
Abstract
Background:
The potential intra-articular effects of ≥1 year after anterior cruciate ligament reconstruction (ACLR) with independent suture tape augmentation (STA) are not fully understood.
Purpose:
To investigate whether incorporating suture tape in an all–soft tissue quadriceps tendon autograft (QTA) ACLR leads to satisfactory patient outcomes while having no intra-articular side effects as determined by magnetic resonance imaging (MRI).
Study Design:
Case series; Level of evidence, 4.
Methods:
Included were 25 patients with a mean age of 19.9 years (95% CI, 17.3-22.5 years) who underwent QTA ACLR with STA between 2016 and 2019. All patients underwent MRI at ≥1 year postoperatively and had at least a 2-year follow-up (mean, 28 months [95% CI, 26.5-29.5 months]) that included physical examination with anterior laxity testing with KT-1000 arthrometer, radiographs, and patient-reported outcome measures (PROMs). At the final follow-up, the minimal clinically important difference (MCID) and the Patient Acceptable Symptom State (PASS) for applicable PROMs were applied to each patient. Postoperative graft and joint integrity were assessed using the Howell classification and the MRI Osteoarthritis Knee Score (MOAKS) joint effusion/synovitis grade. The Mann-Whitney U test for continuous variables and the chi-square or the Fisher exact test for categorical variables were used for statistical analyses.
Results:
The MRI assessment of the grafts demonstrated intact grafts in all patients. Overall, 96% of patients demonstrated grades 0 or 1 MOAKS for joint effusion/synovitis. All patient outcomes significantly improved from preoperatively to the final follow-up (P < .001), except for the Marx score, which decreased significantly (14.2 [95% CI, 12.7-15.8] vs 9.72 [95% CI, 7.3-12.2]; P = .0014). At least 68% of the patients achieved the MCID threshold, and 92% achieved the PASS threshold for all applicable PROMs.
Conclusion:
QTA ACLR with STA did not demonstrate adverse intra-articular changes on MRI at ≥1 year postoperatively. In addition, STA did not appear to negatively affect PROMs.
Keywords
Anterior cruciate ligament (ACL) ruptures have an annual global incidence ranging from 30 to 78 people per 100,000.17,18,42 Subsequently, the ACL reconstruction (ACLR) rate has continued to rise over the past 3 decades.1,20,38,42 ACL ruptures typically occur in the adolescent and young adult populations, with autograft failure rates as high as 23% in patients aged <25 years within the first 2 years.17,55 Furthermore, worse subjective and objective outcomes are experienced with revision compared with primary ACLR.16,31,35 ACL retears significantly increase the risk of additional injuries to the patient's knee and raise overall treatment costs, placing an increased economic burden on the health care system. 21 Therefore, developing safe strategies that decrease graft failure rates and lead to satisfactory patient outcomes is important.
Recently, there has been renewed interest in graft-augmentation techniques for ACLR,13,26,28,34,40,48-52 especially relating to the biomechanical benefit of graft protection and load sharing.5,6,26,34 In 2 separate biomechanical studies performed by Bachmaier et al,5,6 it was found that independent suture tape augmentation (STA) led to significantly reduced graft elongation, higher ultimate failure loads without signs of stress shielding, and increased final construct stiffness. Historically, there has been a negative connotation surrounding the use of artificial devices (ie, Kennedy ligament augmentation device) for augmenting ACLR because of high complication and failure rates associated with synthetic devices used for ACLR.29,53,54
This study investigated whether incorporating suture tape in an all–soft tissue quadriceps tendon autograft (QTA) ACLR leads to satisfactory patient outcomes while having no intra-articular side effects as substantiated by magnetic resonance imaging (MRI). We hypothesized that STA would not negatively affect the joint and that scores on patient-reported outcome measures (PROMs) would significantly improve postoperatively.
Methods
Patient Selection
Institutional review board approval was obtained for the study protocol. All patients aged 15 to 45 years at the time of surgery who underwent primary QTA ACLR with STA between 2016 and 2019 by the senior surgeon (P.A.S.) were retrospectively reviewed. As part of the study, MRIs of the ipsilateral knee were obtained prospectively at least 1 year postoperatively after formal patient consent.
Patients were excluded if they were aged <15 years or >45 years at the time of surgery, had undergone extra-articular stabilization, or had undergone a multiligamentous procedure. Patients who could not be contacted via telephone or email because of incorrect telephone number documentation on their electronic health records were deemed lost to follow-up.
Data Collection
All preoperative PROMs were collected retrospectively from our institution's registry, and all preoperative objective data were collected from the patient charts. Prospectively, the patients completed the following validated PROMs during their 2-year office visit: visual analog scale (VAS) for pain 22 ; Marx activity rating scale 36 ; Single Assessment Numeric Evaluation (SANE) 46 ; Tegner activity scale; Tegner Lysholm knee score (Lysholm) 10 ; International Knee Documentation Committee (IKDC) subjective survey 19 ; Veterans Rand 12-Item Health Survey (VR-12) 45 ; and 3 of the Knee injury and Osteoarthritis Outcome Score (KOOS) subscales—including Sports and Recreation (Sports), Quality of Life (QoL), and Symptoms and Stiffness (Symptoms). 41
Previously reported values for the minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS) thresholds were applied to all applicable PROMs for the final PROM interpretation.7,13,37,39 For the Lysholm score, an MCID of 10.6 points was applied. 39 For the IKDC, an MCID of 18.9 points and a PASS of 75.9 were applied.7,37,39 Regarding the MCID and PASS thresholds for the KOOS subscales, 27 points and 75 were applied for the KOOS-Sports, 25.9 points and 62.5 were applied for the KOOS-QoL, and 15.7 points and 57.1 were applied for the KOOS-Symptoms, respectively.7,37,39 Regarding the MCID and PASS thresholds for VAS pain, an MCID of 1.2 points and a PASS of 1 were applied. 13
At the 2-year prospective follow-up, each patient underwent a physical examination, which included anterior laxity testing using a KT-1000 arthrometer (MEDmetric) and radiographic imaging. A prospective MRI of the ipsilateral knee was collected at least 1 year postoperatively. The senior surgeon collected intraoperative data such as concurrent procedures.
Graft Dimensions and Surgical Technique
Full-thickness, all–soft tissue quadriceps grafts were used in all cases. 43 The final graft length ranged from 62 to 71 mm depending on the intra-articular distance from the femoral and tibial socket depths and the initial length of the quadriceps tendon immediately after harvesting. The diameter of the graft ranged from 10 to 11 mm depending on the size of the native quadriceps tendon, as margins were marked before harvesting.
ACLR was performed using an all–soft tissue QTA via an all-inside approach utilizing a suspensory adjustable loop device (ALD; ACL TightRope II; Arthrex) for cortical femoral fixation. 32 For the STA (InternalBrace; Arthrex), a 2-mm wide by 0.5-mm thick suture tape (FiberTape; Arthrex) was passed through the ALD femoral button to remain independent of the graft, which was passed through the ALD loop 43 (Figure 1).

Overhead view of the proximal adjustable loop device demonstrating the suture tape (black arrowhead) looped through the femoral button to remain independent from the graft, which is associated with the femoral TightRope loop (asterisk). Pull sutures (white arrow) and femoral shortening strands (black arrow) are also pictured.
After graft passage in the femoral socket, the graft was passed into the tibia with a shuttle suture. A tibial fixation button (TightRope ABS Button; Arthrex) was applied to the distal ALD for suspensory fixation, and the 2 ends of the suture tape were passed through the 2 holes of the button. The ALD shortening strands were used to advance this button to the tibia but not to tighten the graft on the tibia, as the suture tape was always fixed first. This was done by taking the slack out of the 2 ends of the suture tape, then with the knee positioned in full hyperextension, a 4.5
Tibial graft fixation was done while the knee was fully hyperextended. The knee was then cycled through a full range of motion 15 to 20 times, then the femoral and tibial ALD shortening strands were tightened with the knee hyperextended. Because of the normal knee biomechanics of the ACL lengthening 3 mm from 90° of flexion to full extension, with the tape always fixed in full hyperextension, it will be slightly lax at 90° (Figure 2). 30

Arthroscopic view of the final (A) all–soft tissue quadriceps tendon autograft construct through the anterolateral portal of a right knee at approximately 90° of knee flexion after the final graft fixation. (B) The suture tape (asterisk) runs posteriorly relative to the graft and can be visualized using a probe, as seen here.
Postoperative Protocol
An accelerated rehabilitation program was followed (Table 1). Each patient was seen in the clinic at 2 weeks, 10 weeks, and 6 months postoperatively as part of routine follow-up. If the patients were medically cleared at the 6-month visit, they were to schedule appointments as needed but were encouraged to return to the office 1 year postoperatively for a final physical examination, including anterior laxity testing, as part of routine follow-up. Study MRIs were completed prospectively at the 2-year office visit if not done so already.
Postoperative Rehabilitation Protocol a

CPM, continuous passive motion; MRI, magnetic resonance imaging; PROMs, patient-reported outcome measures; PT, physical therapy; RTS, return to sport.
MRI Evaluation
A musculoskeletal radiologist (J.D.S.) with 8 years of experience, who was blinded to the surgical technique and patients’ clinical status, prospectively reviewed all imaging examinations. All images were examined using RadiAnt DICOM viewer software Version 2021.2.2 (Medixant). Patients were scanned on a 1.5-T magnet with a dedicated knee coil. The examination consisted of axial T2-weighted with fat suppression, coronal T1-weighted, fat-suppressed T2-weighted, and sagittal T1-weighted images. Oblique axial proton density with fat suppression and oblique sagittal fat-suppressed T2-weighted images were acquired with imaging planes oriented to the ACL graft.
The initial image review was a quantitative assessment of the ACL grafts with a region of interest (ROI) measured in the proximal, midsubstance, and distal ACL graft and the midsubstance posterior cruciate ligament (PCL). Signal intensity was measured utilizing 15 mm2 ROIs, with the mean signal intensity calculated by the imaging software (Figure 3). The standard deviations and ranges were also calculated for the ROIs. As described by Lutz et al, 33 the measured signal intensity within the ROI of the PCL served as an internal control for the signal intensity, which may vary based on patient size and imaging technique. The calculated ACL signal intensity/PCL signal intensity ratios (APRs) allowed a more accurate comparison between examinations.

ROIs within the ACL graft. Sagittal T2-weighted MRI was used to measure signal intensity using 15 mm2 ROIs at the distal (red), midsubstance (green), and proximal (blue) ACL autograft. The mean signal intensities were calculated within the ROIs. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging; ROIs, regions of interest.
A qualitative MRI assessment was performed 1 week later by the same musculoskeletal radiologist. The integrity and internal signal intensity of each graft were assessed. Graft signal intensity was evaluated using the modified Howell classification11,23 (Figure 4). The intrarater reliability of the MRI measurements was also evaluated.

The different ACL Howell grades as seen on sagittal T2-weighted MRI from 3 different knees: (A) grade 1 (completely homogeneous graft); (B) grade 2 (increased intrasubstance intensity involving <50% of the graft); and (C) grade 3 (increased intrasubstance intensity involving >50% of the graft). Knees with Howell grade 4 were not seen in the study cohort. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
As contrast is not routinely administered on knee MRI examinations assessing for internal derangement, the presence of inflammation in the joint was evaluated utilizing the MRI Osteoarthritis Knee Score (MOAKS) 25 (Figure 5). ACL Howell grades and MOAKS effusion/synovitis grades were assessed again at a subsequent point in time to calculate the intrarater reliability.

Coronal (left) and sagittal (right) T2-weighted MRIs from 3 different knees representing MOAKS effusion/synovitis classifications: (A) grade 0 (none); (B) grade 1 (mild); and (C) grade 2 (moderate). MOAKS grade 3 cases were not seen in the study cohort. MOAKS, MRI Osteoarthritis Knee Score; MRI, magnetic resonance imaging.
Statistical Analysis
Continuous variables were expressed using either means (95% CI) or medians (interquartile range [IQR]), and the Mann-Whitney U test was used to compare continuous variables between groups. Categorical variables were expressed using absolute frequency (percentage), and the chi-square or Fisher exact test was used to compare categorical variables between groups. Intrarater agreement regarding the MRI-based assessments was calculated using the Cohen kappa coefficient (κ) with 95% CI. Bivariate analyses were used to assess the relationship between APRs and postoperative MRI follow-up time and were expressed using the Pearson correlation coefficient (r) with 95% CI. Data were analyzed using JMP Version 17 (SAS Institute Inc). For statistical analysis in this study, P < .05 was considered statistically significant.
It was determined that 25 patients would be needed to test a difference in proportions of 0.30, with a power of 0.90, when alpha was equal to .05.
Results
A total of 239 patients were retrospectively reviewed, with 42 patients meeting study eligibility requirements. Because the study was conducted during the COVID-19 pandemic, 17 patients (40%) meeting eligibility criteria could not travel to the clinic for various personal, logistical, and/or financial reasons. Thus, 25 patients with a mean age of 19.9 years (95% CI, 17.3-22.5 years) and a mean final follow-up of 28 months (95% CI, 26.5-29.5 months) were included in this study (Figure 6). The median time from surgery to MRI was 24 months (IQR, 15-26 months). Patient characteristics are summarized in Table 2.

A flowchart of included and excluded patients. ACLR, anterior cruciate ligament reconstruction; non-QTA ACLR, nonquadriceps tendon autograft ACLR (bone patellar-tendon bone autograft, quadrupled semitendinosus autografts, other); ALLR, anterolateral ligament reconstruction.
Patient Characteristics (N = 25 Patients) a
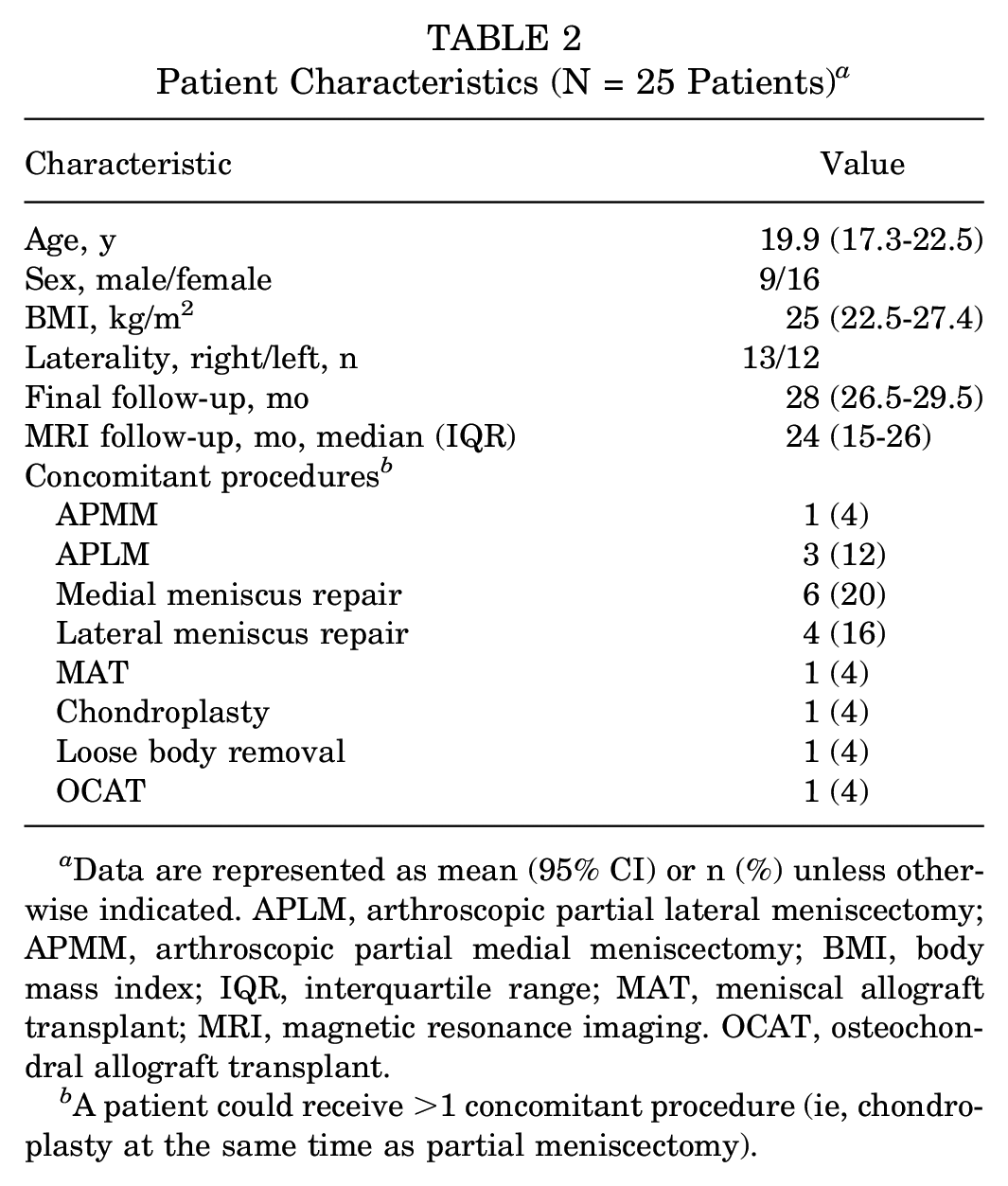
Data are represented as mean (95% CI) or n (%) unless otherwise indicated. APLM, arthroscopic partial lateral meniscectomy; APMM, arthroscopic partial medial meniscectomy; BMI, body mass index; IQR, interquartile range; MAT, meniscal allograft transplant; MRI, magnetic resonance imaging. OCAT, osteochondral allograft transplant.
A patient could receive >1 concomitant procedure (ie, chondroplasty at the same time as partial meniscectomy).
There was near-perfect intrarater agreement when assessing the overall APRs of the ROIs within the ACL graft segments and native PCL (κ = 0.85 [95% CI, 0.66-1]; P < .001). There was perfect intrarater agreement when assessing Howell grades within the ACL graft (κ = 1; P < .001) and substantial intrarater agreement when assessing MOAKS grades (κ = 0.80 [95% CI, 0.66-0.95]; P < .001).
Details of the MRI evaluation are summarized in Table 3. MRI assessment demonstrated completely intact grafts in all patients. Only 1 patient showed a Howell grade 3 graft, and none demonstrated a Howell grade 4. The median MRI follow-up time for those with Howell grades 1 and 2 was ≥24 months. Furthermore, 96% of patients had a MOAKS grade 0 or 1 for joint effusion/synovitis, with a median MRI follow-up time ranging from 15 to 25 months; only 1 patient demonstrated a grade 2, and none demonstrated a MOAKS grade 3. The highest mean APR was noted in the midsubstance of the graft (1.8 [95% CI, 1.6-2.1]). However, all segments demonstrated comparable APRs. There were no associations between APRs from any segment and the postoperative MRI follow-up time.
Results of MRI Evaluation a

Data are reported as n (%), median [interquartile range], or mean (95% CI) unless otherwise indicated. APR, anterior cruciate ligament signal intensity/posterior cruciate ligament signal intensity ratio; IQR, interquartile range; MOAKS, MRI Osteoarthritis Knee Score; MRI, magnetic resonance imaging.
Median value unavailable due to only one value being included.
Pearson r (95% CI) for association between the APR and MRI follow-up time.
Pre- and postoperative PROMs and anterior laxity measurements are shown in Table 4. KT-1000 arthrometer objective joint laxity improved significantly from preoperatively to the final follow-up. All PROM scores similarly improved postoperatively with the exception of the Marx score, which decreased significantly from pre- to postoperatively (14.2 [95% CI, 12.7-15.8] vs 9.7 [95% CI, 7.3-12.2]; P = .0014). It was found that 7 patients sustained their injury and underwent ACLR during their final season and did not go on to play at the next level of competition.
Patient Outcomes a
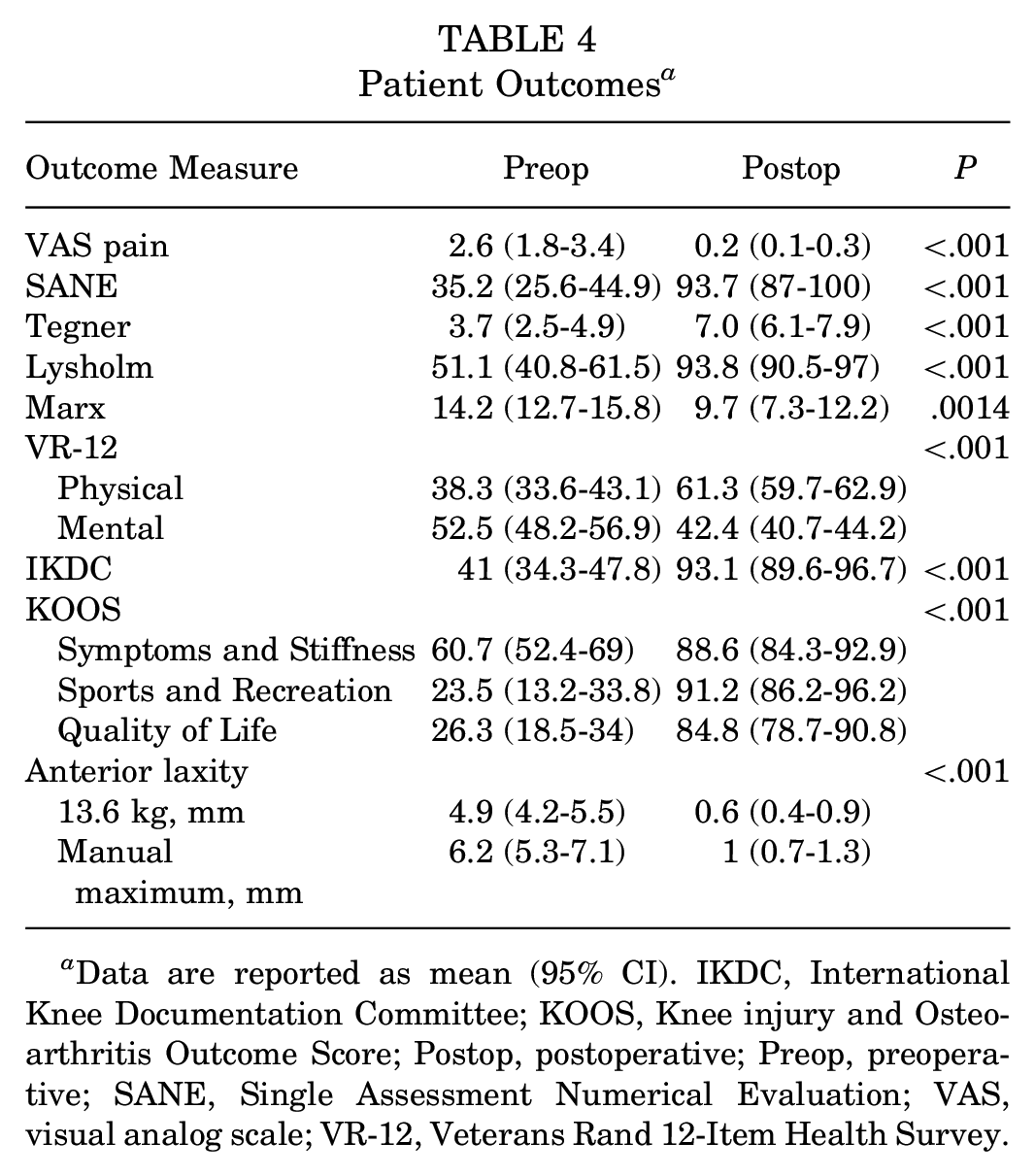
Data are reported as mean (95% CI). IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; Postop, postoperative; Preop, preoperative; SANE, Single Assessment Numerical Evaluation; VAS, visual analog scale; VR-12, Veterans Rand 12-Item Health Survey.
The MCID was met in 92% of patients completing the Lysholm as well as the KOOS-QoL subscale, 100% of those completing the IKDC, 96% of those completing the KOOS-Sports subscale, and 68% of those completing the VAS pain as well as the KOOS-Symptoms subscale. The PASS was achieved in 96% of patients completing the IKDC as well as the KOOS-QoL subscale, 92% of those completing the KOOS-Sports subscale, and 100% of those completing the VAS pain as well as the KOOS-Symptoms subscale.
No patients showed osteoarthritic changes on radiographs at the 2-year follow-up. Four (16%) patients necessitated a subsequent procedure (Table 5). Three cases were due to mild, Shelbourne type 1 arthrofibrosis—loss of <10° of full, active extension but all knees could be passively straightened 47 —occurring within the first year after their initial surgery.
Subsequent Reoperations a

ACLR, anterior cruciate ligament reconstruction; APM, arthroscopic partial meniscectomy.
Includes synovectomies, excision of fat pad fibrosis, and notchplasties.
Discussion
Our most important finding was that the prospective MRI data—at median time from surgery to MRI of 24 months—showed that augmenting QTA ACLR with suture tape led to similar graft signal intensities and Howell scores previously described for nonaugmented grafts,2,9,11,23,33 with most patients demonstrating little to no synovitis. 25 This suggests that STA does not interfere with the ligamentization process, lead to objective differences seen within the graft, or incite a significant intra-articular inflammatory response.
In the MRI study performed by Lutz et al, 33 the APRs of a healthy native ACL for the distal, midsubstance, and proximal segments was 2.6, 2.6, and 3.4, respectively, as the ACL is inherently less dense than the native PCL. Our APRs for the autograft were lower, which may be due to a higher density within the graft compared with the native ACL. In another MRI-based study comparing signal intensity between nonaugmented QTA and hamstring tendon autograft, Aitchison et al 2 found the signal intensity to be significantly lower in the quadriceps tendon at 1 year compared with the hamstring tendon (2.33 vs 2.72). Furthermore, these authors found that quadriceps tendon signal intensities significantly decreased at 1 year compared with 6 months postoperatively (2.70 vs 2.33). This may suggest that as the quadriceps tendon goes through the ligamentization process, changes may continue to be seen within the graft at the final follow-up compared with an earlier timepoint and that the signal intensities of QTAs demonstrate lower values compared with those of both the native ACL and the hamstring tendon autografts.2,33
Regarding the safety of STA for ACLR, translational canine studies have been performed to study this issue. Cook et al 12 found that ACLR in 10 adult research hounds with a QTA with STA did not result in premature osteoarthritis (OA) development after surgery, as evidenced by the 6-month radiograph evaluation. In a subsequent canine study comparing nonaugmented bone–patellar tendon–bone (BTB) autografts and QTA ACLR with STA, Smith et al 52 found that allograft proved to be superior to BTB regarding objective outcomes— including radiographic OA scores. In a third canine study, Smith et al 50 were unable to find postoperative complications such as lameness or clinical dysfunction, severe inflammatory or immune responses, cartilage damage, or premature OA when nonabsorbable braided suture tape was placed alongside a healthy, native ACL—even with the suture tape transected. Of note, none of the patients in the present study exhibited any signs of premature arthritic changes on their 2-year follow-up compared with their preoperative radiographs.
All patient outcomes improved at the final follow-up, with the exception of the Marx score, which decreased significantly. It was found that 7 patients sustained their injury and underwent ACLR during their final season and did not go on to play at the next level of competition. It is not uncommon for patients to have decreased activity levels the farther away they are from primary ACLR,8,27,44 especially if they undergo surgery during their final year of eligibility—particularly at the collegiate level. Two previous studies have found that when compared with nonaugmented cohorts,28,40 the patients with STA exhibited comparable PROM scores, providing further subjective evidence that STA does not negatively affect joint function. Although the present study lacked a control group to compare with, our PROM scores were at least comparable to those that have already been studied.28,40 Moreover, most patients satisfied the MCID and PASS thresholds for all applicable PROMs. These subjective patient outcomes are more than likely because of the ACLR itself rather than the augmentation; nonetheless, it is important to reiterate that augmenting the ACLR with suture tape does not appear to decrease patient satisfaction.
A total of 4 patients (16%) required additional surgical intervention after their initial procedure. Three cases (12%) were due to mild, Shelbourne type 1 arthrofibrosis—loss of <10° of full, active extension but all knees could be passively straightened 47 —occurring within the first year after their initial surgery. Ekhtiari et al 15 demonstrated that arthrofibrosis, universally, affects 4% to 38% of the patients after ACLR. Furthermore, ACLR utilizing QTAs has increased the risk of short-term postoperative arthrofibrosis. 24 The senior surgeon is aggressive in treating postoperative arthrofibrosis, placing great emphasis on the restoration of full knee extension to improve patient quality of life and optimize daily function. Because of the location of the fibrotic tissue—typically found anteriorly within the fat pad—relative to the position of the suture tape that typically runs posterior to the graft, we do not believe this mild arthrofibrosis was because of the suture tape itself. However, we are unable to completely exclude this possibility, as we did not have a nonaugmented group to compare with.
Last, none of our patients necessitated subsequent revision ACLR. This is an important finding given the young mean age of our patients at 19.9 years, as previous studies have shown patients this age to be at high risk for graft failure.3,55 Duong et al 14 found similar results in their study, as they did not record a single retear after ACLR with STA; however, they only had a 1-year documented follow-up and a mean patient age of 33 years, with 75% of their study cohort being men.
Limitations
This study was not without limitations. Because the study was conducted during the COVID-19 pandemic, we could not contact and obtain consent from a large percentage of the eligible patients, which led to a 40% loss to follow-up, thus limiting the study's power and increasing the possibility of selection bias. As the surgical procedures were only performed by the senior author, who is familiar with the technique, the results of this study may not be generalizable. In addition, by only including a single autograft type, it would not be possible to conclude that ACLR with STA will lead to an acceptable intra-articular environment for other commonly used grafts such as quadrupled semitendinosus and BTB autografts as well as allografts. There was a wide range of variation in the timing of postoperative MRIs because patients provided consent on a rolling basis at different time points throughout the postoperative period. However, MRI grading scores were comparable between those obtained >2 years and those obtained ≤2 years.
Conclusion
In the present study, QTA ACLR with STA did not demonstrate adverse intra-articular changes on MRI at ≥1 year postoperatively. In addition, STA did not appear to negatively affect PROMs.
Footnotes
Acknowledgements
The authors thank Arthrex for both financial and nonfinancial support throughout the entirety of this project.
Final revision submitted September 2, 2023; accepted September 18, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study received financial support from Arthrex. P.A.S. has received royalties, consultation and speaker fees, and institutional grants and owns intellectual property with Arthrex; owns stock options with Spinal Simplicity; and has received speaker, presentation, and educational fees from Kairos Surgical, United Orthopedics, and Medical Device Business Services. C.A.W. owns intellectual property with and is a current employee of Arthrex, as is his spouse. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Salus IRB (reference No. 406).