
Abstract
Background:
Tibial plateau fractures in skiers are devastating injuries with increasing incidence. Few studies have evaluated patient-reported outcomes and return to skiing after operative fixation of a tibial plateau fracture.
Purpose:
To (1) identify demographic factors, fracture characteristics, and patient-reported outcome measures that are associated with return to skiing and (2) characterize changes in skiing performance after operative fixation of a tibial plateau fracture.
Study Design:
Case series; Level of evidence, 4.
Methods:
We reviewed all operative tibial plateau fractures performed between 2016 and 2021 at a single level-1 trauma center. Patients with a minimum of 10-month follow-up data were included. Patients who self-identified as skiers or were injured skiing were divided into those who returned to skiing and those who did not postoperatively. Patients were contacted to complete the Patient-Reported Outcomes Measurement Information System–Physical Function domain (PROMIS-PF), the Knee injury and Osteoarthritis Outcome Score–Activities of Living (KOOS-ADL), and a custom return-to-skiing questionnaire. Multivariate logistic regression was performed with sex, injury while skiing, PROMIS-PF, and KOOS-ADL as covariates to evaluate factors predictive of return to skiing.
Results:
A total of 90 skiers with a mean follow-up of 3.4 ± 1.5 years were included in the analysis. The rate of return to skiing was 45.6% (n = 41). The return cohort was significantly more likely to be men (66% vs 41%; P = .018) and injured while skiing (63% vs 39%; P = .020). In the return cohort, 51.2% returned to skiing 12 months postoperatively. The percentage of patients who self-reported skiing on expert terrain dropped by half from pre- to postinjury (61% vs 29.3%, respectively). Only 78% of return skiers had regained comfort with skiing at the final follow-up. Most patients (65%) felt the hardest aspect of returning to skiing was psychological. In the multivariate regression, the male sex and KOOS-ADL independently predicted return to skiing (P = .006 and P = .028, respectively).
Conclusion:
Fewer than half of skiers who underwent operative fixation of a tibial plateau fracture could return to skiing at a mean 3-year follow-up. The knee-specific KOOS-ADL outperformed the global PROMIS-PF in predicting a return to skiing.
Tibial plateau fractures are common injuries that have increased in incidence over time. 3 In young, athletic patients, these fractures can be devastating sport-ending injuries, as they can be associated with significant osteochondral trauma, meniscal damage, ligamentous knee injury, symptomatic hardware, and the development of posttraumatic osteoarthritis in the long term.
Previous literature evaluating functional outcomes and return to sports after operatively treated tibial plateau fractures demonstrated rates of return to an active lifestyle between 53% and 88% at 1 year postoperatively.7,12,13,16,17,19 Several factors that have been shown to predict a return to recreational activity after operative treatment for tibial plateau fracture include White race, young age, social alcohol consumption, and increased range of motion. 13 Patients who return to recreational activity have been noted to have better functional and emotional status postoperatively based on the Short Musculoskeletal Function Assessment. 13
Downhill skiing is a common sports-related cause of tibial plateau fractures.16,17 After undergoing operative treatment of a tibial plateau fracture, it may be more challenging to return to skiing rather than other desired recreational activities, given the significant forces across the joint required for skiing. Several previous studies have specifically investigated return to skiing after tibial plateau fracture, demonstrating rates7,9,16,17 of return between 53% and 87%. However, previous literature on this subject is limited by small sample sizes and needs ski-specific, patient-reported outcome data.3,12,16 There is minimal existing research correlating commonly used patient-reported outcome measures (PROMs) with return to skiing and changes to skiing ability after operative fixation of a tibial plateau fracture.
This study aimed to (1) identify demographic factors, fracture characteristics, and PROMs that are associated with return to skiing and (2) characterize changes in skiing performance after operative fixation of a tibial plateau fracture. We hypothesized that final postoperative PROM scores would predict a return to skiing.
Methods
Patient Selection
Institutional review board approval was obtained before study initiation, and all included patients provided written informed consent. All patients who sustained a tibial plateau fracture and were evaluated at a level-1 trauma center between January 1, 2016, and January 7, 2021, were identified using Current Procedural Terminology (CPT) codes. CPT codes 27535 and 27536 included all displaced intra-articular unicondylar and bicondylar tibial plateau fractures requiring open reduction and internal fixation. A retrospective review of electronic medical records was then performed. Demographic information and postoperative outcomes were recorded. Polytrauma was defined as additional organ system or extremity injuries other than a unilateral tibial plateau fracture. Ligamentous knee injuries were identified by either intraoperative findings or postoperative knee physical examination under anesthesia and confirmed with magnetic resonance imaging. The radiographic review included grouping patients according to unicondylar fractures (medial or lateral column involvement; Schatzker types I-IV) and bicondylar fractures (medial and lateral column involvement; Schatzker types V and VI). 22 The exclusion criteria were as follows: inaccurate CPT code; incomplete medical record; bilateral plateau fractures; ipsilateral lower extremity compartment syndrome; and follow-up <10 months. A minimum 10-month follow-up was utilized to capture patients who completed surveys before their 1-year postoperative visit.
Surgical Technique
All patients were treated by 4 fellowship-trained orthopaedic trauma surgeons (D.R., T.H, L.M., J.H.) at our institution. Preoperative prophylactic antibiotics were administered before the surgical incision. The choice of patient positioning and surgical approach was dictated by a preoperative review of patient radiographs and computed tomography imaging. The distribution of surgical approaches was as follows: isolated anterolateral—103 (49.8%); isolated posteromedial —19 (9.2%); anterolateral and posteromedial—70 (33.8%); posterior— 10 (4.8%); and other—5 (2.4%). For anterolateral exposures, the use of a femoral distractor and direct evaluation of articular reduction and the lateral meniscus via a submeniscal arthrotomy was routine. All fractures were fixed with plate and screw constructs, although the location and desired function of plates was based on the fracture pattern. Cancellous allograft or calcium phosphate void filler was used at the treating surgeon's discretion to fill metaphyseal bone defects. Intrawound vancomycin powder was routinely placed in deep surgical incisions before closure.
Standard postoperative care consisted of immediate active and passive knee range of motion as tolerated. Patients remained nonweightbearing for a minimum of 10 weeks in most cases. Typically, return to impact-loading activities was gradually resumed at a minimum of 16 weeks postoperatively.
Outcomes Evaluation
Patients who met the study inclusion criteria were contacted via telephone or email to complete 3 electronic questionnaires: the Patient-Reported Measurement Information System–Physical Function (PROMIS-PF); the Knee injury and Osteoarthritis Outcome Score–Activities of Living (KOOS-ADL); and a custom return-to-skiing questionnaire. Patients completed surveys electronically via Research Electronic Data Capture (REDCap) or were entered by research coordinators over the phone. 8
Patient-Reported Outcome Measures
The PROMIS was created by the US National Institutes of Health to develop standardized outcome measurements applicable to clinical practice, research, and quality assurance. The PROMIS has an item bank for each domain, which includes PF, Fatigue, Pain, Emotional Distress, and Social Role Participation. 6 In the PROMIS-PF computerized adaptive test, the participant's response to each question guides subsequent items proposed to them out of a 165-item bank. Each question proposes a function task, and the patient scores themselves on a scale of ability from 0 (unable to perform the task) to 5 (perform without any difficulty) or limitations from 0 (cannot do) to 5 (not at all limited). A minimum of 4 items must be answered to receive a score.
The KOOS is a knee-specific questionnaire designed to assess symptoms and function in patients with knee injuries or osteoarthritis. Five subscales are evaluated: Pain, Symptoms, ADL, Function in Sport and Recreation, and Knee-Related Quality of Life (QOL). Subscales are scored from 0 (extreme problems) to 100 (no problems). 21
Return-to-Skiing Questionnaire
A custom questionnaire was created to evaluate whether patients returned to skiing and at what time point they returned to skiing after injury as well as their functional and psychological limitations involved in returning to skiing. This questionnaire comprised 15 multiple choice questions and 2 open-ended questions (AppendixTable A1). Skiers were defined as those who skied before injury based on their survey response or those who had sustained injury while skiing based on a review of the electronic medical record.
Statistical Analysis
The included patients were divided into skiers and those who were not. The skier cohort was then divided into those who had returned to skiing and those who had not. Patient characteristics were summarized descriptively and compared between groups. Continuous variables were summarized as means and standard deviations and compared using the Mann-Whitney U or independent t tests where appropriate. Categorical variables were summarized as frequency (%) and compared using the chi-square or Fisher exact test. Normality for all statistics was assessed using the Shapiro-Wilk test. We also performed multivariate logistic regression analysis—with male sex, injury while skiing, PROMIS-PF, and KOOS-ADL included as covariates—to evaluate variables predictive of return to skiing. Statistical significance was defined as P < .05.
Results
A total of 341 patients were initially identified via the CPT code. After a chart review to exclude inaccurate or repeat CPT coding (n = 21), incomplete medical record data (n = 6), bilateral tibial plateau fractures (n = 3), and concomitant compartment syndrome (n = 6), 305 patients met the initial study inclusion criteria. An additional 98 patients (32.3%) were excluded for lack of a minimum PROM follow-up of 10 months. Thus, 207 patients with tibial plateau fractures with a minimum 10-month follow-up were included in the initial analysis and contacted to complete the questionnaires (response rate, 67.9%). Of these patients, 47.4% were skiers and 52.6% nonskiers. Eight skiers failed to respond to the survey and were excluded from the return-to-skiing analysis (Figure 1).
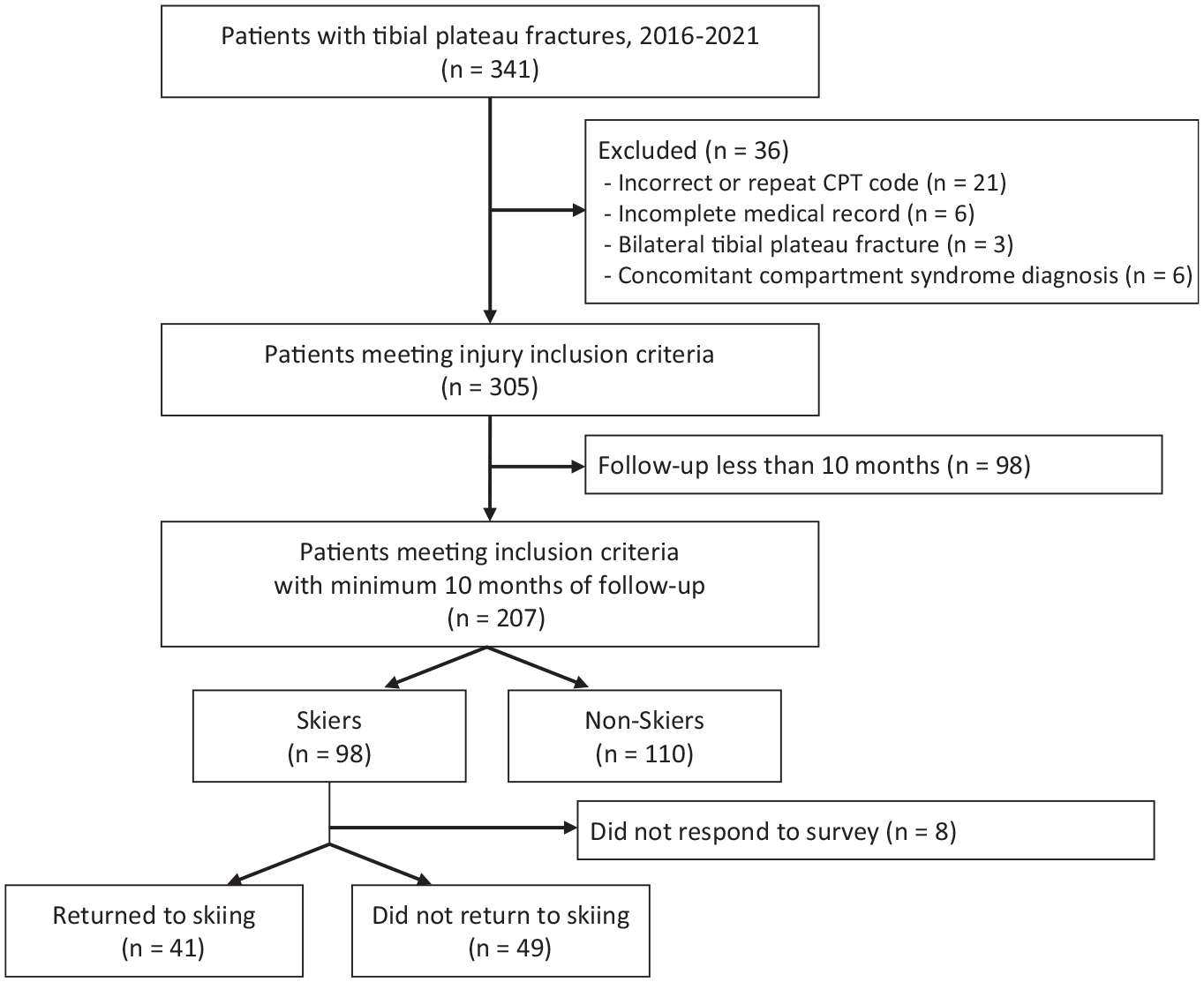
Consort flowchart of patient enrollment in the study. CPT, Current Procedural Terminology.
Skiers Versus Nonskiers
When comparing skiers and nonskiers, age, sex distribution, and the Charleston Comorbidity Index (CCI) were similar between groups (Table 1). However, skiers had a significantly lower body mass index (BMI) and were less likely to be polytraumas than nonskiers (P < .001 and P = .001, respectively). Follow-ups were significantly longer in skiers at 3.2 years compared with 2.5 years in nonskiers (P = .001). Finally, skiers had significantly higher final postoperative PROM scores compared with nonskiers (P≤ .036 for all), except the KOOS-QOL (Table 1).
Skiers Versus Nonskiers: Demographic and Postoperative Data a

Data are presented as mean ± SD or percentage unless otherwise indicated. ADL, Activities of Daily Living; BMI, body mass index; CCI, Charleston Comorbidity Index; KOOS, Knee injury and Osteoarthritis Outcome Score; PROM, patient-reported outcome measure; PROMIS-PF, Patient-Reported Measurement Information System–Physical Function domain; QOL, Quality of Life; Sport, Function in Sport and Recreation.
Return to Skiing
Of the 90 skiers included in the final return-to-skiing analysis, the return-to-skiing rate was 45.6% (n = 41). Also, 50% of skiers were injured while skiing. The return-to-skiing rate for patients injured while skiing was 57.7%. Age, BMI, and the CCI were similar between skiers who returned to skiing versus those who did not (Table 2). Basic injury characteristics—including polytraumatic injury, uni- versus bicondylar fracture pattern, concomitant ligamentous knee injury, or concomitant ipsilateral extremity injury—were also similar between skiers who returned to skiing and those who did not. Skiers who returned to skiing were more likely to be men (66% vs 41%; P = .018) and injured while skiing (P = .013). They also had significantly higher PROMIS-PF (51.9 ± 7.3 vs 47.2 ± 8; P = .006), KOOS-Pain (87.2 ± 10.7 vs 78.9 ± 16.8; P = .021), and KOOS-ADL (93.3 ± 7.5; P = .004) scores.
Return Versus No Return to Skiing: Demographic and Postoperative Data a

Data are presented as mean ± SD or percentage. ADL, Activities of Daily Living; BMI, body mass index; CCI, Charleston Comorbidity Index; KOOS, Knee injury and Osteoarthritis Outcome Score; PROM, patient-reported outcome measure; PROMIS-PF, Patient-Reported Measurement Information System– Physical Function; QOL, Quality of Life; Sport, Function in Sport and Recreation.
Based on responses to the custom questionnaire, more than half of the 41 skiers who returned to skiing did so 12 months after injury (Figure 2). The percentage of patients who self-reported feeling comfortable while skiing trailed the time of return, and only 78% of the return cohort reported ever achieving comfort while skiing. Before injury, the majority of patients who skied reported skiing at least 20 days per season and on expert terrain (53.7% and 61%, respectively). After injury, most patients reported skiing <11 days per season and skiing primarily on intermediate or easy terrain (56.1% and 70.7%, respectively) (Figures 3 and 4).

The proportion of patients who returned to skiing and reported they felt comfortable with skiing according to time after injury.

Reported number of skiing days per season before and after injury.

Reported terrain types skied before and after injury.
According to questionnaire responses, 66% of skiers reported that their skiing performance was “worse” or “much worse” at the final follow-up. Similarly, 58.5% of these patients reported that the enjoyment they experienced while skiing was “less” or “much less.” Only 28.21% of patients felt their injured leg did not limit their skiing ability. Skiers also consistently reported cognitive limitations associated with returning to skiing, with 61.54% of patients reporting that they were more cautious and 65% stating that the hardest aspect of returning to skiing was psychological.
Factors Associated With Return to Skiing
Table 3 shows the results of the multivariate logistic regression analysis. The male sex and KOOS-ADL scores independently predicted return to skiing (P = .006 and P = .028, respectively). The PROMIS-PF did not predict return to skiing in the multivariate model. The Nagelkerke R2 for the multivariate model was 0.300.
Results of Multivariate Regression Analysis a

KOOS-ADL, Knee injury and Osteoarthritis Outcome Score–Activities of Daily Living; PROMIS-PF, Patient-Reported Measurement Information System–Physical Function.
Discussion
We found that at a mean follow-up of 3 years after operative fixation of a tibial plateau fracture, 46% of patients had returned to skiing. Multivariate regression analysis indicated that a knee-specific functional PROM (KOOS-ADL) better predicted return to skiing when compared with a global functional PROM (PROMIS-PF) at the final follow-up. We also collected data regarding the frequency, terrain level, and patient-reported performance and enjoyment of skiing upon return to skiing postoperatively, adding to the existing literature on the subject. As skiing is the most common sports-related cause of tibial plateau fracture, 12 the data from this study will aid postoperative patient counseling for a frequently encountered clinical scenario. Accurate counseling in the peri-injury period is imperative to ensure that patients maintain realistic expectations for their postinjury function, as previous research has demonstrated that patients with tibial plateau fracture overestimate their expected functional recovery. 11
Previous data on return to sports after operatively treated tibial plateau fractures are limited. The rate of return to any sport has been estimated at around 70% in the midterm follow-up for patients treated with open reduction and internal fixation.12,20 Reported rates of return for skiing after tibial plateau fracture vary widely with estimates ranging7,9,16,17 from 53% to 88%. Most previous studies investigating return to skiing are limited by small sample sizes of ≤25 patients.7,9,17 Loibl et al 16 retrospectively studied return to sports in 92 patients with tibial plateau fractures (33% bicondylar) sustained while skiing and treated at a level 3 trauma center with primarily open reduction and internal fixation. In that cohort, 53% of patients returned to skiing. Similarly, Kraus et al 12 evaluated 89 patients with tibial plateau fractures, 58.4% of whom skied before injury and demonstrated that patients were overall likely to transition to lower-impact activities at a 2-year follow-up. However, they did not specifically evaluate return-to-skiing rates and satisfaction in those who returned to downhill skiing. We report a rate of return to skiing of 46% in the present study. We hypothesized that the variability in reported rates of return to skiing observed in the literature was related to differences in injury severity between study cohorts. All previous return-to-skiing studies in tibial plateau fractures have identified skiers as those whose injury occurred while skiing.4,9,16,17 Furthermore, 75% of previously identified return-to-skiing studies used cannulated screw fixation alone, which cannot successfully be applied to many high-energy injuries.7,9,17 When counseling patients regarding their postoperative outcome, the rate of return to skiing in the present study is likely a more generalizable estimate for patients undergoing open reduction and internal fixation for tibial plateau fracture because half of the patients in the present cohort sustained nonskiing-related injuries. Interestingly, within our cohort, there were no differences between groups in the rates of medial column fixation or bicondylar fracture, suggesting that hardware construct or complete articular injury do not provide further prognostic information regarding return to skiing. Finally, minimal prior literature has provided data on the timing of return to skiing. Based on the present study data, we believe it is reasonable to advise patients who desire to return to skiing that they should expect to return at least 12 months after injury.
We demonstrated that the PROMIS-PF, a marker of global PF, and multiple KOOS domains were significantly higher in the return-to-skiing group relative to the no-return group. Furthermore, the KOOS-ADL score independently predicted return to skiing, while the PROMIS-PF score was not predictive in multivariate analysis. Although several studies have published data on the KOOS and PROMIS-PF in tibial plateau fractures at a midterm follow-up, limited previous research has investigated patient-reported outcomes as predictors of return to sports.10,18,23 One previous study on return to sports in tibial plateau fractures demonstrated significant differences in the Short Musculoskeletal Function Assessment between the return and no-return groups. 13 To our knowledge, no previous literature has compared a global versus a joint-specific functional outcome score as predictors of return to sports. In our analysis, we hypothesized that the KOOS-ADL was more predictive for return to skiing because it represents a more sensitive measurement of knee function than the PROMIS-PF. The PROMIS-PF domain has been shown to be a reliable indicator of gross function. However, in this analysis, a PROMIS-PF range that includes athletes returning to skiing likely also includes active, independent individuals who do not have the knee function to ski reliably.
Many patients who returned to skiing reported decreasing their days on the mountain and choosing less challenging terrain postinjury relative to their preinjury baseline. Peak forces across the knee joint during downhill skiing have been demonstrated to be as high as 10 times the body weight on medium incline slopes. 14 Given the demands across the knee during skiing, particularly on more aggressive terrain, it is unsurprising that the number of skiers frequenting expert-level terrain dropped by half in our cohort. This finding aligns with previous research, which has demonstrated that patients report decreased participation in high-impact sporting activities after tibial plateau fracture. 12 Beyond physical limitations, 65% of the patients in our study reported that psychological factors were the greatest limitation in returning to skiing after their trauma. To our knowledge, the psychological aspects of return to sports have not been studied in tibial plateau fractures. However, this is a common area of research in other sport-related knee injuries, such as anterior cruciate ligament tears.2,15 Our data suggest that orthopaedic trauma populations may benefit from further research in this area and targeted interventions.
Limitations
This study has several limitations. Based on CPT coding, the injury data and patient baseline characteristics were collected retrospectively from the electronic medical record. This subjects the survey to the inherent limitations of a retrospective study and may not fully capture the number of patients treated for tibial plateau fractures at our institution. Furthermore, our medical center is within a 1-hour drive of 77 major ski resorts, which likely increases the percentage of skiing-related injuries relative to other centers and may make our findings less generalizable. Patient-reported outcomes data were collected via survey response rather than at clinic follow-up visits, and the data are susceptible to survey bias as a result. However, given that both the skiing and nonskiing groups responded to the survey, the impact of survey bias should be mitigated for most comparisons of interest in the present study data. In addition, the presence of meniscal injuries and fracture classification according to commonly used classifications, such as the Schatzker classification, may correlate with return to skiing and is an area for further investigation with larger, multicenter patient cohorts. Last, we limited our follow-up to a minimum of 10 months as surveys were not infrequently sent out before patients’ 1-year postoperative visit. This may not capture patients who were lost to follow-up and returned to skiing beyond this time point, resulting in an underestimation of the actual return-to-skiing rates, given that a large proportion of patients return to skiing beyond 12 months. However, our mean follow-up was 2.5 years for nonskiers and 3.2 years for skiers. A minimum follow-up of <1 year postoperatively is seen frequently within the orthopaedic trauma literature and is generally accepted as sufficient. Most routine fracture care is completed before 6 months postoperatively, and noncompliance within the orthopaedic trauma population limits the feasibility of longer-term follow-up.1,5,24 However, further analyses with longer-term follow-ups in multicenter cohorts are needed to evaluate whether more patients return to skiing beyond 10 months postoperatively.
Conclusion
Fewer than half of skiers who underwent operative fixation of a tibial plateau fracture could return to skiing at a mean 3-year follow-up. A knee-specific functional PROM outperformed a global functional PROM in predicting return to skiing. Skiers should be advised that their injury will likely cause lasting physical and psychological limitations relative to their preinjury baseline.
Footnotes
Appendix
Return-to-Skiing Questionnaire

| 1. Did you ski before your injury? If not, you have completed the questionnaire. |
| (A) Yes |
| (B) No |
| 2. Did you return to skiing after your injury? If not, you have completed the questionnaire. |
| (A) Yes |
| (B) No |
| 3. How long after your injury did you |
| (A) 0-6 months |
| (B) 6-12 months |
| (C) 12-18 months |
| (D) 18-24 months |
| (E) 24+ months |
| 4. How long after your injury did you |
| (A) 0-6 months |
| (B) 6-12 months |
| (C) 12-18 months |
| (D) 18-24 months |
| (E) 24+ months |
| (F) I still don't feel comfortable skiing. |
| 5. Please estimate the number of days you skied the season before |
| (A) 0-5 |
| (B) 6-10 |
| (C) 11-15 |
| (D) 16-20 |
| (E) 20+ |
| 6. Please estimate the number of days you skied the first full season |
| (A) 0-5 |
| (B) 6-10 |
| (C) 11-15 |
| (D) 16-20 |
| (E) 20+ |
| 7. Please rate your skiing |
| (A) I ski much worse than I did before injury. |
| (B) I ski slightly worse than I did before injury. |
| (C) I ski about the same as I did before injury. |
| (D) I ski slightly better than I did before injury. |
| (E) I ski much better than I did before injury. |
| 8. Please rate your skiing |
| (A) I enjoy skiing much less than I did before injury. |
| (B) I enjoy skiing slightly less than I did before injury. |
| (C) I enjoy skiing the same amount as I did before injury. |
| (D) I enjoy skiing slightly more than I did before injury. |
| (E) I enjoy skiing significantly more than I did before injury. |
| 9. Please choose a single selection below that best categorizes the type of terrain that you most commonly skied |
| (A) Easy—Mostly green runs; gentle, low-grade groomed terrain. |
| (B) Moderate— Mostly blue runs; a mix of groomed and ungroomed terrain, moderate grades, small moguls. |
| (C) Expert (mostly black, double black, or out-of-bounds runs; steep grades, mixed conditions, large moguls, tight trees, and other technical terrain features). |
| 10. Please choose a single selection below that best categorizes the type of terrain that you most commonly ski after your injury. |
| (A) Easy— Mostly green runs; gentle, low-grade groomed terrain |
| (B) Moderate—Mostly blue runs; a mix of groomed and ungroomed terrain, moderate grades, small moguls. |
| (C) Expert (mostly black, double black, or out-of-bounds runs; steep grades, mixed conditions, large moguls, tight trees, and other technical terrain features). |
| 11. Have you changed your skiing in other ways since your injury? |
| (A) Yes |
| (B) No |
| 12. If you answered Yes to question 5, please specify the changes you have made to your skiing routine. |
| 13. Please rate your current average pain while skiing on a scale of 0-10. |
| 14. Please rate your average pain at the end of a ski day on a scale of 0-10. |
| 15. Please rate your current average anxiety when skiing on a scale of 0-10. |
| 16. How much does your injured leg limit your skiing ability? |
| (A) A lot— my leg constantly limits my skiing ability. |
| (B) A little— there are times when my leg limits my skiing ability. |
| (C) None—my leg does not directly limit my ability to ski. |
| 17. Please state the hardest aspect of returning to skiing following your injury. |
Final revision submitted April 17, 2023; accepted May 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.L.R. has received speaking fees from AO Trauma North America and Synthes GmbH and has stock/stock options in Purgo Scientific. T.F.H. has received consulting fees from DePuy/Medical Device Business Services, Globus Medical, and OsteoCentric; speaking fees from Synthes GmbH; royalties from DePuy Synthes; and has stock/stock options in Imagen, NT nPhase, Orthogrid, and SMV Holdings. L.S.M. has received speaking fees from Synthes GmbH. J.M.H. has received consulting fees from Globus, KCI USA, Newclip Technics, Orthogrid, OsteoCentric Technologies, and Stryker; education payments from Summit Surgical; speaking fees from Synthes GmbH; and hospitality payments from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Utah, Utah, USA (No. 00114175).