
Abstract
Background:
Tibial plateau fractures account for a small portion of all fractures; however, these fractures can pose a surgical challenge when occurring concomitantly with ligament injuries.
Purpose/Hypothesis:
The purpose of this study was to compare 2-year outcomes of soft tissue reconstruction with or without a concomitant tibial plateau fracture and open reduction internal fixation. We hypothesized that patients with a concomitant tibial plateau fracture at the time of soft tissue surgery would have inferior outcomes compared with patients without an associated tibial plateau fracture.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Forty patients were included in this study: 8 in the fracture group and 32 in the matched control group. Inclusion criteria for the fracture group included patients who were at least 18 years old at the time of surgery and sustained a tibial plateau fracture and a concomitant injury of the anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, or fibular collateral ligament in isolation or any combination of cruciate or collateral ligaments and who subsequently underwent isolated or combined ligament reconstruction. Patients were excluded if they underwent prior ipsilateral knee surgery, sustained additional bony injuries, or sustained an isolated extra-articular ligament injury at the time of injury. Each patient with a fracture was matched with 4 patients from a control group who had no evidence of a tibial plateau fracture but underwent the same soft tissue reconstruction procedure.
Results:
Patients in the fracture group improved significantly from preoperatively to postoperatively with respect to Short Form–12 (P < .05) and Western Ontario and McMaster Universities Osteoarthritis Index total scores (P < .05). The Lysholm (P = .075) and Tegner scores (P = .086) also improved, although this was not statistically significant. Patients in the control group improved significantly from preoperatively to postoperatively across all measured scores. A comparison of the postoperative results between the 2 groups showed no statistically significant difference.
Conclusion:
The presence of a tibial plateau fracture in conjunction with a ligamentous knee injury did not have a negative effect on postoperative patient-reported outcomes. Patient-reported outcome scores after surgery in both the fracture and control groups improved beyond the minimally clinically important difference, indicating that the presence of a fracture did not detract from the outcomes observed in patients without fractures undergoing concomitant ligament reconstruction.
Tibial plateau fractures account for approximately 1% of all fractures 14 ; however, these fractures can pose a surgical challenge when occurring concomitantly with ligament injuries. Delamarter et al 4 first described the patterns of ligament injuries associated with tibial plateau fractures, reporting that lateral tibial plateau fractures most commonly occurred with medial collateral ligament (MCL) tears. Similarly, Bennett and Browner 1 reported that Schatzker type II and IV fractures were most commonly associated with soft tissue injuries and that Schatzker type II fractures were associated with MCL tears, while Schatzker type IV fractures were most commonly associated with meniscal injuries. In the setting of intra-articular soft tissue injures, tibial plateau fractures can compromise soft tissue reconstruction by altering joint geometry and by preventing anatomic tunnel placement. 15
Soft tissue injuries throughout the knee can be found in up to 99% of patients with concomitant tibial plateau fractures, and the overall incidences of anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) tears in patients with concomitant tibial plateau fractures have been reported to be 80% and 36%, respectively. The magnitude of the trauma, the position of the leg at the time of injury, and the bone quality often determine the fracture type and extent of soft tissue damage. Isolated knee ligament injuries without fractures have been reported to have a relatively good prognosis, with improved functional scores and return to sports after surgical treatment. 14,15 However, proximal tibial fractures can result in malalignment and postoperative osteoarthritis despite adequate treatment. Furthermore, patients with tibial plateau fractures are reported to often present with limb-specific and general health deficits at follow-up. 6,14,15
Although the association between tibial plateau fractures and ligamentous injuries is already known, the effect of these fractures on postoperative patient-reported outcomes has not been well studied. For this reason, the aim of this study was to compare 2-year outcomes of soft tissue reconstruction with or without concomitant tibial plateau fractures and open reduction internal fixation (ORIF). We hypothesized that patients with a concomitant tibial plateau fracture at the time of ligament reconstruction would have inferior outcomes compared to patients without an associated tibial plateau fracture.
Methods
Study Design
This study was approved by an institutional review board. A database of prospectively collected, institution-based patient outcomes was searched retrospectively. Inclusion criteria were as follows: patients who sustained a tibial plateau fracture and a concomitant injury of the ACL, PCL, MCL, or fibular collateral ligament (FCL) in isolation or any combination of cruciate or collateral ligaments, subsequently underwent surgery by a single surgeon; age older than 18 years and at most 60 years; and a minimum of 2 years of follow-up after index surgery. Patients were excluded from this study if they had undergone prior ipsilateral knee surgery, sustained additional bony injuries, or sustained an isolated collateral ligament injury. Patients were also excluded if they sustained additional ipsilateral or contralateral lower extremity injuries. To make postoperative outcomes comparable, each patient with a fracture was matched with 4 patients from a control group who had no evidence of a tibial plateau fracture but who underwent the same ligament reconstruction and meniscal repair procedures. In total, the control group consisted of 32 patients who were matched according to age, sex, body mass index (BMI), meniscal status, articular cartilage status, and ligament injury. Assuming an alpha of 0.05 and an independent-groups t test, 32 patients in the control group was sufficient to detect an effect size (d) of 0.8 with 80% statistical power. All patients included in this study sustained low-velocity injuries.
Patient Demographics
Preoperatively, demographic characteristics such as age, sex, and BMI were recorded, and conventional radiographs and magnetic resonance imaging (MRI) scans were obtained in all patients to evaluate for concomitant lesions. The chronicity of surgery was also recorded for all patients. Acute treatment was defined as surgery ≤6 weeks from injury, whereas chronic treatment was defined as treatment >6 weeks from injury. Intraoperatively, all injuries were graded and recorded. Chondral defects were graded using the Outerbridge classification. 2 Patient demographics are reported in Table 1.
Patient Demographics and Characteristics a

a Values are reported as mean ± SD unless otherwise specified. ACL, anterior cruciate ligament; FCL, fibular collateral ligament; MCL, medial collateral ligament; N/A, not applicable; PCL, posterior cruciate ligament.
Subjective Patient Outcomes
Preoperatively and at a minimum of 2 years after index surgery, patients were administered a subjective questionnaire that included the following clinical outcome measures: Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total score, Lysholm score, Short Form–12 physical component summary (SF-12 PCS), Tegner activity scale, and patient satisfaction rating (measured on a 1-10 scale, with 10 being very satisfied and 1 being very unsatisfied). Failure was defined as a subsequent operative procedure for arthrofibrosis, revision reconstruction for graft laxity (>5-mm side-to-side difference on clinical examination ), meniscal repair failure, and a reconstruction graft rupture.
Surgical Technique
Anatomic-based reconstruction was performed to reconstruct the torn ligaments as previously described. 3,5,7 –13 All PCL tears were treated with anatomic double-bundle PCL reconstruction with an Achilles tendon allograft for the anterolateral bundle and a tibialis anterior allograft for the posteromedial bundle. ACL tears were reconstructed with a patellar tendon autograft. Tears of the superficial MCL were reconstructed with a hamstring autograft. FCL tears were reconstructed with a semitendinosus autograft or allograft, while complete posterolateral corner (PLC) reconstruction was performed with a split Achilles tendon allograft. The sequence of graft fixation depended on the involved ligament reconstruction procedure. When the PCL was reconstructed, the anterolateral bundle of the PCL was always fixed first at 90° to restore the normal tibial step-off, followed by the posteromedial bundle of the PCL in extension and neutral rotation. In patients undergoing FCL or complete PLC reconstruction, the FCL or PLC reconstruction grafts were tensioned after the PCL but before the ACL and posteromedial corner. The FCL was fixed at 20° to 30° of knee flexion and with a slight valgus force and in neutral rotation, followed by the rest of the PLC structures (popliteus tendon and popliteofibular ligament) at 60° of knee flexion and neutral rotation. The ACL was fixed in full extension, and the posteromedial corner was always fixed last, with the superficial MCL fixed at 20° to 30° and the posterior oblique ligament repaired or reconstructed at 0° and in neutral rotation. All surgeries were performed with a tourniquet, with all grafts placed and meniscal repair completed within 2 hours. The tourniquet was let down for surgical incision closure. In accordance with the existing literature, patients were considered to be treated in the acute phase if they underwent multiligament reconstruction in ≤3 weeks, while patients treated >3 weeks from injury were considered to be treated in the chronic phase. A preoperative MRI scan and postoperative radiograph of a patient with a tibial plateau fracture are shown in Figure 1.

(A) Coronal magnetic resonance imaging scan of a patient with an anterior cruciate ligament injury with a concomitant tibial plateau fracture. (B) Six months postoperatively, an anteroposterior plain radiograph demonstrates tibial plateau fixation.
Rehabilitation
Physical therapy was performed immediately postoperatively and focused on early quadriceps muscle activation and assisted knee flexion from 0° to 90°. Starting 2 weeks postoperatively, knee flexion was increased to full motion as tolerated. At 6 weeks postoperatively, weightbearing was initiated along with the utilization of a low-resistance stationary bicycle and 25% body-weight leg presses to a maximum of 70° of knee flexion. Once the patients developed good dynamic neuromuscular control without any pain, they were allowed to progress to their functional sport-specific exercises. Patients who underwent a multiligament reconstruction procedure typically required 9 to 12 months of rehabilitation before returning to full activities.
Statistical Analysis
Statistical analysis was performed by use of the SPSS software package (version 22.0; SPSS). Statistical power was considered for this study in terms of the effect size detectable when testing the primary hypothesis given the fixed sample size. The distribution of data was tested by using the Kolmogorov-Smirnov test, showing nonnormal distribution for all scores. Therefore, preoperative and postoperative scores were compared using Wilcoxon tests. To compare the patients with a fracture to those in the control group, independent testing (Mann-Whitney U test) was applied. Outcomes are presented as median and range values. All reported P values are 2-tailed, with P < .05 indicating statistical significance.
Results
Patient Demographics
Between 2010 and 2014, 14 consecutive patients underwent ORIF of tibial plateau fractures. Of these 14 patients, 12 (86%) were available for follow-up at a minimum of 2 years after surgery, with a mean follow-up of 3.1 years (range, 2-4 years). Two patients did not complete the minimum postoperative follow-up and were excluded. An additional 2 patients did not suffer from a concomitant ligament lesion and were also excluded. The remaining 8 patients fulfilled the inclusion criteria and were assigned to the fracture group. Twenty-eight (88%) patients in the control group were treated acutely, while all 8 patients in the fracture group were treated acutely (P = .566). No postoperative failures were observed at a minimum of 2 years after index surgery in the fracture group. Two patients in the control group went on to undergo revision reconstruction: 1 patient underwent revision MCL reconstruction after a sport-related injury, and 1 patient underwent revision ACL reconstruction because of primary reconstruction tunnel osteolysis and persistent instability. No significant differences in patient characteristics were observed between the groups. The patient characteristics of both groups are presented in Table 1.
Injury Patterns and Concomitant Injuries
In the fracture group, 4 patients had 2 ligaments torn, 3 patients had 1 ligament torn (1 cruciate ligament in all of the patients), and 1 patient had 3 ligaments torn (ACL, PCL, and MCL). All patients in the fracture group underwent ORIF for their tibial plateau fractures during ligament reconstruction surgery. The distribution of the ligamentous tear pattern in the fracture group is reported in Table 2. Five patients in the control group (15.6%) were found to have chondral defects at the time of surgery; no patients in the fracture group were found to have chondral damage in addition to their tibial plateau fracture. All patients with chondral defects were treated with chondroplasty. Six patients (75%) in the fracture group had concomitant meniscal injuries: 5 lateral meniscal tears and 1 medial meniscal root tear. Twenty patients (63%) in the control group had concomitant meniscal injuries: 12 lateral meniscal injuries and 8 medial meniscal root tears. All meniscal tears were treated with inside-out repair. No additional meniscus surgery was necessary in the follow-up period.
Injury Pattern in Fracture Group With Corresponding Schatzker Type and Subsequent Surgical Intervention a
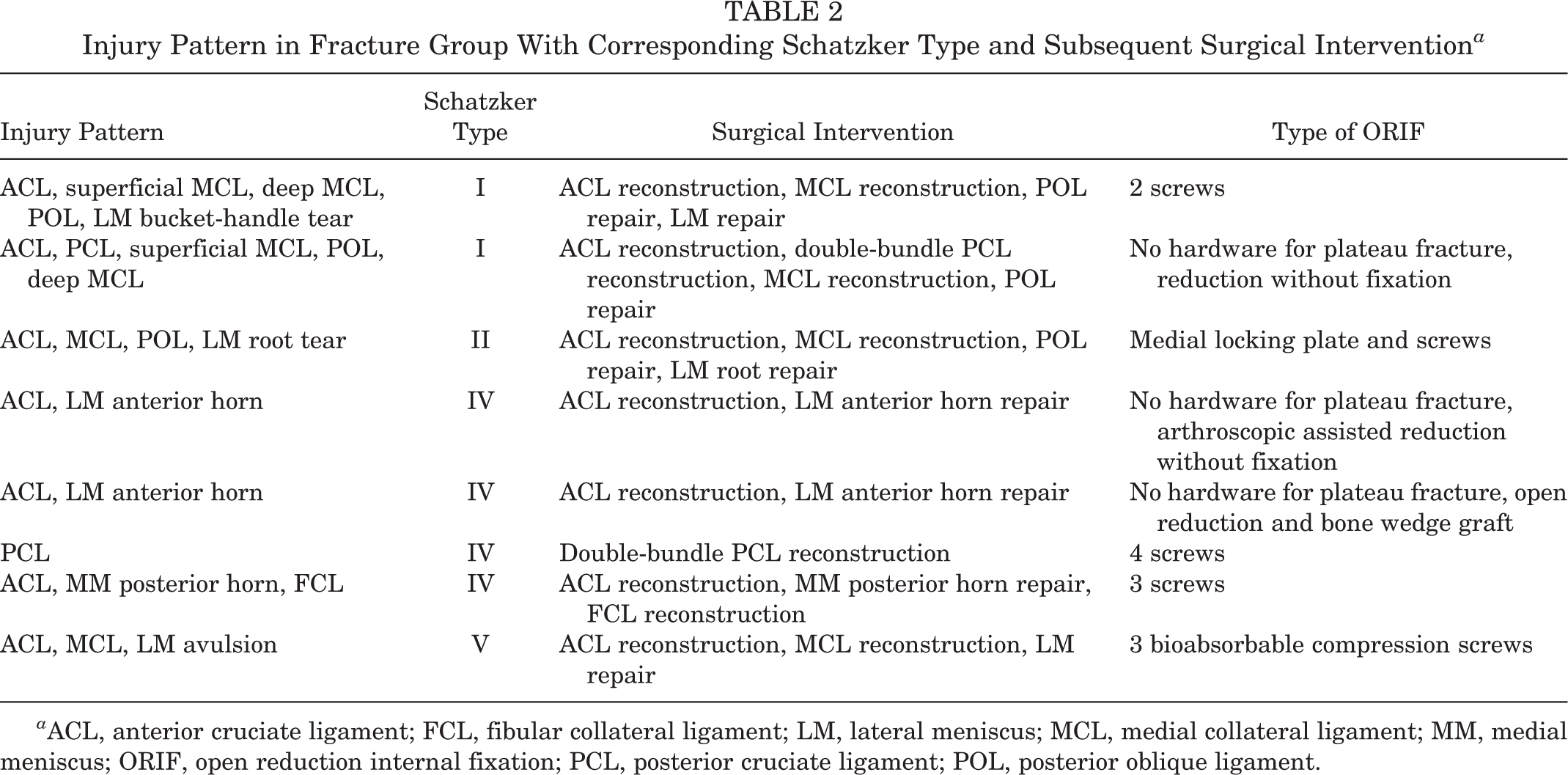
a ACL, anterior cruciate ligament; FCL, fibular collateral ligament; LM, lateral meniscus; MCL, medial collateral ligament; MM, medial meniscus; ORIF, open reduction internal fixation; PCL, posterior cruciate ligament; POL, posterior oblique ligament.
Patient-Reported Outcomes
Patients in the fracture group improved significantly from preoperatively to postoperatively with respect to SF-12 PCS (P < .05) and WOMAC total scores (P < .05). The Lysholm (P = .075) and Tegner scores (P = .086) also improved, although not in a statistically significant manner (Table 3). Patients in the control group improved significantly from preoperatively to postoperatively across all measured scores (Table 3). A comparison of the postoperative results between the 2 groups showed no statistically significant difference (Table 4).
Patient-Reported Outcome Scores a

a Values are reported as median (range). N/A, not applicable; SF-12 PCS, Short Form–12, physical component summary; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Statistically significant.
Comparison of Postoperative Patient-Reported Outcome Scores for Fracture and Control Groups a

a Values are reported as median (range). SF-12 PCS, Short Form–12, physical component summary; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Discussion
The main finding of this study was that the presence of a tibial plateau fracture did not have a negative effect on postoperative patient-reported outcomes after concurrent ligament reconstruction and ORIF of tibial plateau fractures. We observed a significant improvement in SF-12 PCS and WOMAC scores after surgery in the fracture group and an improvement in Lysholm and Tegner scores, although this was not statistically significant. Although these improvements were not statistically significant, the scores were greater than the minimally clinically important difference reported in the literature. 14 When comparing the fracture group to the control group with a similar ligament injury pattern, no significant difference in postoperative scores between the 2 groups was found. Based on these observations, knee ligament reconstruction can be safely performed concurrently with ORIF of tibial plateau fractures.
There is still some controversy in the literature as to whether ligament injuries with concomitant fractures should be treated with staged management. The concurrent placement of hardware for tibial plateau fractures may pose a challenge for ligament reconstruction. This study demonstrated that despite the challenge of concomitant fractures with ligament tears, outcomes comparable to ligament tears without fractures can be achieved after single-stage surgery. Unlike Delamarter et al, 4 who concluded that a cruciate ligament injury associated with a tibial plateau fracture carries a poor prognosis, our study showed that isolated and combined cruciate ligament injuries in the setting of a tibial plateau fracture can have good outcomes. Tibial plateau fractures without concomitant ligament tears are challenging and have poor outcomes, depending on the fracture type.
The prevalence of ligament tears associated with tibial plateau fractures and the prevalence of tibial plateau fractures associated with knee ligament tears are variable in the literature. An MRI analysis of 103 patients with tibial plateau fractures revealed a 99% incidence of soft tissue injuries around the knee, with 77% having a complete cruciate or collateral ligament rupture. 5 The MCL is reported to be most commonly injured in the setting of tibial plateau fractures, with an incidence of 20%. 4 The next most frequently injured ligament in the setting of plateau fractures is the ACL, with an incidence of 10%. 4 A fracture of the posterolateral tibial plateau has been reported in some case reports and is associated with combined violent internal tibial rotation/anterior tibial translation. 15 However, MRI studies have reported a higher prevalence of occult fractures in the posterolateral tibial plateau in association with ACL tears. Taken together, the existing literature indicates that tibial plateau fractures are not a rare occurrence in the setting of ligamentous injuries. The findings of the present study build on the existing literature by demonstrating that a patient undergoing single-stage ligamentous reconstruction and ORIF of a tibial plateau fracture can be expected to have equivalent outcomes as a patient without a concomitant tibial plateau fracture.
Limitations
This study is not without limitations. The data were examined retrospectively, and as such, the inherent limitations in retrospective studies exist. However, all data were collected prospectively and stored in a registry database. The study is also limited by the low number of patients with associated tibial plateau fractures. Further, although the groups were matched closely by sex, age, BMI, and injury pattern, inherent and undetectable differences may be present, such as additional injuries or procedures differing from the matched group. Finally, given that the senior surgeon operates at a referral clinic, obtaining radiographs to assess the progression of osteoarthritis was not possible.
Conclusion
The presence of a tibial plateau fracture in conjunction with a ligamentous knee injury did not have a negative effect on postoperative patient-reported outcomes. Patient-reported outcome scores after surgery in both the fracture and control groups improved beyond the minimally clinically important difference, indicating that the presence of a fracture did not detract from the outcomes observed in patients without fractures undergoing concomitant ligament reconstruction.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: G.M. receives research support from South Eastern Norway Health Authorities and Arthrex. R.F.L. receives royalties from Arthrex and Smith & Nephew; is a paid consultant for Arthrex, Ossur, and Smith & Nephew; and receives research support from Arthrex, Linvatec, Ossur, and Smith & Nephew.
Ethical approval for this study was obtained from the Vail Valley Medical Center Institutional Review Board (protocol #2002-03).