
Abstract
Background:
Tibial plateau fractures can be devastating traumatic injuries to the knee, particularly in active athletes.
Purpose/Hypothesis:
The purpose of this study was to report on the return to participation in recreational athletics after operatively managed tibial plateau fractures. In addition, this study assessed factors associated with the ability to return to participation in recreational athletics after tibial plateau fractures treated with open reduction internal fixation and compared final outcomes between patients who were able to return to recreational athletics and those who could not. The hypothesis was that returning to participation in recreational athletics would be dependent on the time from surgery after operative fixation of tibial plateau fractures. Less severe injuries would be associated with a quicker return to athletics.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
All tibial plateau fractures treated by 1 of 3 surgeons at a single academic institution over an 11-year period were prospectively followed. Final outcomes were evaluated using the Short Musculoskeletal Function Assessment at latest follow-up. All complications were recorded at each follow-up. Differences between the groups were compared using Student t tests for continuous variables. Chi-square analysis was used to determine whether differences between categorical variables existed. Logistic regression was performed to assess independent variables associated with returning to participation in recreational athletics.
Results:
A total of 169 patients who underwent operative management of their tibial plateau fracture reported participation in recreational athletics before their injury. By the 6-month time point, 48 patients (31.6%) had returned to participation in recreational athletics, and at final follow-up (mean, 15 months), 89 patients (52.4%) had returned to participation in recreational athletics. Predictors of returning to recreational athletics included white race, female sex, social alcohol consumption, younger age, increased range of motion (ROM), low-energy Schatzker patterns (I-III), injuries not inclusive of orthopaedic polytrauma or open fractures, and no postoperative complications. White race, social alcohol consumption, and increased ROM were associated with returning to athletics at both 6-month and final follow-up. Lack of a venous thromboembolism was associated with returning to athletics at final follow-up. Patients who returned to recreational athletics had associations with better functional outcomes and emotional status than those who did not.
Conclusion:
The number of patients who returned to participation in recreational athletics gradually increased over time after operative fixation of tibial plateau fractures. Less severe injuries and a lack of postoperative complications were associated with a quicker return to athletics. Predictors of returning to participation in recreational athletics after operatively managed tibial plateau fractures can be used to target patients at risk of not returning to play to provide interventions aimed at improving their recovery, such as early knee range of motion, muscle strengthening, and participation in low-impact activities.
Keywords
Tibial plateau fractures are orthopaedic injuries that occur in a bimodal age distribution. These injuries are commonly seen in younger to middle-aged males (high-energy trauma) and elderly females (falls). 5,7 The operative management of tibial plateau fractures is performed to reconstruct the articular surfaces of the tibia, provide stable fragment fixation, and repair associated injuries of the knee when possible. 29,31 Decreased knee stability and the failure to restore joint alignment are the most significant predictors of poor final outcomes. 18,23,27 While much is known about outcomes after tibial plateau fractures, a diminutive amount of literature exists with regard to recreational and athletic activities subsequent to this injury. However, returning to recreational athletics after orthopaedic trauma is an important topic. Tibial plateau fractures often occur in young and active patients and may precipitate disability or a decrease in overall function. 17 Although not always possible, patients desire a return to preinjury activity, as recreational athletics has been demonstrated to contribute to a person’s overall physical health and well-being. 2,9,11,13,15,17,20
There has been an increase in life expectancy over the past several decades. 20 Through advancements in medicine and surgery, patients have the ability to remain active with increasing age. The recent literature has demonstrated the importance of physical activity in adolescents, adults, and the elderly. 11,15,17 When possible, returning to physical activity after orthopaedic trauma improves the patient’s physical and emotional health.
Returning to participation in recreational athletics after orthopaedic injuries has been associated with improved satisfaction after anterior cruciate ligament tears. 4 Few studies have discussed the return to participation in recreational athletics after tibial plateau fractures. 13,17,23,28 Only 1 study reported participation in recreational athletics at numerous time points after tibial plateau fractures. 17 The purpose of this study was 3-fold: (1) to present the largest study to date to report on the return to athletic participation after tibial plateau fractures managed with open reduction internal fixation (ORIF); (2) to determine which patient demographics, injury characteristics, surgical techniques, or postoperative complications are associated with the return to athletic participation after operatively managed tibial plateau fractures; and (3) to assess if differences exist regarding physical (functional) and psychological (emotional) outcomes in patients who were able to return to recreational athletics after operatively managed tibial plateau fractures compared with those who were not.
Methods
Over an 11-year period, from April 2006 to March 2016, all tibial plateau fractures treated by 1 of 3 surgeons at a single academic institution were prospectively followed from an institutional review board–approved database. Patients were screened and identified on presentation to the emergency department or the clinical office for inclusion in the registry. After attaining history and physical examination findings, standard radiographs of the knee, including anteroposterior, lateral, and 10° caudal tilt plateau views, were obtained for all patients (Figure 1). A computed tomography scan was obtained to further elucidate the fracture morphology and allow for the planning of surgical interventions in all cases (Figure 2). The fracture classification was based on the systems of Schatzker et al 27 and Moore et al. 22 Classifying was performed by the treating surgeon and confirmed by another fellowship-trained orthopaedic trauma surgeon.

A 34-year-old female patient sustained a severe tibial plateau fracture-dislocation of the knee after a fall while running. Initial injury radiographs, which included (left to right) anteroposterior, lateral, and 10° caudal tilt plateau views of the knee.

Computed tomography scan demonstrating articular involvement in the same patient, axial views (top row) and sagittal/coronal views (bottom row).
Inclusion criteria for this study were the following: operatively managed tibial plateau fractures that were a minimum of 12 months after surgery, age ≥18 years, at least 1 year of postoperative follow-up data, and patient participation in recreational athletics before sustaining the tibial plateau fracture.
Patient-related factors and demographics (age, sex, race, body mass index [BMI], tobacco use, alcohol use, drug use), injury characteristics (open fracture, compartment syndrome, neurovascular injury, orthopaedic polytrauma, Schatzker classification, Moore classification), and surgical techniques (application of external fixator, locked or unlocked plating, single or dual plating, number of incisions, soft tissue repair, anesthesia type) were recorded. Radiographic malreduction was documented at 6-month and final follow-up as a malalignment of ≥5°. A preinjury functional assessment, including questions about athletic participation before the injury, was conducted using the validated Short Musculoskeletal Function Assessment (SMFA). The Short Form–36 (SF-36) questionnaire with regard to “return to athletics” was utilized. Fractures were further divided into low-energy (Schatzker I-III) and high-energy (Schatzker IV-VI) patterns. Additionally, fractures were divided into 2 groups based on the Moore classification: fracture-dislocation (types I-V) and no fracture-dislocation.
Surgical Indications, Operative Fixation, and Postoperative Management
Patients were indicated for surgical management based on several accepted parameters: articular malalignment assessed through coronal and sagittal radiographic imaging (at least 2-mm articular incongruence and/or condylar widening >5 mm), presence of an open fracture, varus/valgus instability >5° on physical examination, absence of significant pre-existing arthritis of the knee, and the patient’s medical stability to undergo surgery. The principles of definitive ORIF fixation included the restoration of articular congruity and the provision of proper mechanical alignment. This was achieved through balanced fixation utilizing appropriate implants (Figure 3).
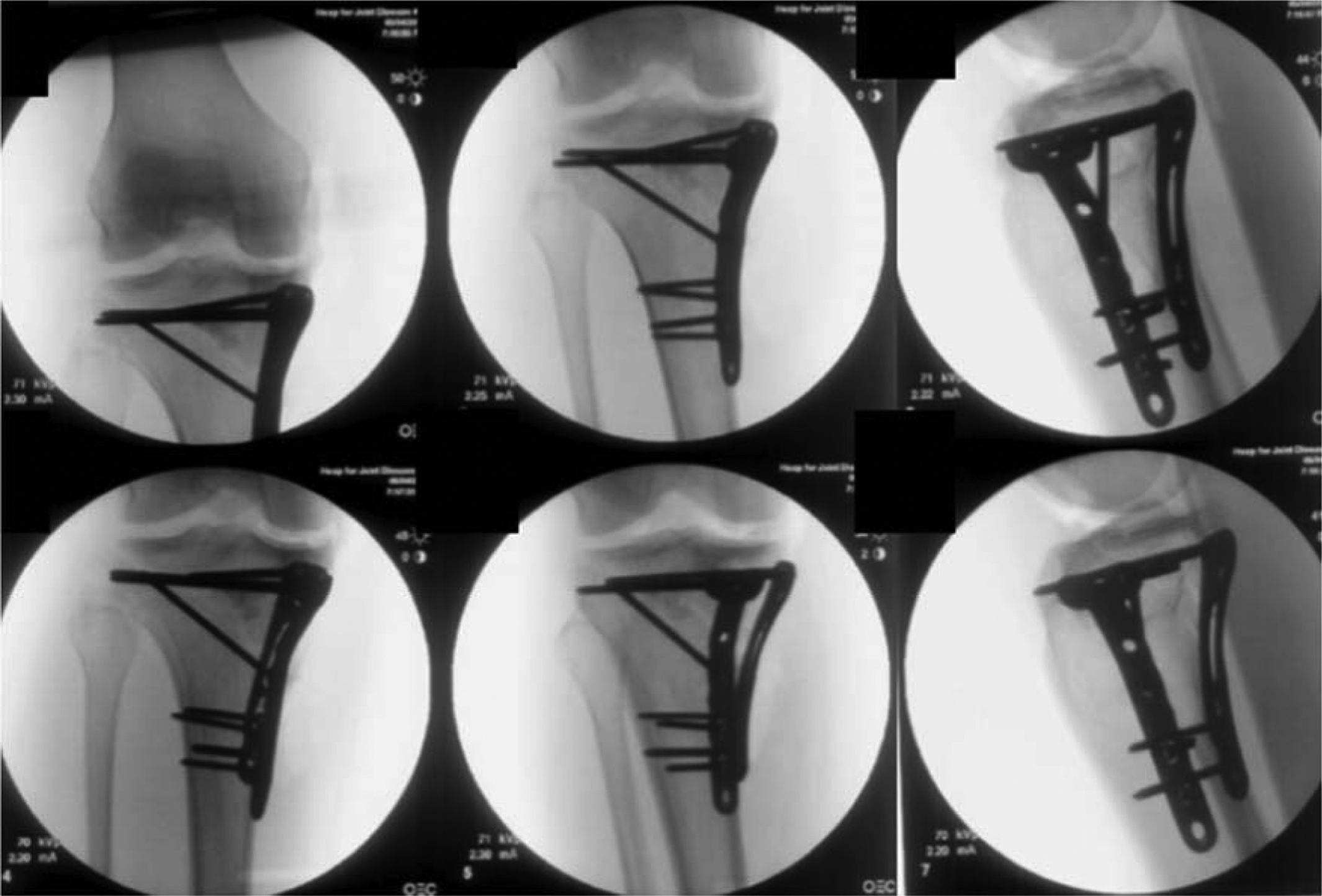
Postoperative images after open reduction internal fixation in the same patient.
Interventions generally followed a period of waiting to operate until the soft tissue envelope was ready, using percutaneous and minimally invasive techniques when appropriate. 35 Our standard protocol for high-energy tibial plateau fractures was based on a staged management protocol, which utilized knee-spanning external fixation followed by definitive repair when the soft tissue allowed. 6
Thromboprophylaxis was administered in the form of low–molecular weight heparin (LMWH) beginning 12 hours postoperatively and prescribed for a minimum of 4 weeks, unless contradicted. If the patient required a subsequent procedure, LMWH was discontinued at least 12 hours before surgery. Upon discharge, all patients were provided thromboprophylaxis in the form of LMWH or aspirin 1 time daily, depending on physician and patient choice. Patients with closed injuries received intravenous antibiotics for 24 hours after each surgical procedure. Those who sustained an open fracture received 48 hours of antibiotics (cephalosporin and aminoglycoside), followed by 24 hours of antibiotics after each operative procedure. Patients who developed a deep wound infection were given a 6-week course of intravenous antibiotics.
Patients’ knees were generally kept immobilized for 3 to 7 days postoperatively. The knees were initially placed in extension and then transitioned to an unlocked hinged knee brace. Patients began physical therapy for knee range of motion (ROM) exercises along with quadriceps and hamstring strengthening. Patients remained nonweightbearing until they had achieved radiographic and clinical signs of union, which typically occurred at 10 to 12 weeks after operative fixation. When union was achieved and weightbearing was allowed, patients continued physical therapy with a weightbearing-as-tolerated approach. When complete fracture healing was confirmed, patients were allowed to participate in recreational activity and were given the following recommendations: (1) to perform activities that do not elicit pain and (2) to begin with minimal- to low-impact recreational athletics, such as spinning machines and water aerobics. Postoperative complications and reoperations (deep infection requiring incision and drainage, superficial infection requiring oral antibiotics, early implant failure requiring revision fixation, nonunion requiring nonunion repair with grafting, venous thromboembolism requiring anticoagulation, painful implant requiring implant removal, and knee arthrofibrosis requiring lysis of adhesions) were documented at follow-up and recorded contemporaneously at each postoperative visit. Clinical outcomes were assessed using the validated SMFA at 3-month, 6-month, and final (≥12-month) follow-up.
Statistical Analysis
Patients were divided into 2 groups based on their own description of their participation in recreational athletics on the SF-36 questionnaire (vigorous activities such as running and heavy lifting and participation in strenuous sports) at short-term (6-month) and final follow-up: group 1 comprised those who initially participated in sport and were able to return to recreational athletics after operatively managed tibial plateau fractures, and group 2 comprised those who initially participated in sport and were unable to return to recreational athletics after operatively managed tibial plateau fractures. Patients were considered to have returned to recreational athletics if they participated at any level of recreation, whether limited or full. Final outcomes were evaluated using ROM and the SMFA at latest follow-up. Statistics were calculated using SPSS version 23 (IBM). For all analyses, significance was set at P < .05. Student t tests were used to assess differences between continuous variables, and Pearson chi-square analysis was used to assess differences in categorical variables. Logistic regression was performed, with the dependent variable being return to participation in athletics, while the independent variables consisted of demographics, initial injury characteristics, and postoperative complications.
Results
Overall, 321 patients were treated over the 11-year study period. Thirty-nine of these patients were treated with nonoperative management, and 7 patients were lost to follow-up. Two hundred seventy-five patients were at least 12 months from operative management and eligible for review, and 245 patients had 12-month follow-up data available. Of these, 76 patients did not participate in recreational athletics before their injury; 169 patients had final follow-up data recorded and participated in recreational athletics before their tibial plateau fracture and were therefore included in our analysis.
Demographics and initial injury characteristics of the study patients are shown in Table 1. The detailed mechanisms of sustaining a tibial plateau fracture in this cohort are demonstrated in Figure 4.
Demographics and Initial Injury Characteristics a

a Data are presented as % unless otherwise specified.
b Types I-III indicate low-energy injury, and types IV-VI indicate high-energy injury.

The percentage of tibial plateau fractures sustained by a specific mechanism. Percentages are based on the patients who participated in recreational athletics before their operatively managed tibial plateau fracture. Only 11% of tibial plateau fractures occurred from a sporting injury.
Factors Associated With Athletic Participation After Operatively Managed Tibial Plateau Fractures
By 6 months postoperatively, 31.6% of the patients returned to participation in recreational athletics. Factors associated with an early return (6 months) were white race (P < .001), social alcohol consumption (P = .016), and increased ROM (P < .001). Increasing age was not associated with a decreased return to recreational athletics (P = .267).
Patients were less likely to return to recreational athletics by 6 months if their tibial plateau fracture was a high-energy Schatzker pattern (IV-VI) (P = .025), if their fracture was accompanied by additional orthopaedic injuries (P = .010), and if postoperative complications such as a deep infection (P = .048) occurred (Table 2). Surgical techniques were not associated with the return to athletics.
Significant Predictors and Trends of Returning to Participation in Recreational Athletics at Short-Term Follow-up (6 Months) a

a A total of 17 patients did not provide their participation in recreational athletics at the 6-month time point. Data are presented as % unless otherwise specified.
b Statistical significance at P < .05.
Logistic regression demonstrated white race to be the only independent predictor of returning to participation in recreational athletics at 6-month follow-up (odds ratio [OR], 3.026 [95% CI, 1.254-7.350]; P = .014). Not sustaining orthopaedic polytrauma was a trend associated with returning to participation in athletics at 6-month follow-up (OR, 0.390 [95% CI, 0.141-1.084]; P = .071).
At final follow-up (mean, 15 months [range, 12-78 months]), 52.6% of patients had returned to participation in athletic activities. At final follow-up, white race (P < .001), social alcohol consumption (P = .029), increased ROM (P = .013), and younger age (P = .014) were associated with a return to participation in athletics.
Patients were less likely to return to recreational athletics at final follow-up if they developed a postoperative complication of a deep infection (P = .020) (Table 3).
Significant Predictors and Trends of Returning to Participation in Recreational Athletics at Final Follow-up (Mean, 15 Months) a
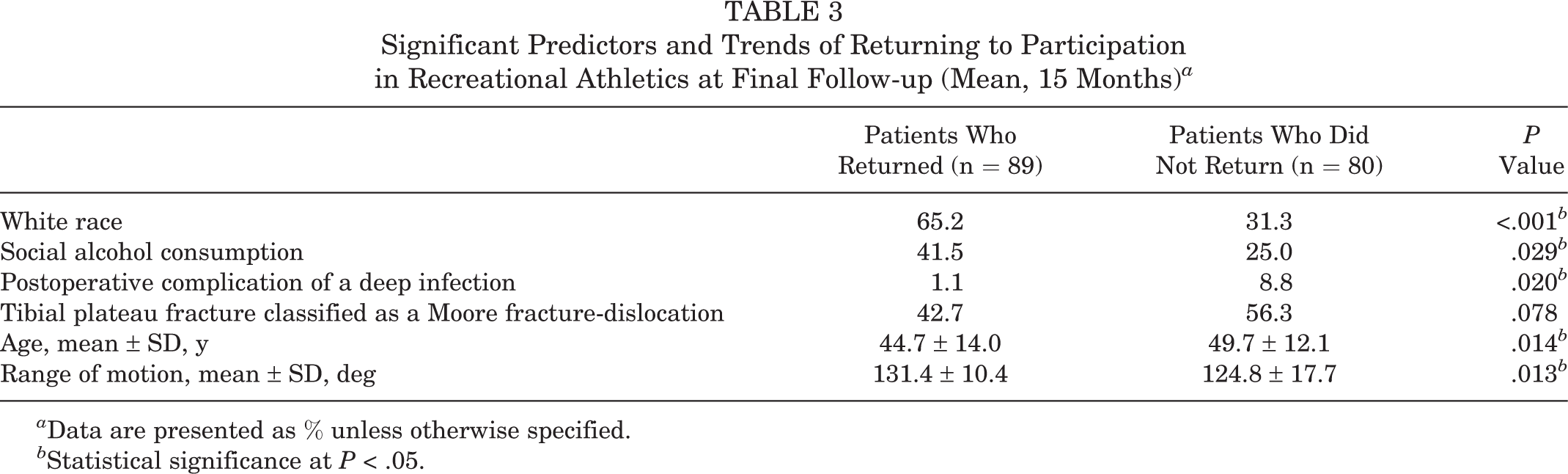
a Data are presented as % unless otherwise specified.
b Statistical significance at P < .05.
Logistic regression demonstrated the following variables to be independent predictors of returning to participation in recreational athletics at final follow-up: white race (OR, 8.445 [95% CI, 3.400-20.977]; P < .001) and not sustaining a venous thromboembolism (OR, 0.024 [95% CI, 0.003-0.660]; P = .045).
Final Functional Outcomes
Final functional outcomes and emotional status (mean, 15 months [range, 12-78 months]), as measured by the SMFA, were worse for patients who did not return to participation in recreational athletics (P < .001). Patients who did not return to participation in recreational athletics had a mean SMFA score of 28.36 ± 19.37, while patients who returned to participation in recreational athletics had a mean SMFA score of 8.84 ± 10.17.
Discussion
Tibial plateau fractures may lead to disability and hinder patients’ participation in recreational athletics. They are one of the more challenging intra-articular fractures to treat. ORIF is a standard of care for tibial plateau fractures that meet displacement criteria, have an associated vascular injury requiring repair, are considered an open fracture, or have an associated compartment syndrome. 18,23,27,31 In the past decade, multiple studies have looked at functional results after operatively managed tibial plateau fractures, showing a favorable prognosis at final follow-up. 14,26,27,30 While many studies have focused on radiological findings and outcomes years after surgery, Urruela et al 32 found that good clinical and functional results are demonstrated in operatively managed tibial plateau fractures that achieve appropriate articular reduction at 12-month follow-up. Patient-reported outcomes at 1 year after operatively managed tibial plateau fractures provided a good prognosis for knee function in the future. 26 Rademakers et al 26 found monocondylar fractures to have significantly better functional results than bicondylar fractures. Additionally, they found osteoarthritis to be more prevalent in patients with a postoperative knee malalignment of >5°. 26 Failure of restoring joint alignment and decreased knee stability are significant contributors to substandard results after the operative repair of a tibial plateau fracture. 18,23,25,27,29 Indeed, good surgical outcomes are needed for patients to have the ability to return to previous activities, such as participation in recreational athletics.
We found that the number of patients who returned to participation in recreational athletics gradually increased over time after ORIF for a tibial plateau fracture. At the 6-month time point after operative management, only one-third of patients had returned to participation in recreational athletics. By final follow-up, over half of patients in this study had returned to participation in athletics. At a longer follow-up, more patients, especially those who sustained polytrauma, may be able to return to athletics.
In a study performed by Kraus et al, 17 nearly two-thirds of patients with operatively managed tibial plateau fractures returned to participation in recreational athletics at 1-year follow-up, while 88% of the patients participated in recreational athletics at a mean of 4.4 years of follow-up. However, significant differences exist between this study and ours, which may account for the discrepancies in athletic participation at final follow-up. The study performed by Kraus et al 17 likely represented a different patient population, as they had a broad set of exclusion criteria, which included severe injury characteristics and patient comorbidities, which our study did not exclude. In addition, that study used different surgical techniques, as 71% were treated with ORIF, 23% were arthroscopically assisted, and 6% were minimally displaced and treated with percutaneous screws. Patient characteristics and the mechanism of sustaining a tibial plateau fracture also differed, with more than half of the tibial plateau fractures being caused by sporting injuries, while this mechanism of injury accounted for only 11% of the fractures in our cohort. More than 10% of the patients in the aforementioned study were competitive or professional athletes.
Previous studies have reported changes in patients’ athletic participation, from high-impact sports, such as skiing and jogging, before their knee injury to lower impact sports, such as Nordic walking, aqua fitness, weight training, and cycling, after the injury. 17,20 Yet, multiple patients in the discussed studies continued to participate in high-impact sports after operatively managed tibial plateau fractures, which was noted in our cohort as well. All patients should be counseled on the current literature and information presented in this study, which demonstrates a decrease in athletic participation after tibial plateau fractures.
Our study demonstrates that patients who were able to return to recreational athletics had associations with better functional outcomes, both physically and emotionally. Participation in recreational athletics is an important aspect of life among all ages, especially in an environment in which the life span of people is increasing. 20 The benefits of physical activity and participation in sports have been well established. 2,12 A majority of the leading causes of death in the United States are chronic diseases, such as heart disease, cancer, stroke, pulmonary disease, and hazardous drinking. 3,16,21 Physical inactivity is a major contributor to these diseases and a modifiable risk factor. 16 The American College of Sports Medicine and the American Heart Association recommend physical activity for a minimum of 30 minutes, 5 days a week, or intense aerobic activity for a minimum of 20 minutes, 3 days each week.
In addition to the benefits that physical activity has on overall health, participation in recreational athletics contributes to a healthier emotional state. 8 The study patients who were able to return to participation in recreational athletics had a better emotional status (from the validated SMFA’s emotional status category, which includes items based on an individual patient’s overall well-being) in comparison with patients who did not return to recreational athletics.
This study is the first to our knowledge to provide a report on factors associated with a return to participation in recreational athletics after operatively managed tibial plateau fractures. Severe tibial plateau fractures have been associated with increased complication rates and worse outcomes compared with low-energy tibial plateau fractures. 22,23,26,27 We therefore recommend orthopaedic trauma surgeons carefully follow patients who have sustained high-energy injuries, open fractures, and postoperative complications. It is crucial for these patients to be made aware of the prognosis of their injuries. Having the ability to predict factors that influence a patient’s ability to participate in recreational athletics after unexpected injuries is crucial to aiding patients in their injury prognosis and to providing early interventions in at-risk groups.
Ethnicity played a factor in returning to recreational athletics. At both short-term and final follow-up, white patients were more likely to have returned to recreational activities. Minorities have been reported to have worse outcomes than white patients after orthopaedic trauma. 24,34 Penrod et al 24 found that white patients had decreased mortality and increased mobility after hip fractures. After distal radius fractures, Walsh et al 34 found that black and Latino patients had increased pain and a suboptimal functional status compared with white patients. The literature suggests that people with a lower socioeconomic status have decreased access to medical care, which may contribute to suboptimal outcomes after fractures and orthopaedic procedures. 1,24,34 We recommend that patients of lower socioeconomic status be closely followed and physicians be aware of the socioeconomic disparities that may affect these patients’ care and return to recreational athletics.
Postoperative interventions may include early ROM exercises, such as continuous passive motion (CPM). Knee stiffness can hinder a patient’s participation in recreation, as knee ROM of 125° is necessary for adequate function. 19 Wall and Board 33 demonstrated that the differentiation of mesenchymal tissue to hyaline articular cartilage was more rapid and complete with immediate CPM in rabbits. Haller et al 10 utilized CPM after tibial plateau fractures and demonstrated a decreased risk of developing arthrofibrosis.
This study has limitations. With regard to participation in recreational athletics, patients were not queried about the specific sports that they participated in. Furthermore, there was no preinjury or postinjury information recorded with regard to the intensity of athletics and time spent participating in athletics. Future studies may consider utilizing the Tegner score for surveying patients. Next, the mean follow-up was 15 months. A longer follow-up is needed to assess the development of osteoarthritis after these traumatic injuries, as this may lead to decreased participation in athletics over time. It is also possible that although many patients did return to participation in recreational athletics, it was at a lower level than previously attained. All ORIF procedures were performed by 1 of 3 fellowship-trained orthopaedic trauma surgeons, and results may not be reproducible by general orthopaedic surgeons.
Conclusion
Patients who sustain a tibial plateau fracture and are undergoing operative interventions should be counseled that they have a 50% chance of returning to participation in recreational athletics by 1 year after the injury. White race, social alcohol use, younger age, increased knee ROM, low-energy Schatzker fractures, and absence of postoperative complications were predictive for patients being able to return to recreational athletics after operatively managed tibial plateau fractures. White race was an independent predictor of returning to athletics at both 6-month and final follow-up. Not sustaining a venous thromboembolism was an independent predictor of returning to athletics at final follow-up. The patients who were able to return to recreational athletics had better functional and emotional outcomes at final follow-up. This information can be used to target patients at risk of not returning to play by providing early interventions aimed at improving their recovery.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: K.A.E. is a consultant for Exactech; receives royalties from Exactech, Slack, and Lippincott; and receives grant support from the Orthopaedic Research and Education Foundation.
Ethical approval for this study was obtained from the New York University School of Medicine’s Office of Science and Research Institutional Review Board (study No. i06-581).