of arthrofibrosis, 1 case of deep vein thrombosis, and 1 case of pain were noted in the group that underwent PCL reconstruction with suture tape augmentation. In contrast, 4 patients who developed arthrofibrosis and 3 patients who experienced pain were from the group that underwent PCL reconstruction only. Patients who had arthrofibrosis underwent an additional procedure (manipulation under anesthesia).
Discussion
This study evaluated Lysholm scores, residual instability on stress radiographs, and complications among patients after PCL reconstruction with versus without suture tape augmentation. Patients who underwent PCL reconstruction with suture tape augmentation completed a rehabilitation program that allowed earlier ROM and weightbearing. The results obtained showed that there were no statistically significant differences between the study groups in the evaluated parameters. Thus, PCL reconstruction, both with and without suture tape augmentation, produced similar postoperative outcomes, and our hypothesis that suture tape augmentation would result in better outcomes was rejected.
The study findings demonstrated that the internal brace group was able to undergo more aggressive rehabilitation without any change in their outcomes or complications compared to the other group. The accelerated rehabilitation protocol did not have any deleterious effect on PCL graft healing and may allow patients to return earlier to daily activities. On the other hand, the more conservative protocol, used for patients who only underwent PCL reconstruction, imposed more restrictions and limitations.
Regarding the results during follow-up, a mean increase in the Lysholm score was observed in both treatment groups, indicating a progressive functional improvement over time. As for the radiographic examination, 10 a mean decrease in posterior tibial laxity was observed in both groups. This reduction can be explained by the fact that PCL reconstruction aims to restrict posterior tibial translation, which can lead to a decrease in residual instability. 1
Previous studies (eg, LaPrade et al 8 ) have shown a more conservative rehabilitation approach, with the use of braces for up to 25 weeks. Furthermore, a literature review by Senese et al 14 revealed that only 34% of the studies describe specific recommendations for strengthening the hamstring. Among these studies, only 15% started strengthening exercises after 6 weeks, while 46% started after 12 weeks, 62% after 16 weeks, and 100% after 24 weeks. The more aggressive rehabilitation protocol adopted in the current study for PCL reconstruction with suture tape augmentation resulted in outcomes comparable to these more conservative protocols. The findings of this study suggest that PCL reconstruction with internal bracing, together with a more aggressive rehabilitation protocol, may be a viable option for patients who want a faster recovery, less postoperative restrictions, and a better quality of life. It is unknown if the accelerated rehabilitation protocol could be safely implemented with a quadriceps tendon autograft alone.
Biomechanical studies have also been performed to evaluate the effects of additional reinforcement on PCL reconstruction. Levy et al 9 conducted an in vitro biomechanical study and demonstrated that the use of suture tape as independent reinforcement resulted in a decrease in final elongation of the graft and an increase in its final strength, thus concluding that the reinforcement technique provides better joint stability. Furthermore, a clinical study by Hopper et al 4 showed favorable results with the use of reinforcement with suture tape in PCL reconstruction.
The use of additional reinforcement in PCL reconstruction is a recent area of interest. Suture tape augmentation has been a promising approach. Research by Fanelli and Edson 3 in 1995 demonstrated that tape reinforcement could improve knee stability and clinical outcomes. Therrien et al 15 compared PCL reconstruction with and without suture tape, concluding that the addition of reinforcement improved anterior stability of the knee. These findings are supported by Zhao et al, 17 who described the internal reinforcement technique with independent suture tape and reported promising clinical results. However, we did not find that the addition of suture tape resulted in any improvement in the Lysholm score or posterior laxity.
However, it is important to emphasize that the effectiveness and need for additional reinforcement in PCL reconstruction are still topics of debate in the literature. Further studies are needed to assess long-term clinical and functional outcomes as well as to compare different augmentation techniques. The review by Senese et al 14 highlights the importance of personalized rehabilitation after PCL reconstruction and provides recommendations on published rehabilitation protocols. They emphasized the importance of a multidisciplinary approach, including manual therapy, strengthening exercises, proprioceptive training, and progressive functional activities, with the goal of restoring ROM, muscle strength, and joint stability.
Limitations
The first limitation of this study is the sample size, which may have influenced the statistical results. Furthermore, follow-up was limited to a period of 2 years, which may not be enough time to fully assess the effectiveness of different PCL reconstruction techniques. Both aspects can influence the direction and magnitude of potential bias. It is possible that adding more patients or a longer follow-up period could affect the results. One significant limitation of our study is the variation observed in both the surgical techniques and rehabilitation protocols used. Although this variability afforded us the chance to assess the safety of accelerated rehabilitation, it hampers the study's ability to conclusively attribute the observed outcomes solely to either the surgical approach or the rehabilitation regimen. As a limitation, the absence of objective data on strength and ROM at final follow-up is acknowledged. As discharge criteria and return-to-sports objectives, complete ROM and muscle strength comparable to the contralateral side were targeted. In this retrospective cohort, all patients met the strength and ROM parameters for medical discharge; however, objective measurements on these parameters were not obtained. These were only noted in medical records as either “achieved” or “not achieved.” It was not within the scope of this study to evaluate return to sports, and data on the Tegner activity scale were not collected, which we acknowledge as a limitation of this study, along with the lack of objective measurements of final ROM and strength using dynamometry.
Previous evidence has indicated the use of more conservative rehabilitation protocols, but our results suggest that a more aggressive approach may be effective, despite not demonstrating superiority over the more conservative protocol.5,14 While this study presents valid conclusions for the assessed groups, the generalizability of the results may be limited by the relatively small and homogeneous sample. Future studies on larger and more diverse populations are needed to confirm the results of this study and to evaluate the usefulness of suture tape augmentation in clinical practice in a broader setting.
Conclusion
Suture tape augmentation of PCL reconstruction and an accelerated rehabilitation protocol did not result in improvements in functional scores or postoperative laxity. The results of this study indicated that PCL reconstruction with and without suture tape augmentation produced similar functional and residual instability outcomes. The results also showed no disadvantage of a more aggressive rehabilitation protocol.
Footnotes
Final revision submitted July 5, 2024; accepted July 18, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hospital Leforte (No. 6.033.975).