
Abstract
Background:
Although recent evidence suggests that any prior shoulder surgery may cause inferior shoulder arthroplasty outcomes, there is no consensus on whether previous rotator cuff repair (RCR) is associated with inferior outcomes after reverse total shoulder arthroplasty (RTSA).
Purpose:
To retrospectively compare outcomes in patients who underwent RTSA with and without previous RCR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with prior RCR and those without previous shoulder surgery (control) who underwent RTSA for cuff tear arthropathy or irreparable cuff tear were retrospectively identified from a prospective database. Exclusion criteria included revision arthroplasty, fractures, rheumatoid arthritis, dislocations, infection, prior non-RCR procedures, less than 12 months of follow-up, and latissimus dorsi tendon transfer. The American Shoulder and Elbow Surgeons (ASES) score, ASES Activities of Daily Living (ADL) score, visual analog scale (VAS) score for pain, Subjective Shoulder Value (SSV), and range of motion (ROM) were compared between groups.
Results:
Patients with previous RCR (n = 83 shoulders) were younger (mean ± SD, 67 ± 10 vs 72 ± 8 years; P < .001) and more likely to be male (46% vs 32%, P = .033) than controls (n = 189 shoulders). No differences were found in follow-up duration (25 ± 13 vs 26 ± 13 months, P = .734), body mass index, or any preoperative outcome variable or ROM measure. At final follow-up, patients with previous RCR had significantly lower ASES (76.5 [95% CI, 71.2-81.7] vs 85.0 [82.6-87.5], P = .015), lower SSV (76 [72-81] vs 86 [83-88], P < .001), worse pain (2.0 [1.4-2.6] vs 0.9 [0.6-1.1], P < .001), and less improvement in the ASES, ASES ADL, VAS, SSV, and forward elevation measures than controls. Multivariable linear regression analysis demonstrated that previous RCR was significantly associated with lower postoperative ASES score (B = –9.5, P < .001), lower ASES improvement (B = –7.9, P = .012), worse postoperative pain (B = 0.9, P = .001), worse improvement in pain (B = –1.0, P = .011), lower postoperative SSV (B = –9.2, P < .001), lower SSV improvement (B = –11.1, P = .003), and lower forward elevation ROM improvement (B = –12.7, P = .008).
Conclusion:
Patients with previous RCR attempts may experience fewer short-term gains in functional and subjective outcome scores after RTSA compared with patients with no history of shoulder surgery who undergo RTSA. However, the differences between groups were small and below the minimal clinically important differences for the outcome measures analyzed.
Reverse total shoulder arthroplasty (RTSA) was developed to treat patients with degenerative glenohumeral arthrosis with rotator cuff insufficiency, and this procedure has been well documented to reduce pain and improve function in such patients. 2,4,16,21 –23,26 Rates of RTSA have increased exponentially over the past decade, 8,17 and RTSA now comprises approximately one-third of all glenohumeral arthroplasty procedures and roughly one-fourth of arthroplasty-treated proximal humerus fractures. 20 This success has resulted in the rapid expansion of RTSA indications and application. 7,15,23,26
Among the expanded indications for RTSA is failed rotator cuff repair (RCR), and many authors have reported satisfactory outcomes of RTSA in such patients. 1,15,23,26 Although recent evidence suggests that lack of prior shoulder surgery is associated with better Simple Shoulder Test scores after shoulder arthroplasty, 12 no consensus is available on whether previous glenohumeral surgery is associated with inferior outcomes after RTSA. 1,15,23,26 Some authors have reported worse outcomes in patients with prior RCR compared with those without, 1 while other authors have found no significant impact. 15,18,23,26 To date, the majority of data on this topic have come from relatively small sample sizes in subgroup analyses within study cohorts. Furthermore, only 1 previous study specifically set out to compare RTSA outcomes between patients with and without prior RCR, concluding that there was no difference between the 2 groups. 18
The potential impact of previous RCR surgery on RTSA outcomes is important for counseling patients and identifying the highest value surgery for elderly patients with large tears. 11 The purpose of this study was to compare outcomes in patients who underwent RTSA with and without previous RCR and to elucidate whether previous RCR is an independent factor associated with clinical outcome. We hypothesized that patients undergoing primary RTSA without a history of previous surgery would have better outcomes compared with patients who had previously undergone RCR surgery.
Methods
Patients
From 2007 through 2014, patients undergoing RTSA by the senior author (J.M.W.) were offered enrollment in a prospective, institutional review board–approved database. Patients were asked to return postoperatively at 3 months, 1 year, and yearly thereafter for radiographic analysis and collection of outcomes data. The database was retrospectively reviewed for patients with a diagnosis of rotator cuff tear arthropathy (CTA), osteoarthritis with rotator cuff tear (RCT), or massive RCT refractory to all other treatments; a minimum of 1-year follow-up; and use of the same prosthesis (Trabecular Metal Reverse Shoulder System; Zimmer). Patients with revision arthroplasty, proximal humerus fractures, rheumatoid arthritis, chronic dislocations, previous infection, prior non-RCR procedures, or concomitant latissimus dorsi tendon transfer were excluded. Patients were then separated into 2 groups: those with prior rotator cuff surgery attempts (previous RCR group) and those without any prior shoulder surgery (control group). All procedures were performed by a single surgeon through a standard deltopectoral approach, and the prosthesis was implanted in accordance with manufacturer recommendations. The senior author repaired the subscapularis tendon at the end of the procedure, unless the subscapularis tendon was deficient preoperatively. Indications for surgery included persistent pain, decreased active range of motion (ROM), and inability to perform activities of daily living (ADL) due to any combination of these symptoms. All patients underwent the same postoperative rehabilitation protocol.
Clinical Evaluation
An independent clinical research nurse examined all patients both preoperatively and postoperatively. Functional outcomes were assessed with the American Shoulder and Elbow Surgeons (ASES) and ASES ADL scores (higher scores indicate better outcomes) 13 ; visual analog scale (VAS) score for pain, where 0 indicates none and 10 indicates the highest possible level of pain; and Subjective Shoulder Value (SSV), in which patients rate their shoulder on a scale of 0 to 100, where 100 indicates completely normal. 5 A standard goniometer was used to measure active forward elevation and active external rotation ROM with the shoulder in 0° of abduction. Body mass index (BMI) was calculated from the medical record. Additional patient demographics were obtained directly from the database.
Statistical Analysis
All statistical analyses were performed with SPSS (v22; IBM). The equal variance and normality assumptions of continuous data were assessed by use of the Levene test and the Shapiro-Wilk test, respectively. Student t tests and Mann-Whitney U tests were used to assess differences in normally distributed and nonnormally distributed independent outcome variables, respectively. Multivariable stepwise linear regression was used to identify independent factors significantly associated with preoperative, postoperative, and change in all continuous outcome variables. Independent predictors were age at surgery, sex (male = 0, female = 1), BMI, time from surgery to follow-up (in months), and previous RCR (no = 0, yes = 1). P values below .05 were considered significant. Aggregate results are reported as mean (95% confidence interval) or mean ± standard deviation (SD).
Results
The study criteria were met by 83 shoulders in 80 patients with at least 1 previous RCR and 189 shoulders in 181 patients without previous shoulder surgery (control group), and these 2 patient groups were used in all final analyses. In the previous RCR group, 44 of 83 shoulders (53%) had undergone surgery for irreparable cuff tears and 39 (47%) had CTA, while the control group contained 117 of 189 shoulders (62%) with irreparable cuff tears and 72 (38%) with CTA (P = .17). Patients with previous RCR were significantly younger at the time of RTSA (67 ± 10 vs 72 ± 8 years; P < .001), and the previous RCR cohort had a higher percentage of males (46% vs 32%; P = .033) (Table 1). Other baseline demographics were similar between the 2 groups (Table 1).
Patient Demographics a

a Results are reported as mean ± SD or n (%). BMI, body mass index; RCR, rotator cuff repair.
b Group numbers refer to number of shoulders.
No significant differences in preoperative values were found for ASES score, ASES ADL score, VAS pain score, SSV, or ROM measures between the 2 groups (Table 2). At final follow-up, previous RCR patients had significantly lower ASES (P = .015), lower SSV (P < .001), higher VAS pain score (P < .001), and less improvement in the ASES, ASES ADL, VAS pain, SSV, and forward elevation measures (Table 2).
Outcomes After Reverse Total Shoulder Arthroplasty for Control Group Versus Previous RCR Group a
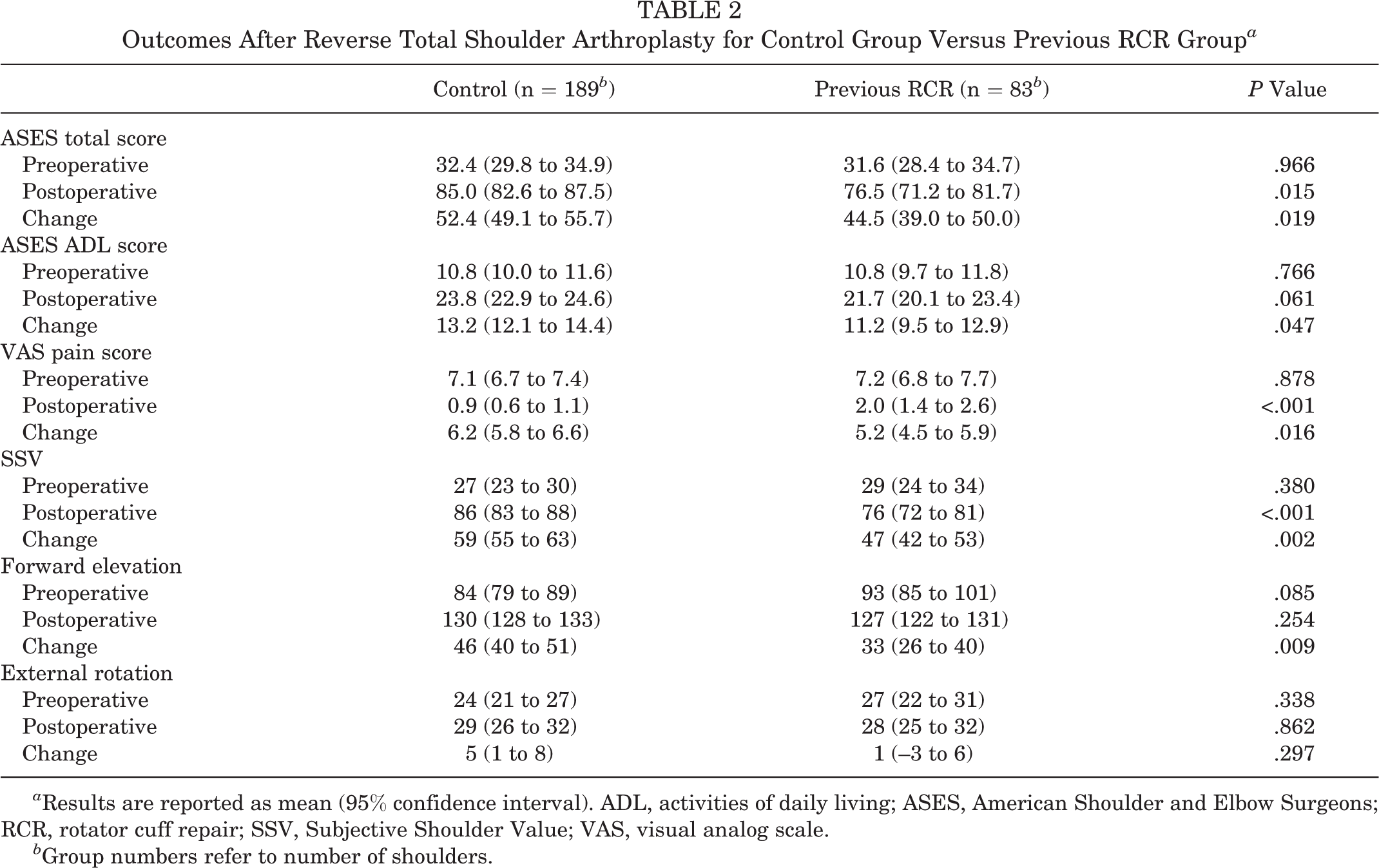
a Results are reported as mean (95% confidence interval). ADL, activities of daily living; ASES, American Shoulder and Elbow Surgeons; RCR, rotator cuff repair; SSV, Subjective Shoulder Value; VAS, visual analog scale.
b Group numbers refer to number of shoulders.
After we controlled for age at the time of surgery, sex, BMI, and time from surgery to follow-up, results from multivariable analysis demonstrated that previous RCR was a significant independent predictor for lower postoperative ASES score (B = –9.5, P < .001), lower ASES score improvement (B = –7.9, P = .012), worse postoperative pain (B = 0.9, P = .001), worse improvement in pain (B = –1.0, P = .011), lower postoperative SSV (B = –9.2, P < .001), lower SSV improvement (B = –11.1, P = .003), and lower improvement in forward elevation ROM (B = –12.7, P = .008) (Table 3). In addition to previous RCR, sex played a role in the ASES and ASES ADL postoperative scores. Patient sex had less of an impact than previous RCR on the ASES score (B = –6.3, P = .010) and a nearly equivalent impact for ASES ADL (B = –2.4, P = .003), with males having higher scores than females in both cases. Age and follow-up were found to have a small impact on postoperative pain and change in pain, respectively. Only 22 of the 83 previous RCR shoulders had more than 1 prior RCR attempt, and with the numbers available, no significant impact on outcomes was found with increased repair attempts.
Effect of Prior RCR on Postoperative Outcomes and Improvement in Outcomes a

a The analysis controlled for age, sex, body mass index, and follow-up length using stepwise linear regression. After these factors were controlled, prior RCR was significantly associated with worse postoperative ASES score and improvement, worse postoperative pain and improvement, lower postoperative SSV and improvement, and lower improvement in forward elevation range of motion. The adjusted difference between groups is indicated by the coefficient B. A negative B indicates lower scores for dichotomous variables (previous RCR, female sex). A negative B for continuous variables (age, follow-up) suggests that for every 1-unit increase in the variable, there is a decrease in the outcome value. A positive B suggests the opposite. ADL, activities of daily living; ASES, American Shoulder and Elbow Surgeons; RCR, rotator cuff repair; Ref, reference; SSV, Subjective Shoulder Value.
The previous RCR group experienced 10 complications (12%), while the control cohort had 21 (11%; P = .82). Complications in the RCR group included 1 intraoperative anterior glenoid rim fracture, 2 postoperative fractures (acromion and scapular spine), 1 dislocation with closed reduction, 2 medical complications (leg deep vein thrombosis, cardiomyopathy), 2 radiculopathies, 1 perineural catheter site infection from continuous interscalene block, and 1 reoperation due to polyethylene dissociation. Patients in the control group experienced 4 intraoperative fractures (1 greater tuberosity, 3 humeral fractures), 2 postoperative fractures (1 humeral shaft, 1 acromion), 4 dislocations treated with closed reduction in emergency room, 4 medical complications (myocardial infarction, renal artery thrombosis, pneumonia, Clostridium difficile infection), 3 instrument complications (broken guide wires), 1 ulnar nerve palsy, 1 superficial cellulitis, and 2 reoperations (1 revision for repeated dislocation and 1 for dissociation of polyethylene).
Discussion
Published reports on the effect of previous RCR on RTSA outcomes are from small patient cohorts and do not provide a clear consensus on whether patients with previous RCR surgery are predisposed to inferior outcomes after RTSA surgery. 1,15,18,23,26 Results from the present study indicate that patients with previous RCR have inferior gains in ASES score, ASES ADL score, VAS pain score, SSV, and forward elevation, with ultimately worse overall ASES, VAS pain, and SSV scores at an average of 2 years after RTSA, compared with patients without previous RCR surgery. Prior RCR did not appear to affect complication rate.
To date, only 1 study has specifically investigated the impact of previous RCR on RTSA outcomes compared with a control group. 18 The investigators compared patients with previous RCR (n = 29) and patients without prior shoulder surgery (n = 39) and found no difference in final outcome scores or complications. Other authors of similarly sized studies have also reported no difference in outcomes after RCR in subgroup analyses. 15,23,26 Contrary to these studies, Boileau et al 1 published a series of 42 RTSAs with previous RCR and documented that these patients had worse outcomes than patients undergoing RTSA without previous RCR. However, data for the controls in that study were not presented and were only mentioned in the discussion, precluding a definitive comparison of quantitative results. The present investigation is the largest study to investigate the effect of previous RCR (189 control shoulders and 83 shoulders with previous RCR), and it was more highly powered to detect differences in gains and final outcomes between the 2 cohorts of interest. This may partially explain why conclusions from our study differ from previous reports suggesting that RCR does not cause deterioration of functional gains after RTSA.
Limited evidence is available regarding why RTSA outcomes would be worse after RCR. Deltoid pressure during arthroscopic surgery is high but returns to normal within 30 minutes after cessation of saline inflow, 9 and Longo et al 10 reported no change in deltoid thickness at a minimum of 1 year after arthroscopic shoulder surgery. However, low rates of partial deltoid detachment (∼2%) and deltoid atrophy (∼5%) have been reported after arthroscopic and open RCR, 3 which could perhaps in large enough cohorts result in mild deleterious effects on the overall average outcome scores. This is important, as both preoperative and postoperative atrophy or fatty infiltration of the deltoid have been correlated with functional outcome scores after RTSA. 6,27 Lower functional scores in patients with prior RCR might also be due to postoperative scarring or even psychological factors related to having a failed procedure and requiring another surgery with another prolonged rehabilitation period. Unfortunately, the main clinical dilemma of how to treat an elderly patient with a large RCT and no or minimal glenohumeral arthritis remains unresolved based on the current literature.
If RTSA after failed RCR truly results in worse clinical outcomes compared with primary RTSA, it may be more cost-effective to perform RTSA in elderly patients with large RCTs. 11 Makhni et al 11 performed a cost-effectiveness study comparing primary arthroscopic RCR versus RTSA in elderly patients with large or massive RCTs. The investigators found arthroscopic RCR to be more cost-effective, assuming RTSA outcomes are not degraded by prior RCR. However, the investigators also conducted a sensitivity analysis showing that RTSA outcomes were reduced by 10% from previous RCR, and this analysis actually suggested that primary RTSA would be more cost-effective in elderly patients with large tears. 11 In our study, prior RCR resulted in a 10% decline in ASES scores and a 12% decline in SSV scores, compared with primary RTSA. Prospective studies of patient outcomes with and without prior RCR, along with advanced imaging of the deltoid pre- and postoperatively, will be necessary in future research to better delineate the best clinical algorithm to maximize outcomes and value.
Although a number of statistically significant differences existed between previous RCR patients and the control cohort, it is important to discuss whether these differences are clinically relevant. The minimal clinically important difference (MCID) for the ASES score with regard to shoulder arthroplasty has been addressed by multiple recent publications. 24,25 Unfortunately, these reported MCID values vary notably: One study suggested that a change or difference as low as 9 points may be clinically significant, 25 while another study found 21 points to be clinically significant. 24 The differences we found between previous RCR patients and controls in postoperative ASES score (8.5 points) and improvement in ASES score (7.9 points) are both just below the 9-point threshold reported by Werner et al. 25 However, when we controlled for patient-related factors, as indicated by the coefficient B in stepwise regression, the postoperative between-group difference in ASES score was adjusted to 9.5, which may indicate a clinically meaningful difference. 25 The MCID for the VAS pain score after shoulder arthroplasty has been reported to be 1.4. 24 Again, the differences we found between the previous RCR and control cohorts for postoperative VAS pain score (1.1 points) and VAS pain score improvement (1.0 points) are below this threshold. The difference between groups for improvement in forward elevation was 13° and is within the published range for the MCID. 14
Although some of the observed differences between the 2 groups in the present study may be below the MCID threshold, the difference in function compared with the average, normal-functioning shoulder may demonstrate clinically inferior outcomes in the previous RCR group. The mean normative ASES score has been reported to be approximately 92 points. 19 This is a 15.5-point difference from the previous RCR group (mean score, 76.5), which is well within the range of an MCID. Conversely, the control group had an ASES score of 85, or only 7 points lower than a healthy shoulder and well below any reported MCID of the ASES for shoulder arthroplasty.
This study is weakened by a number of limitations. The retrospective nature of the study generates the potential introduction of bias in our results, despite the data being collected prospectively. Some data regarding surgical history were obtained only through patient history, and it is possible that some patients incorrectly reported their previous surgical procedures or the number of previous repairs. Data regarding open versus arthroscopic repair involving the glenohumeral joint were not recorded in the database. The database also does not include information on workers’ compensation, litigation, or automobile insurance. These groups have secondary gain issues that have been shown to negatively affect outcomes. That both groups had such similar baseline functional data may indicate that any secondary gain issues were balanced between the groups. Additionally, baseline age and sex distribution were different between the groups. However, when we controlled for age and sex in the multivariate analysis, previous RCR remained a significant predictor for worse ASES scores. 19
Conclusion
Patients with previous RCR may experience inferior clinical outcomes and fewer short-term gains in functional and subjective outcome scores compared with patients who have no history of shoulder surgery after RTSA. However, the differences between groups were small and were below the MCID for the outcomes measures analyzed.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: J.M.W. receives consulting fees from Zimmer-Biomet, DePuy-Synthes, and Wright Medical; royalties from Smith & Nephew; and research support from Donjoy Orthopaedics, DePuy-Synthes, Zimmer-Biomet, and Wright Medical.
Ethical approval for this study was obtained from Beaumont Health System Institutional Review Board (protocol No. 2006-088).