
Abstract
Studies of professional American football players have shown that football-related activities lead to acute injuries and may have long-term adverse health outcomes including osteoarthritis, neurocognitive impairment, and cardiovascular disease. However, the full complement of what constitutes professional football exposure has yet to be effectively articulated. Most likely, professional football exposure encompasses a multifaceted array of experiences including head impacts and joint stresses, long-term pain medication use, dietary restrictions, and strenuous training regimens. To study the health of professional American football players, characterizing the group as an occupational cohort and taking advantage of methods established within the discipline of occupational epidemiology may be beneficial. We conducted a narrative review of existing football research, occupational epidemiological methods papers, and occupational medicine studies. Here we describe the traditional occupational epidemiological approach to assessing exposure in a novel cohort and show how this framework could be implemented in studies of professional football players. In addition, we identify the specific challenges associated with studying an elite athletic occupational group, including the healthy worker effect and other types of selection and information biases, and explore these in the context of existing studies of football-related health. The application of well-established occupational epidemiological methods to professional football players may yield new insights into the effects of playing exposure and may provide opportunities for interventions to reduce harm.
Keywords
A wide spectrum of health issues has been documented in former professional American football players, including cognitive dysfunction, neuroanatomical changes, joint injuries, and cardiovascular disease. For example, concussions in National Football League (NFL) cohorts have been associated with increased risk of depression 18,29,66 and cognitive impairment. 2,28,67,90 Although some studies have shown increased longevity in football players compared with a general sample from the United States (US) population, 1,41,44,46 increased neurodegenerative (eg, Alzheimer disease, Parkinson disease) 44 and cardiovascular 5 mortality has been found when compared with the US population. Taken together, these results imply that exposure to professional football may be causally associated with deleterious health outcomes despite observed associations with increased longevity.
To fully capture the health-related effects of playing American football, it is critical that investigators accurately identify the constellation of exposures to which participants are subjected. Importantly, some acute football play–related outcomes such as head and joint impacts and stresses may serve as exposures for future outcomes including cardiovascular 53 and neuropsychiatric disease. 29,39,66 Although many studies conducted on football players have yielded important insights, questions remain regarding the relationship between football-related exposures and disease. 43 This may be because quantifying football exposures is a complicated task: Relevant events may have occurred decades ago, and disparate activities by position may have unique impacts on health. We propose that occupational epidemiology offers a useful framework that can expand upon previous findings in football players. A systematic exploration that identifies high-risk aspects of football play would be of significant interest to football players and families, clinicians, youth and collegiate players, coaches, and other stakeholders.
Occupational epidemiology studies the relationship between workplace exposures and injury and disease. The method developed for this subdiscipline systematically defines exposures, classifies worker subgroups, and identifies sources of bias. 12 The primary objective of occupational epidemiology is to protect the health and safety of workers. Secondarily, it seeks to safeguard the general population to the extent that the exposures under study may also occur in the public. Exposures and outcomes associated with football, such as concussions and joint injuries, also occur in the general population and during athletic activities, so knowledge gained from such a professional cohort could be applicable beyond NFL players. However, successful prevention depends on establishing direct connections between specific exposures and harmful outcomes; it is far more difficult to mitigate a harmful outcome when its exact cause is unknown. Given that many adverse health outcomes in professional football players have not yet been shown to be directly associated with specific football-related activities, using a traditional occupational epidemiological approach to defining football exposure could yield actionable insight.
Occupational Epidemiological Approaches to Exposure Assessment
Historically, occupational epidemiology has focused on chemical or environmental hazards in the workplace, such as exposure to asbestos and heavy metals. Over time, the definition of exposure in occupational epidemiology has expanded to include physical hazards, such as repetitive knee stress experienced by carpet layers, 79 strenuous patient transfers in nursing, 84 and injuries in professional athletes such as football players. 5,20 An occupational epidemiologist initiating a study would engage in the following: (1) cohort surveillance to describe the occurrence of illness and injury; (2) exposure assessment, where putative exposures of interest are measured in subgroups of workers; (3) hypothesis testing to determine whether specific occupational exposures are hazardous; and (4) evaluation of an intervention by measuring changes in health status over time. Figure 1 presents a generalized workflow for an occupational cohort, as adapted from several sources. 12,36,58

Occupational epidemiological framework for cohort characterization.
Briefly stated, if outcome prevalences gathered during surveillance (Figure 1, A) are elevated when compared with a general population, an occupational epidemiologist will begin exposure assessment (Figure 1, B). Next, subgroups expected to experience homogeneous patterns of exposure are designated (Figure 1, B.2). When evaluating possible data resources (Figure 1, B.3), investigators use professional expertise to anticipate bias and to assess data collection quality and feasibility. Occupational epidemiologists then collect data (Figure 1, B.4), test hypotheses, and explore dose-response relationships (Figure 1, C). In the final stage, preventive measures and interventions are tested such that reductions in injury or disease rates can be evaluated (Figure 1, D). Interventions may be guided by the hierarchy of hazard control, 55 which prioritizes hazard reduction or elimination strategies (Figure 2, left). Typically, a common stop-gap approach to mitigating risk is improved personal protective equipment. 49 Seen as more effective, administrative controls (changing the way people interact with the hazard) and engineering controls (isolating workers from the hazard) can be implemented. Finally, the most protective strategies to risk reduction include hazard substitution and hazard elimination (Figure 2, left).

The hierarchy of control framework (left). Application to recent professional football interventions and safety measures (right). Adapted from the Hierarchy of Controls, National Institute for Occupational Safety and Health. 55 PPE, personal protective equipment.
The strategy for exposure assessment (Figure 1, B) and hypothesis testing (Figure 1, C) in an occupational epidemiological investigation depends on whether a putative causative agent has been named at the start of the study. When a specific exposure of interest has not been identified, occupational epidemiologists conduct exploratory analyses using surrogate variables or exploring outcomes by job type. Surrogate or proxy variables are measurable, exposure-related factors or biomarkers that are expected, but not guaranteed, to correlate with a known exposure. 58 Surrogate exposures include the “ever- or never-employed” dichotomy (where participants who have any employment history are contrasted with those who have no employment history) or employment duration of employment as a means of initially exploring exposure-outcome associations.
Alternatively, investigators may initiate an occupational study with a specific hypothesis in mind. Known as a priori hypotheses, these assumptions are often based on biological mechanisms that link a specific exposure to an outcome. The process of inquiry may resemble that for exploratory analyses outlined above or may first examine jobs or tasks expected to result in high levels of the hypothesized exposure of interest. This may be combined with targeted direct measurement studies to confirm that the groupings are indeed highly exposed; such studies are typically conducted in a subset of workers because of cost and time concerns. Evidence from these smaller studies can be used to construct job-exposure matrices (JEMs), which systematically assign levels of exposures to specific jobs so that exposures can be inferred from job titles. The advantages of JEMs are that they can applied to a specific occupational group or across an entire industry and that they may reduce exposure misclassification because exposures are similarly applied to participants with and without the outcome. 37 When one is attempting to link putatively hazardous exposures to adverse health outcomes, the selection of surrogate variables will depend on both the type and stage of a study and will also inform generalizability of findings.
Applying an Occupational Epidemiological Framework to the NFL
To a limited extent, the methodological framework outlined above has been applied to professional football. Studies have explored the prevalence of football-related injuries and other adverse outcomes, including concussion, 9,60 joint injuries, 10,19,88 opioid use, 14 hypertension, 80 suicide, 45,86 and cognitive impairment. 67 Often, these and other surveillance studies did not define football exposure in specific terms but rather broadly used study participants’ status as active or former football players to represent all relevant exposures. 2,5,11,80 In addition to the ever-employed/never-employed approach, some studies quantified exposures such as concussions by using either the number of self-reported concussions 18,28 or an index that combined concussion-relevant parameters. 90 Years of play 8,52 and number of seasons or games played have also been used in analyses. 20 Other studies have explored how playing position 5,16,43,60 or weight gain 13 are associated with later life outcomes. Tailoring the steps of exposure assessment methodology for professional American football players would include (1) translating the full complement of football-related activities into quantifiable exposures, (2) identifying subgroups (eg, playing position), (3) assessing the data quality and opportunities for bias; and (4) implementing optimal assessment methods for contemporary and historical exposures.
Figure 3 maps potential exposures and outcomes experienced over the life-course of a football player that may be relevant for football health studies, as well as confounding variables and mediators. These can be divided into preprofessional, professional, and postretirement periods. Professional football can be further broken down into game-related exposures such as total seasons, snaps, and positions. Acute injuries may occur, such as concussions, joint injuries, and fractures. Some acute injuries or outcomes can act as mediators, increasing the risk of long-term outcomes such as arthritis, cognitive impairment, chronic pain, sleep disorders, neurodegenerative disease, and hormonal dysfunction. Finally, behavioral health factors such as smoking and alcohol use, adult socioeconomic status, and exercise may modify risk of acute or long-term outcomes.
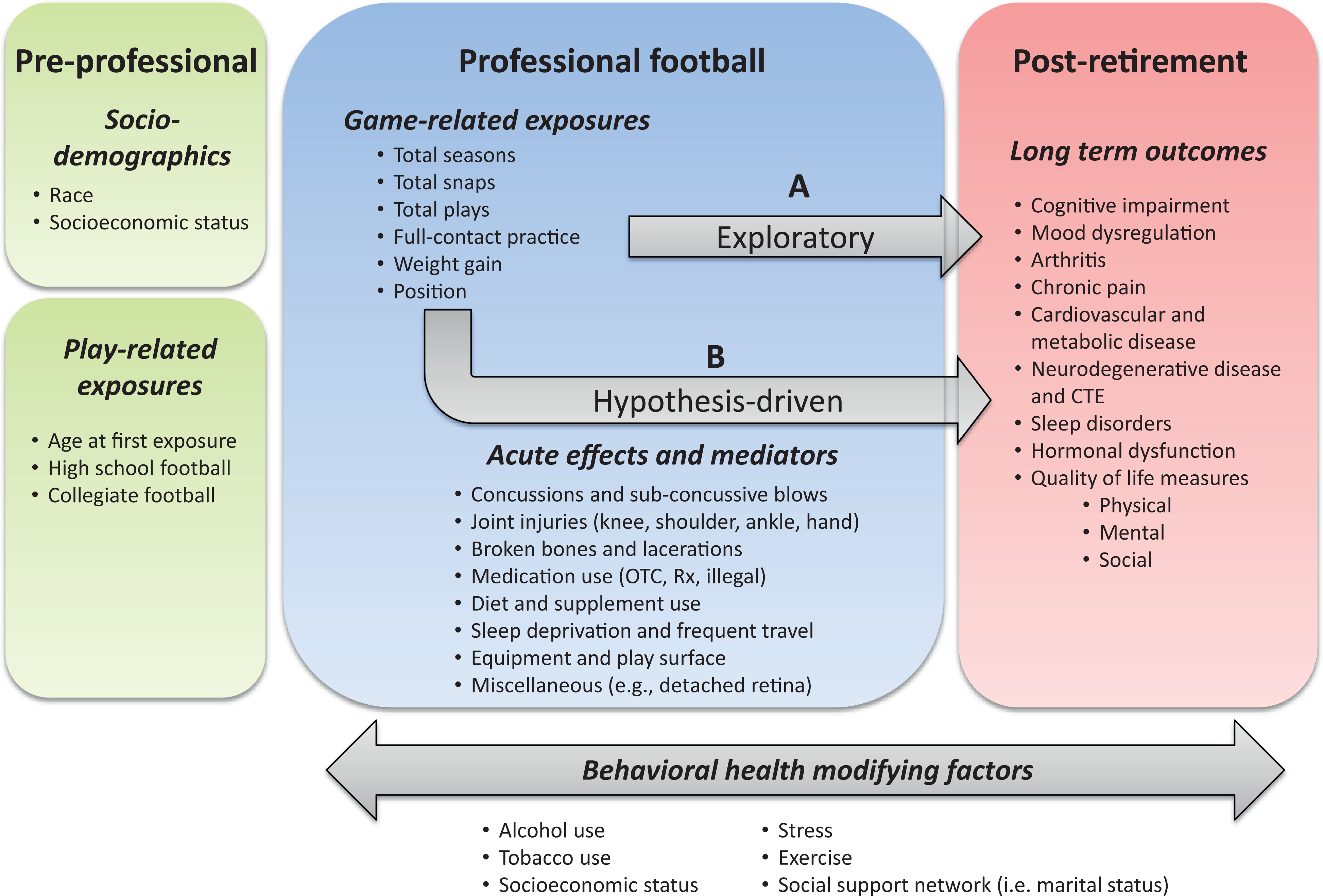
Defining exposures, mediators, and acute and long-term outcomes for a professional football cohort. Exposures and outcomes are divided by life stage, including preprofessional, professional, and postretirement. CTE, chronic traumatic encephalopathy; OTC, over the counter; Rx, prescription.
Playing position represents one of the most relevant subgroup classifications in professional football and is defined by a player’s functional role within the game. Some positions, such as wide receivers and running backs, are typified by speed and agility. Some require greater size and strength, such as seen in defensive and offensive linemen, while kickers, punters, and quarterbacks are defined by skillset. Position may also serve as a surrogate variable for amount of time on the field per game, career length, and training regimen. Modeled after the job exposure matrix, a football-specific position exposure matrix (PEM) could be created that reflects the typical exposures at every football position. A PEM would incorporate types and magnitude of impacts, training regimen information, and other position-specific exposures that could be applied generally across all football players. Over the course of their high school, collegiate, and professional careers, players may play multiple positions, complicating the approaches to exposure assessment. Other potential subgroup divisions include era of play before and after rule or safety equipment changes, as well as team membership.
Confounders should also be taken into consideration to effectively disentangle health effects attributable to professional football versus those resulting from preprofessional factors. For example, confounding could be caused by factors related to youth football participation, which has been associated with later neurocognitive function and neuroanatomic status. 75,76 Confounding could occur if professionals who played football when they were young accumulated more injuries but also were more likely to be hurt once in the NFL. Pre-NFL physical attributes can serve as another confounder: Large physical size offers a critical advantage for defensive linemen yet may put them at increased risk for some cardiovascular outcomes. 5
In terms of preventing injuries in professional football, many recent safety-motivated changes have occurred at the personal protective equipment end of the hierarchy of controls framework 55 (Figure 2, right). For example, helmets and mouthguards have been upgraded over recent years in an effort to reduce concussions. 17,83 Administrative controls in the form of rule changes have been implemented to alter the way football players interact on the field. For example, the NFL currently penalizes players for unnecessary roughness, 56 such as using the helmet to ram another player (the “crown-of-the-helmet rule,” or CHR) or hitting or launching at a defenseless player. 54 Preliminary research on the CHR has shown a reduction in concussions but also an increase in lower extremity injuries. 31 In 2011, the NFL returned kickoffs to the 35-yard line after a previous shift to the 30-yard line. 81 Although overall injuries were significantly reduced after this rule change, head injuries were not. 70 In 2018, the NFL mandated that instead of taking a running start, players on the kicking team must be stationary before kicking the ball to presumably reduce the velocity at contact. Other administrative controls include mandating preseason concussion education and baseline examinations, designating unaffiliated medical advisors to perform concussion evaluations of head-injured players, 24 and prohibiting concussed players from returning to the field. As an engineering control, remote-controlled robotic tackling dummies have been introduced during tackle practice. 59 Examples of substitution or elimination controls in professional football could include replacing tackle football with the less injurious flag football. 26,62
Bias in Studies of Professional Football Players
Studies of football players’ health are likely to be susceptible to biases due to the nature of football as an elite athletic pursuit and the types of data that must be collected. Although eliminating all bias is challenging, many sources of bias can be avoided at the study design phase or addressed during data analysis. Biases relevant to professional football data include selection bias, loss-to-follow-up bias, and information bias such as recall bias.
Healthy Worker Effect and Healthy Worker Survivor Bias
A type of selection bias called the healthy worker effect (HWE) may play a large role in studies of professional football and health. HWE refers to the phenomenon in which individuals who gain and maintain employment appear healthier compared with a general population. 12 For elite athletes, the HWE stems from two related phenomena: (1) the healthy hire effect, where healthier candidates will be preferentially hired as professional athletes; and (2) healthy worker survivor bias, where players who remain fit continue employment while those with illness or injuries stop playing. 47,48 When not taken into account, the HWE can produce paradoxical results because the relatively lower rates of mortality and morbidity in a working population compared with a general population can obscure additional increased risk stemming from occupational exposures. One study on the HWE found that professional football players had an average of 6 years of increased longevity over age-matched general controls. 1 This longevity increase has been seen in a number of other professional sports studies 5,25,41,44,46 and has been used in mainstream media to suggest that football exposure is minimally hazardous. 22,23
Comparison Group and Matching Factor Selection
Relevant to the HWE, it is important to note that elite college athletes have far better than average fitness before joining the NFL. To effectively study the isolated effects of playing professional football, investigators should preferentially use a comparison group of men with similar fitness to football players, such as other professional athletes. This approach would control for non-football-specific factors known to affect longevity, such as the positive physiological effects of regular exercise. 1 Problematically, most football longevity studies use the general US male population as a comparison group to investigate NFL player health. Authors often have adjusted or matched by age 30,44 or by age and race, 5,41,46 thus disregarding key differences between professional players and the general population. To better account for health and fitness, some NFL studies match on body mass index (BMI), 11,73 a measure that does not differentiate between fat and muscle mass. As a result, an active or former NFL player with a high BMI may be healthier than an age- and BMI-matched male control. A study of athletes competing at the NFL Combines found that obesity prevalence was overestimated when based solely on BMI and not body fat percentage. 65 Taken together, increased longevity studies in football players may reflect the inclusion of inappropriate comparison groups, potentially masking possible negative effects of professional football on mortality. 48
Other NFL studies have used education as an adjustment variable because it can serve as a proxy for socioeconomic status. 73 Independent of income, education has been shown to be protective against many diseases, including dementia. 21 However, this adjustment strategy may be inappropriate for a professional football population because most players attend college, thus reducing its predictive ability. In fact, while the college graduation rates among former NFL players are greater than 70% (compared with 30% for the general male population), former professional football players are twice as likely to report income below the poverty level than a general population of college graduates. 87
To address the HWE in football players, a recent study used replacement players recruited during an NFL players’ strike as a comparison group. 82 Replacement players likely had similar body composition and fitness to career professional players, yet they played 3 games or fewer of professional football. In contrast to results from previous studies, longevity of football players was not significantly greater than that of replacement players in this study. 82 Instead, data suggested that career professional football players were 38% more likely to have died during the course of the study compared with replacement players (results did not reach statistical significance). Players of other professional sports may serve as an even better comparison group. 33,52 When NFL players were compared with players in the National Basketball Association, National Hockey League, and Major League Baseball, age at death was relatively comparable across all sports, 47 despite methodological weaknesses related to adjustment factors. Other studies have compared contact sports versus noncontact sports to better isolate exposures in non-NFL cohorts. 50,51 These studies have shown neuroanatomic imaging parameter 51 and cognitive 50 differences between athletes in contact versus noncontact sports. Results from studies of this type may yield additional insight beyond those that use general population samples.
Volunteer and Nonresponse Bias in Study Participant Enrollment
Volunteer bias may shape study results when study volunteers have different characteristics from those who declined participation. Former and current football players experiencing health challenges that they attribute to football may be more likely to participate in a study, thus overrepresenting health conditions. If participation is simultaneously driven by the health of volunteers and level of exposure (eg, the exposed unhealthy volunteers preferentially participate), this can bias association statistics between exposures and outcomes. Along similar lines, nonresponse bias may occur when potential study participants do not enroll because they are too ill or impaired. For example, a study on nonresponse bias in an asbestos-cancer surveillance program found that nonrespondents were older than respondents, which could bias results if age was related to both the exposure and outcome of the study. 40 Importantly, though, if participation or nonresponse is only related to the exposure or only related to the outcome, then although overall prevalence would be biased, spurious associations between an exposure and outcome would not occur if no true association exists. 34
If volunteer or nonresponse biases occur in professional football studies, study samples from participants may not accurately represent the approximately 26,000 former NFL players. To address these types of selection biases, researchers can look at the distribution of characteristics in the study sample and compare those with data on the larger population. For example, the Pro Football Reference data set contains information on approximately 20,000 former players. 64 It has been previously established that injury is not evenly distributed by position. 6,9,10,42,60 Therefore, in any football study that considers the effects of injury, the distribution of playing position in the full population could be compared with the position distribution in the study sample. If there is concern that a study sample may be nonrepresentative, different statistical techniques can be considered to account for any over- or underrepresentation that has occurred; one such approach is inverse probability weighting (IPW). 89
Survivor Effects in Longitudinal Studies
Bias can also occur in football studies if participants’ willingness to remain in a longitudinal study depends on their health. In a phenomenon known as survivor bias, participants who are most impaired or ill are more likely to be lost to follow-up, resulting in a final study sample that has excluded the poorest faring members of the cohort. 89 Attrition bias refers to the loss of participants in studies that require more than 1 interview or assessment. If this differential loss of participants is jointly related to exposure and outcome (eg, the sicker, exposed participants drop out), it can affect final parameter estimates. Sensitivity analyses that explore characteristics of those who drop out compared with those who remain (eg, IPW analyses) for this study and others would provide investigators with a means of assessing and potentially compensating for attrition bias. 35,69
Subgroup Designation
As exposures even within a single occupational cohort tend not to be uniform, occupational epidemiologists identify subgroups likely to experience homogeneous exposure profiles. In football, position represents the most obvious subgroup and may serve as a proxy for a combination of other variables such as physical size, training regimen, potential injuries, and even race. Injury data show patterns by position for concussion, 9,61 joint injuries, 6,10,42 and mortality. 5,41 Nevertheless, some NFL studies combine positions into categories that may not align with injury data. For example, Baron et al 5 created 3 categories: category 1 included defensive backs, punters, kickers, quarterbacks, and wide receivers; category 2 included fullbacks, halfbacks, linebackers, running backs, and tight ends; and category 3 included only linemen. The effect of position on mortality was nonsignificant in their analyses after adjustment for BMI, age, race, and calendar year. However, given that much of the data on injury show that quarterbacks, wide receivers, and defensive secondaries receive the most injuries, it is possible that combining these high-injury positions with low-injury positions such as kickers diminished or obscured position effects.
A number of studies have separated linemen from other positions and found particular hazards for linemen in terms of sleep apnea, 27 cardiac disease, 16,33 and mortality. 5 Many NFL studies do not adjust for position 2,18,32,57,67 or they consider only linemen versus nonlinemen. 11,16,63,74 Given that the physique required for players is known to be associated with certain health risks and that positions themselves carry specific risks and hazards on the field, a more granular approach that examines data position-by-position may be more likely to yield nonbiased results. Studies with larger sample sizes or those restricted to specific positions may also be better able to capture position-specific effects of football.
Information Bias
Data on past play and practice injuries may not be accessible to professional players and researchers, either because data were not recorded or because they are considered proprietary. As a result, exposure and outcome data need to be reconstructed by players and their families in studies that attempt to link football exposure to health outcomes. However, relying on memory makes the study susceptible to recall bias. 12,15 If such exposure recall error is random with respect to the outcome under study, it is known as nondifferential recall bias. This type of error does not create a spurious association where a true causal effect does not exist, but it typically biases any true effect toward the null, increases the variance of risk estimates, and therefore increases the likelihood that real causal associations are not detected. 4 Recall can also be differential, such as when patients who are sick overreport exposures they believe are relevant to their illness. 58,72,85 For example, a study on parental occupational exposure and childhood leukemia showed overestimations of exposure by fathers of leukemia patients in the prenatal period. 71 Differential misclassification of exposure can also occur when the health outcome affects cognitive processing. Cognitive or memory impairment putatively caused by football could result in those participants’ misremembering and underreporting exposures, thus making an exposure appear less harmful and potentially protective when it is not. 15 As an example, a study on former NFL players looked specifically at the reliability of concussion self-report and found that only 62% of participants reported the same number of concussions at baseline and follow-up. 38 Those who reported new physical and mental health deficits at follow-up were more likely to report more concussions, suggesting that health issues may affect concussion recall.
Information bias can be assessed by comparing recalled evidence with additional sources such as video footage or interviews with family members. 28 Game footage that sampled small numbers of players across positions could be analyzed to quantify typical hits and force rates and then applied more broadly to all players by position in a PEM. In studies at risk for recall bias, investigators might choose to instead use easier to recall surrogate variables such as number of seasons or snaps as a more accurately assessed proxy for football exposures. Researchers can use self-administered questionnaires for sensitive questions, use a control group with a different disease to minimize differential recall bias, or use questionnaires with prompts that maximize accuracy. For example, Robbins et al 68 found that athletes were significantly more likely to report higher numbers of concussions after hearing a medical definition of concussion. When athletes’ conceptions of concussion are aligned with a medical definition, data are ostensibly more reliable. Recall bias is a known risk for retrospective cohorts in occupational epidemiology, especially for studies with long-term outcomes such as cardiovascular and neurodegenerative disease. 15 However, these considerations are rarely explored systematically in published football data, so their influence over these results is unknown.
Small-Study Bias
A number of the currently published studies on the health effects of football were conducted using small sample sizes. 3,8,57,75,78 These studies may be influenced by small-study effects, a term that refers to the tendency of smaller studies to report greater effect estimates than larger studies 77 and demonstrate poorer reproducibility. 7 As an example, Stamm et al 75 conducted a study on 21 former professional football players who had been exposed to tackle football before age 12 years, who were matched to 21 former professional players exposed after age 12 years. The investigators found that men who played earlier performed significantly worse on cognitive tests of memory and verbal IQ, and large significant effects were seen in executive function tasks. However, in such a small study, the effect size must be large to achieve significance because the confidence intervals will also be wide. Given that follow-up will be preferentially done on studies with promising results and considering the penchant not to publish results that are not significant (publication bias), there is a potential bias to reporting large effect sizes that may not be apparent in larger study samples. Publication bias may also be at play within the landscape of football and health literature, in that studies with nonsignificant effect sizes are not submitted or selected for publication. In cases when nonsignificant results are found in football health studies, post hoc power calculations could be used to ascertain the minimum sample size needed to see a reasonable effect while allowing for some margin of error. These statistics would allow researchers to determine whether small studies were sufficiently powered to detect the effect they intended to capture. There may be subtle yet important health effects that are not appearing in the published literature that are nevertheless relevant to NFL players, doctors, and coaches and could inform larger, better powered studies in the future.
Conclusion
Many published studies rely on the “ever-never” dichotomy for professional football players, making it difficult to ascertain what aspects of football are tied to a particular outcome or result from nonspecific football-related characteristics such as increased income or access to health care. Similarly, the healthy worker effect is likely relevant for these cohorts. New studies on long-term consequences in football players could make comparisons within players and incorporate more detailed football exposure metrics such as position information, as well as factors that are known to affect health such as childhood socioeconomic status. Additionally, using larger publicly or commercially available data sources would enable the evaluation of selection bias in NFL cohorts and provide objective exposure data. Such data could be used to identify the most effective strategies for elimination or mitigation of injuries and their sequelae in professional football players. In summary, using well-established methods developed for occupational cohorts to define and interrogate different football exposures will potentially improve researchers’ ability to tie play-related activities to health outcomes, with an eye toward reducing injury and illness in this highly specialized yet uniquely vulnerable population.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.Z. receives royalties from Oakstone and Demos Publishing; serves on the scientific advisory boards for Myomo, Oxeia Biopharma, ElMIndA, and Biodirection; and evaluates patients in the MGH Brain and Body-TRUST Program, which is funded by the National Football League Players Association (NFLPA). A.P.-L. was partly supported by the Sidney R. Baer Jr. Foundation, the National Institutes of Health (NIH) (grants R01MH100186, R21AG051846, R01MH111875, R01MH115949, R01MH117063, R24AG06142, and P01AG031720), the National Science Foundation, DARPA, the Football Players Health Study at Harvard University, and Harvard Catalyst - The Harvard Clinical and Translational Science Center (NCRR and the NCATS NIH, UL1 RR025758); serves on the scientific advisory boards for Neosync, Neuronix, Starlab Neuroscience, Neuroelectrics, Magstim, Constant Therapy, and Cognito; and is listed as an inventor on several issued and pending patents on the real-time integration of transcranial magnetic stimulation with electroencephalography and magnetic resonance imaging. A.B. has received funding from the NIH/National Heart, Lung, and Blood Institute, NFLPA, American Heart Association, and American Society of Echocardiography and receives compensation for his role as team cardiologist for US Soccer, US Rowing, the New England Patriots, the Boston Bruins, the New England Revolution, and Harvard University. All of the other authors named in this study are either partially or fully supported by the Football Players Health Study at Harvard University, which is sponsored by the NFLPA. The NFLPA had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Acknowledgment
The authors acknowledge the study participants, advisors, and staff of the Football Players Health Study. They are also grateful to Dr Frank Speizer for his helpful feedback on the manuscript and Jeffrey Adams for his football expertise.