
Abstract
Background:
High school sports participation in the United States has increased dramatically over the past 25 years. A corresponding increase in the number of injuries has been noted, particularly in contact sports such as football. This has led medical and sports organizations nationwide to advocate for proper medical supervision of athletes at games and practices.
Purpose:
To gather information from Chicago public high schools to gauge how medical supervision for high school sports has changed in 2017 compared with 2003.
Study Design:
Cross-sectional study.
Methods:
Survey questionnaires were sent to the athletic directors of all 99 Chicago public high schools to complete via email. The questionnaire survey contained the same questions as in a survey conducted in 2003 by Tonino and Bollier, with the addition of 4 novel questions relating to emergency action plans (EAPs), automated external defibrillators, concussion management policy, and tackling progression drills.
Results:
The response rate was 66.67% (66/99 schools). Of the 66 responding schools, all with football programs, no school had a physician on the sideline at home games (decrease from 10.6% in 2003), 37.9% had an athletic trainer present (increase from 8.5% in 2003), and 63.6% had a paramedic available (decrease from 89.4% in 2003). In 2017, 65.6% of responding schools had a coach certified in cardiopulmonary resuscitation (CPR) available at practice to handle medical problems, compared with 89.4% in 2003 (P < .001). Regarding the 4 novel questions, 93.9% of the responding schools had proper tackling progression drills in place, followed by 89.1% who had appropriate EAPs and 93.9% with concussion management protocols, including return-to-play and return-to-learn protocols.
Conclusion:
Although significant improvement was found in athletic trainer coverage, especially at games, physician coverage was lacking and fewer coaches were certified in CPR in 2017 compared with 2003. EAPs and concussion management protocols were present in most Chicago public high schools. Overall, greater medical supervision is needed, which we believe should come in the form of increased athletic training and physician involvement and coverage, given that expert, expedited medical care saves lives.
Keywords
The past 25 years have seen a significant increase in student participation in high school athletics, from an estimated 4 million participants 1971-1972 to 7.9 million in 2015-2016. 8,22 Prior studies have revealed that 2 million injuries, 500,000 doctor visits, and 30,000 hospitalizations occur each year among high school athletes. 8 Specifically regarding the risks of high school sports, high school athletes have 3 times as many catastrophic football injuries as college athletes, which likely has to do with the greater number of participants and the relative inexperience of high school athletes. 5 Athletic trainers (ATs) and other health care providers, including physicians, are on the frontlines of addressing this increase in injury burden. To provide appropriate medical coverage of this ever-increasing number of high school athletic events, the National Athletic Trainers’ Association (NATA), the American Academy of Family Physicians, and the American Medical Association encourage schools to consider employing certified ATs as opposed to relying on coaches, who often are inadequately prepared or trained to deal with medical emergencies. 1,9,14,17 ATs are trained to quickly handle emergency situations in an athletic environment, such as heat stroke, diabetic events, concussions, spinal cord injuries, and sudden cardiac death. 7 In most of these emergency situations, timeliness is of the essence and can signal the difference between life and death. For example, in the case of heat illness, early recognition and appropriate treatment are vital for favorable outcomes. 4 Other recommendations include providing access to automated external defibrillators (AEDs), creating and implementing emergency action plans (EAPs), and providing medical coverage at all sporting events. 1,2,7 Despite such recommendations, most states lack formal legislation related to medical care at sporting events in secondary schools. 1 The NATA states that appropriate policy and staffing may reduce the number of life-threatening events in secondary schools. 7 In addition to the employment of appropriately trained personnel, implementation of a written EAP detailing standard of care during emergency situations at venues is of vital importance. 2,6,7,10,21,23 EAPs define roles and help guide actions for emergencies and require the availability of lifesaving equipment, such as AEDs. 7,10 For example, in sudden cardiac arrest, prompt implementation of the EAP and cardiopulmonary resuscitation (CPR) and rapid defibrillation with the help of an AED have been shown to be critically important. 7,10,28,34 EAPs improve response time, and survival rates after ventricular defibrillation decrease around 10% for every minute defibrillation is delayed. 16,31,34 A prior study showed that the mere presence of an AT was associated with higher rates of EAP implementation. 17
The increases in high school athletic participation and subsequent injuries have led to strong recommendations for sideline medical coverage by multiple medical organizations. This study set out to investigate the current state of medical sideline coverage during games and practices in Chicago public high schools 1,9 and determine any changes in medical supervision from 2003 to 2017.
Methods
This study was declared exempt by our institution board. The lowest amount of risk was afforded to those we surveyed, as the collection was anonymous.
Survey and Instrumentation
A survey (Appendix 1) was created using questions similar to those in a survey conducted in 2003 by Tonino and Bollier 33 (Appendix 2). To address the new laws and requirements, we added 4 supplemental questions pertaining to EAPs, AEDs, and concussions. Questions were also changed to include all sports coverage, with some questions directed to football. Although the 2003 questions addressed football specifically, the generalizability of the 2017 questions did not affect the data analysis because coaching requirements are consistent across sports. The survey was prepared in an electronic online format via an institutionally approved survey platform account. The electronic survey was meant to encourage participation and reduce mailing costs. The survey requested information about the personnel available to assess medical problems at home football games and at practices, and it also sought information about CPR and first aid certification of these staffers. In addition, the 2017 survey gathered information on tackling progression drills instruction, EAPs, and concussion management protocol, none of which were required by schools at the time of the 2003 survey.
Participants
A complete listing of the 99 Chicago public high schools was obtained via the Chicago Public Schools website (https://cps.edu). The survey was sent electronically to all 99 Chicago public high school athletic directors, with a follow-up reminder email sent 1 month later. A total of 66 schools completed the survey. Electronic survey responses were automatically and anonymously compiled by the institutional electronic survey platform. An institutional statistician was able to extract anonymous raw data and compile responses from the institutional electronic survey platform for statistical analysis.
Data Analysis
Responses to the 2003 and 2017 medical supervision surveys were assessed as independent observations for this analysis. This approach accounted for the 14-year gap between administrations, during which personnel changes and cultural shifts about player safety are well documented. All response options were discrete in nature, presented as either a binary choice (yes/no) or a “select all that apply” list. As such, frequencies and proportions for each survey item are reported by year, and Pearson chi-square tests were used to assess for statistically significant differences. In the event expected cell counts fell below 5, Fisher exact tests were used instead. For the supplemental questions in the 2017 survey, no additional comparisons were possible, so raw response totals are reported. An alpha error rate of P ≤ .05 was considered statistically significant, and all analyses were conducted with SAS software, version 9.4 (SAS Institute Inc).
Results
A robust response rate was obtained, with 66 of the 99 schools participating (66%). 11 Comparison of football home game coverage for 2003 versus 2017 revealed that a greater proportion of Chicago public high schools had ATs (P < .001) and an ambulance (P = .04) on the sidelines at home games in 2017 (Table 1). By contrast, a smaller proportion of Chicago public high schools had a physician (P = .03) or paramedics (P = .002) on the sidelines at home games in 2017.
Who Is Available for Medical Problems at Home Games and Sideline Coverage? a
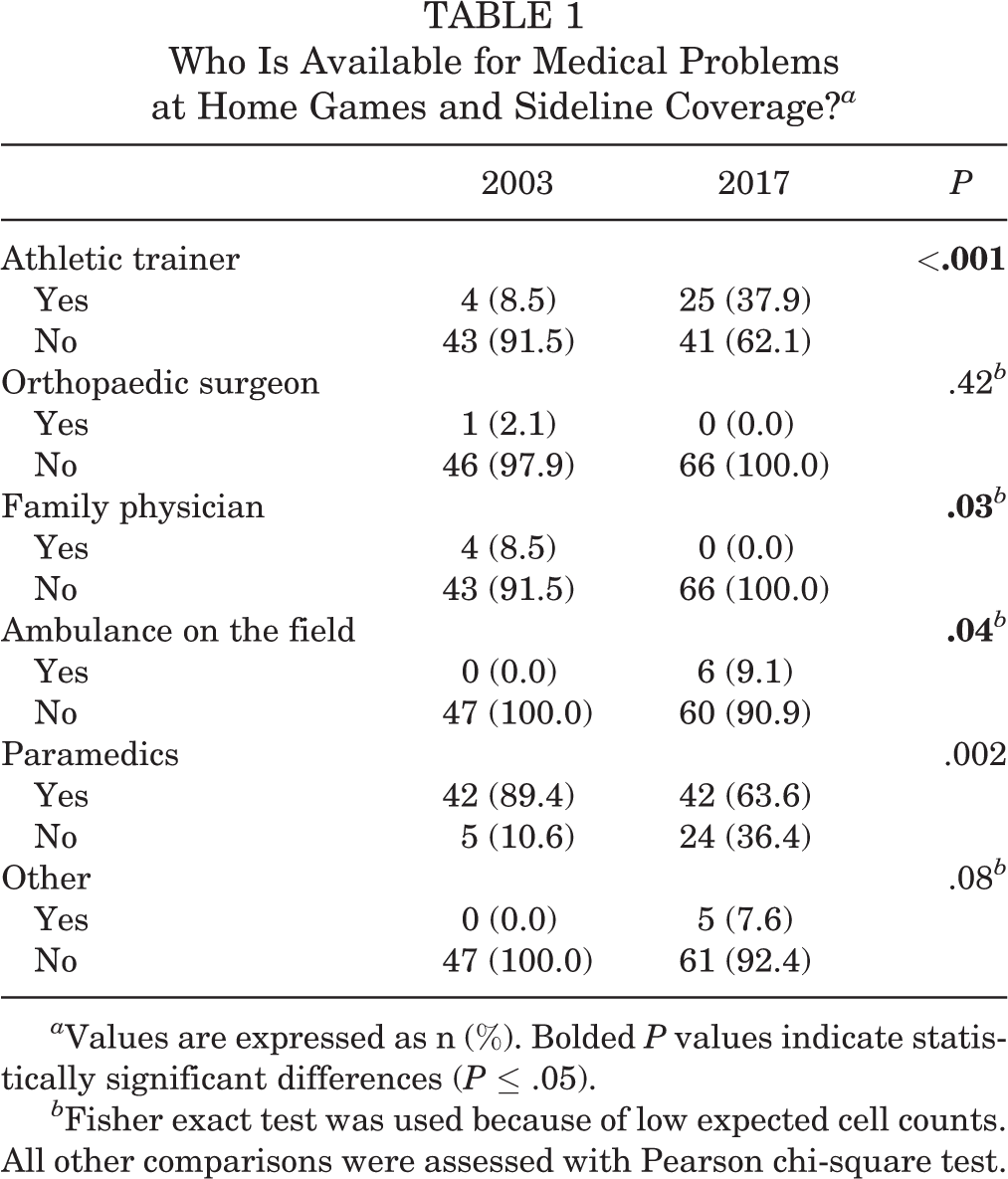
a Values are expressed as n (%). Bolded P values indicate statistically significant differences (P ≤ .05).
b Fisher exact test was used because of low expected cell counts. All other comparisons were assessed with Pearson chi-square test.
Comparison of football practice coverage for 2003 versus 2017 (Table 2) showed that a smaller proportion of Chicago public high schools had head coaches certified in CPR or first aid at football practices (P < .001) in 2017. A greater proportion of Chicago public high schools also reported having “no one” on hand to address medical issues at practice (P < .001) in the 2017 survey. A decrease in coaches certified in CPR was noted as well (P = .004) (Table 3).
Who Is Available for Medical Problems at Practice? a

a Values are expressed as n (%). Bolded P values indicate statistically significant differences (P ≤ .05).
b Fisher exact test was used because of low expected cell counts. All other comparisons were assessed with Pearson chi-square test.
Are Coaches Certified in Cardiopulmonary Resuscitation and First Aid? a

a Values are expressed as n (%). Bolded P value indicates statistically significant difference (P ≤ .05). All comparisons were assessed with Pearson chi-square test.
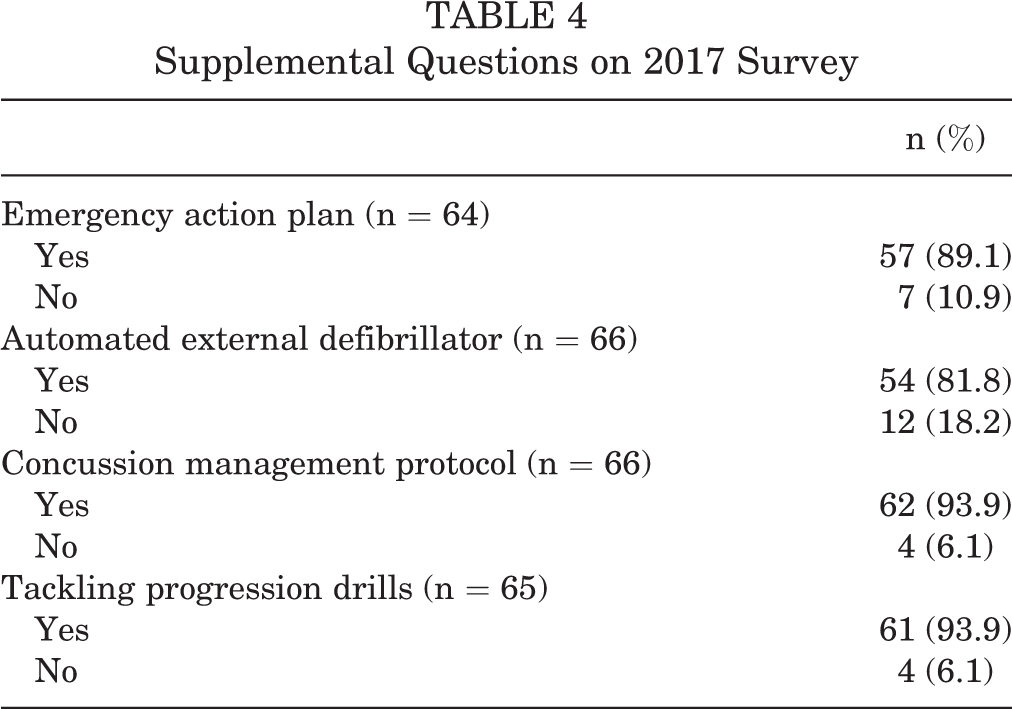
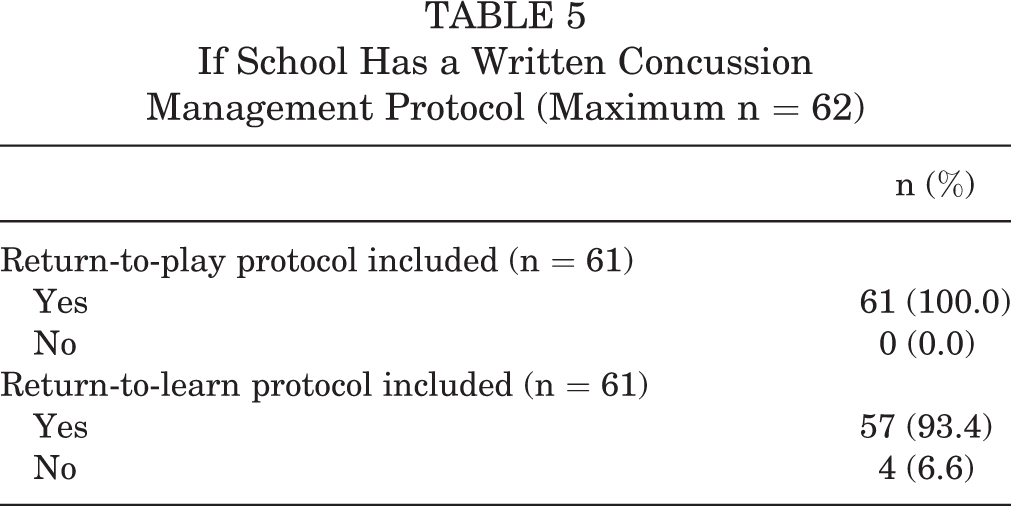
Responses to the supplemental questions in the 2017 survey revealed that 89.1% of the respondent schools had EAPs and 81.8% had AEDs (Table 4). Similarly, 93.9% of schools had protocols in place for football progression drills where athletes are taught to tackle safely. The same proportion (93.9%) of schools also had concussion management protocols, with 100% of schools having return-to-play protocols and 93.4% having return-to-learn protocols (Table 5).
Supplemental Questions on 2017 Survey
If School Has a Written Concussion Management Protocol (Maximum n = 62)
Discussion
In this study, we aimed to assess the current state of medical supervision in the Chicago public high schools and compare it with findings from similar studies. We found a few other national studies that have assessed physician and certified AT presence on the sideline. ‖ In 1980, Porter et al 26 looked at both private and public high schools and found that only 42.4% of schools had a physician on the sideline. When these investigators looked specifically at Chicago public high schools, physicians were found to be on the sideline 12.5% of the time and ATs 10% of the time. In 2003, Tonino and Bollier 33 evaluated Chicago public high schools and found that only 10.6% of schools had physician coverage at home varsity football games and that ATs were present in only 8.5% of schools. Tonino and Bollier did not note a difference in physician and AT coverage between 1980 and 2003.
Now, almost 40 years later, we find that there remains a significant lack of physician and AT coverage in Chicago public high schools compared with national surveys. 24,25,27 In both 2003 and 2017, survey findings suggest that coaches bear the brunt of medical supervision, especially in the practice setting. This stems in part from a persistent belief that a coach can provide medical care in the place of ATs. 19 Studies have shown a low level of knowledge by coaches concerning health-related issues such as management and recognition of concussions, first aid, and hydration strategies. 12,13,20,29 Coaches do not receive the appropriate training or education to handle such emergency situations. In fact, our study showed a decrease in the number of coaches certified in CPR from 2003 to 2017, which is of concern when schools rely on coaches as the first line of care. Despite the decrease in coaches certified in CPR, 65.6% of coaches in Chicago public high schools had this certification. This is an impressive result compared with a recent survey in rural West Virginia 32 showing only 33% of coaches with CPR training and a 2014 study in Wisconsin 14 that found only 50% of coaches with CPR certification. These findings could be attributable to differences in state requirements, given that no federal regulation or requirement is currently in place.
Our study showed that of the 66 Chicago public high schools that responded, almost 90% have EAPs in place, which is in line with the NATA 2002 recommendation. 2 A 2015 study in Ohio showed that only 16% of schools had EAPs. 18 A similar study found that only 38% of West Virginia schools had EAPs, 32 while a study from Oregon found that only 28% of schools had implemented EAPs and ready access to AEDs. 17 Implementation of an EAP has been shown to decrease risk of death in athletes. 2 The mere presence of a certified AT at a school increases the rate of EAP implementation. 17 EAPs help define roles and appropriate actions for emergencies, while instructing personnel in the lifesaving equipment necessary to carry out the plan. For instance, in the case of sudden cardiac arrest, the condition must be immediately recognized, followed by EAP activation, early CPR, and defibrillation with an AED. An AT is best positioned to execute the EAP in this situation.
Return-to-Play Decisions
A recent study of high school students in California revealed that medical return-to-play decisions were made by non–health care professionals, and nearly 40% of surveyed schools did not refer injured athletes to physicians for follow-up evaluation. 30 The presence of a health care professional, such as an AT or physician, would be of great value for these complex return-to-play decisions.
Our study showed an increase in AT presence at practice as well as games and competition in 2017 compared with 2003. A recent national study looking at athletic training services in public secondary schools found that 70% of high schools provided some sort athletic training services but only 37% were full-time. 27 A study looking at private secondary schools found that 58% had varying levels of athletic training services, with a fraction (28%) being full-time. 24 An study from Oregon found 50% AT availability on the sideline, 17 and in a North Carolina study, 3 56% of schools surveyed had AT presence. Given these reported numbers, Chicago public high schools still lag behind in terms of AT coverage. The reason for this lag is likely multifactorial and involve issues such as budgetary constraints, school size, and lack of awareness of the AT’s role, although we did not specifically inquire about these factors in our study. 25,32 One possible solution would be to employ teachers who are also ATs. Instead of the common practice of a teacher coaching after school, a dually trained teacher-AT could provide sideline coverage at practice and games after class.
A study from North Carolina found that 71% of athletic events were covered by physicians, 3 which appears to be higher than average, especially compared with our survey of Chicago public high schools. Lack of volunteer physicians on the sideline is also multifactorial, with possible reasons including lack of sideline coverage experience, concern for medical liability, and noncompensated time. 33 Some of these issues may be resolved with legislation at a state level covering physicians’ malpractice when they serve in the capacity of sideline physicians. Also, increasing musculoskeletal training and sideline coverage experience in medical school and residency could greatly increase physician comfort level. 33
Even though the results of our survey are self-reported, our survey revealed several positive findings. We found that a high percentage of coaches (93.9%) provided education in proper tackling techniques. This education addresses calls to avoid illegal tackles such as spear tackling and contributes to overall injury prevention. 15 We also noted that almost all (93.9%) of the Chicago public high schools have a concussion management protocol that includes not only a return-to-play protocol but also an equally important return-to-learn protocol. The high presence of concussion management protocols and the low AT and physician availability beg the question of who is managing the return-to-play decisions. A future study could answer such questions.
Conclusion
We found a decrease in CPR training among coaches over the 14-year time period assessed in this study, and most schools had EAPs and protocols for return-to-learn and return-to-play after concussion in 2017. However, given the decrease in sideline medical supervision, appropriately trained staff who can best implement EAPs and concussion protocols are lacking. Continued improvement is needed with regard to medical supervision on the sideline. Future studies could look at different ways to increase the medical supervision coverage while addressing the barriers that are at the core of our present shortfall.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: P.M.T. has received consulting fees from ConMed Linvatec and hospitality payments from DePuy Orthopedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Loyola University Chicago.
Notes
Appendix 1
To: Athletic Director
From: Orthopedic Surgery Department
We are researching the availability of medical coverage for high school athletic events and would like to know if you have a doctor or other medical professional on the field during sporting events/games.
Please indicate if you have coverage and who provides such service at your school. Please check all the choices that apply for your school. At our home games, we have the following on the sidelines: – Athletic trainer ___ – Orthopaedic surgeon ___ – Family doctor ___ – Pediatrician ___ – Physician (other specialty) ___ – Chiropractor ___ – Ambulance on the field ___ – Paramedic ___ – Other (please describe) ___ – None (please list who would initiate medical care; eg, coach) ____ At practice, who is available for medical problems? – Athletic trainer ___ – Physician ___ – Coach certified in cardiopulmonary resuscitation (CPR) or first aid ___ – Paramedic ___ – Other (ie, school nurse) ___ – No one ___ Are your coaches certified in CPR? Yes___ No___ Are your coaches certified in basic first aid? Yes___ No___ Does your school have a written emergency action plan (EAP)? Yes ___ No ___ Does your school have an automatic external defibrillator (AED) on site? Yes ___ No ___ Does your school have a written concussion management protocol? Yes____ No____ If yes, does it include a return-to-play protocol? Yes ___ No ___ Also, if yes, does it include a return-to-learn protocol? Yes ___ No ___
Schools with football: 8. Does your school have tackling progression drills where players learn how to tackle properly and safely? Yes____ No ____ N/A ____
Individual schools’ results will remain anonymous to the public, but we would be happy to supply a summary of our findings if you desire.
Thanks for participating in the project and good luck this season.
Appendix 2
To: Athletic Director
From: Orthopedic Surgery Department
We are researching the availability of medical coverage for high school athletic events and would like to know if you have a doctor or other medical professional on the field during your home football games.
Please indicate if you have coverage and who provides such service at your school. Please check all the choices that apply for your school.
At our home games, we have the following on the sidelines:
—Athletic trainer
—Orthopaedic surgeon
—Family doctor
—Pediatrician
—Chiropractor
—Ambulance on the field
—Paramedic
—Other (Please describe)
Are your football coaches certified in cardiopulmonary resuscitation (CPR)? Yes__ No__
Are your football coaches certified in basic first aid? Yes__ No__
At football practice, who is available for medical problems?
—Athletic trainer
—Physician
—Coach certified in CPR or first aid
—Paramedic
—No one
We would be happy to supply a summary of our findings if you desire.
Thanks for participating in the project and good luck this season.