
Abstract
Background
High-grade fracture of the posterolateral tibial plateau (PLTP) has been reported to increase bone loss, which in turn is associated with residual rotational instability and impaired function after anterior cruciate ligament (ACL) reconstruction.
Purpose
To investigate whether high-grade impaction fracture in PLTP is associated with the rate of return to sports (RTS) after ACL reconstruction (ACLR).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study retrospectively analyzed data from patients with complete ACL tears between December 2018 and June 2022. Inclusion criteria included primary ACLR with autologous hamstring reconstruction, standard preoperative magnetic resonance imaging (MRI) evaluation, and at least 2 years of postoperative follow-up. In contrast to bone contusions, a high-grade impaction fracture in PLTP is defined as subchondral or cortical bone displacement in this area involving the articular surface. Based on whether or not there were high-grade impaction fractures seen on the preoperative MRI, patients were divided into 2 groups: high-grade fracture and control group. Patients were followed up after surgery to assess their level of RTS, Tegner score, Lysholm score, and recovery time. The chi-square test was used to compare the differences in the RTS rate between the 2 groups.
Results:
Among 190 patients, 34 patients (17.9%) were in the high-grade group, while 156 patients (82.1%) were in the control group. Among the main outcomes, the high-grade fracture knee group performed worse in return to any sport (Tegner score ≥5) (71% vs 88.9%; P = .002) and level 1/2 (cutting) sports (26.5% vs 46.2%; P = .035), while there was no significant difference in return to strenuous sports (Tegner score ≥6) (48.4% in the high-grade group and 62.7% in the control group; P = .136) and return to play (2.9% in the high-grade group and 10.3% in the control group; P = .317). In the later follow-up period of survival analysis, the rate of recovery of any sport was slower in the high-grade fracture group (hazard ratio, 0.22; 95% CI, 0.07-0.72; P = .0118).
Conclusion:
The results of this study showed that high-grade impaction fracture of PLTP was associated with the rate of RTS after ACLR, mainly in the rate of return to any sport and level 1/2 (cutting) sports. Accordingly, the rehabilitation strategies and priorities for such patients should be adjusted to compensate for the impact.
Acute anterior cruciate ligament (ACL) injuries are often associated with bone bruising. More than 80% of patients with acute ACL injuries show bone bruises at different sites on postinjury magnetic resonance imaging (MRI).17,25 The posterolateral tibial plateau (PLTP) is a common site for multiple injury patterns in bone contusion.4,17,21,22,25 Posterolateral impaction fractures of the tibial plateau occur more frequently in high-energy injuries with extensive ACL tears or even ruptures, with a reported incidence of 49% to 85%.1-3,10 In contrast to low-grade ACL tears, PLTP damage can range from bone bruises to displaced impaction fractures in high-energy injuries, 3 and shear or depressed fragments may even appear in the tibial plateau in higher-energy injuries.
PLTP impaction fractures are more severe than bone bruises, and T1-weighted MRI shows cortical discontinuity with partial articular depression. It has been proposed that impaction fractures involving the articular surface should be defined as high-grade impaction fractures, which can cause a decrease in the depth of PLTP. 10 Milinkovic et al 20 this type of high-impaction fracture to the “Bankart knee.” Mechanical studies have shown the important role of the posterior horn of the lateral meniscus in knee stability, which is reflected in the increased stability of tibial internal rotation and forward translation during knee flexion.7,11,19,23 The intact tibial plateau is also an important bone support for the meniscus in converting axial stress into circumferential stress.14,19 Therefore, PLTP high-impaction fractures cause bone loss on the lateral tibial plateau, which may affect return to sports (RTS) after ACL reconstruction (ACLR). Milinkovic et al 20 verified the biomechanical impact of such fractures on the kinematics of the knee joint in cadaveric models. Bernholt et al 3 evaluated and found that highly incarcerated fractures were associated with increased pivot displacement and poor postoperative prognosis after ACLR. However, research on the relationship between high-grade impaction fractures in PLTP and the rate of RTS after ACLR in clinical practice is still lacking.
This study aimed to investigate whether a high-grade fracture in PLTP was associated with the rate of RTS after ACLR. It was hypothesized that patients undergoing ACLR with PLTP impaction fractures would have a significantly lower RTS rate compared to patients undergoing ACLR without PLTP impaction fractures.
Methods
Patient Selection
This study was approved after local institutional review board review (IRB No. 2024-072). This retrospective cohort study analyzed the data of patients who underwent ACLR between December 2018 and June 2022. All the surgeries were performed by the same group of surgeons. Data were extracted from electronic medical records and follow-up surveys were administered during routine clinical visits. The inclusion criteria were primary ACLR combined with autologous hamstring ligament reconstruction, standard preoperative MRI evaluation, and completion of at least 2 years of postoperative follow-up. The exclusion criteria were previous surgical history of the affected knee, past or current ACL injury to the contralateral knee, multiple ligament injuries with indications for additional surgical intervention, and extensive cartilage injury (Figure 1). Surgeries involving revision and reconstruction of the ACL and patients who underwent total lateral meniscectomy were also excluded, while those who underwent meniscal repair were included. Postoperative rehabilitation generally follows a conventional plan, with crutches for 4 to 6 weeks and braces for 6 to 8 weeks. The knee flexion angle reached 90° within 1 week and 120° within 6 weeks, and the normal full angle was achieved 3 months after the operation. Specific adjustments were made based on the individual's recovery progress.
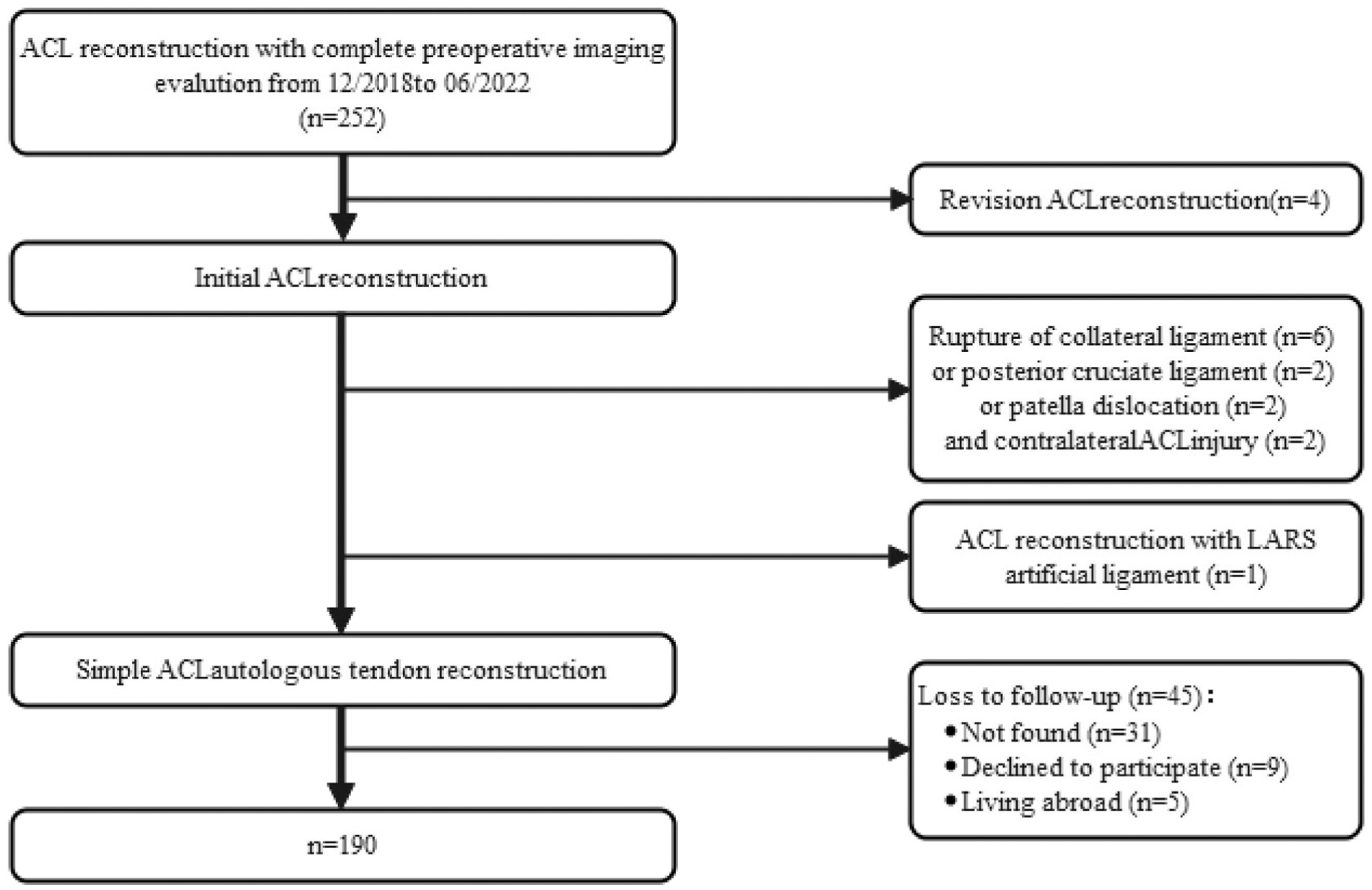
Flowchart of the patient selection process. ACL, anterior cruciate ligament.
Radiographic Assessment
A senior radiologist (Y.Q.) blinded to the clinical data reviewed preoperative MRI scans of the included patients. The MRI sequence used for analysis was a sagittal slice taken at the 50th percentile of the lateral width of the tibial plateau. The presence of impaction fractures in the PLTP was evaluated. Impaction fractures were diagnosed only when sagittal T1-weighted MRI scans revealed the subchondral bone or cortical bone displacement in the PLTP. 2 Subsequently, the impaction fractures were classified according to the method of Bernholt et al. 2 Type 1 was posterior cortex impaction of the lateral tibial plateau without accumulation on the articular surface. Type 2 was defined as an impaction fracture involving the articular surface. Type 3 was displacement of bone fragments, including shear (type 3A) and depressed (type 3B) fragments.1-3 In this study, we followed the method of Milinkovic et al 10 and described type 2 and above, involving the inferior surface of the fibular epithelial joint, as high-grade impaction fractures. According to the presence or absence of high-grade impaction fractures on preoperative MRI, patients were divided into the high-grade fracture group or control group (Figure 2).

Impaction fractures of the posterolateral tibial plateau in the (A and B) control and (C and D) high-grade fracture groups. Magnetic resonance imaging (MRI) scans of (A and B) the right knee joint obtained in a 38-year-old patient and (C and D) the left knee joint obtained in a 40-year-old patient, both with anterior cruciate ligament injuries. (A) T1-weighted MRI scan showing a posterolateral fracture of the tibial plateau not involving the articular surface, corresponding to low-grade fracture with a small cortical buckle (arrow). (B) T2-weighted MRI scan showing hyperintense signal alteration with intact fibers of the distal anterolateral complex (arrow). (C) T1-weighted MRI scan showing that the fracture involves the joint surface, resulting in a reduction in the depth of the lateral tibial plateau, corresponding to a higher grade (arrow). (D) T2-weighted MRI scan showing high signal changes and disrupted signals in the posterolateral tibial plateau, consistent with a high-grade injury (arrow).
Clinical Evaluation
Demographic information (including sex and age), cause of injury, time from injury to surgery, and surgical records (whether there were multiple ligament injuries requiring additional surgical intervention and whether meniscal surgery was performed) were collected for all patients.
Patients were followed for at least 2 years after surgery. For RTS, we looked at whether the optimal level at which the patient could recover had reached the following levels: (1) return to any sport (Tegner score ≥5), 13 (2) return to strenuous sports (Tegner score ≥6), 13 (3) return to level 1/2 (cutting) sports,6,8,15,16 and (4) return to play.6,9 If the ligament ruptured within 2 years and required revision surgery, the patient was classified as not being able to RTS (no postoperative Tegner level). 24 The primary outcome was the rate of return to any sport, while the recovery rates of other sports levels, Lysholm scores, and time from surgery to return to any sport were regarded as secondary outcomes.
Statistical Analysis
Categorical variables are described as frequency and percentage, continuous variables with nonnormal distribution are presented as median and range, and normally distributed variables are presented as mean and standard deviation. The Shapiro-Wilk test was used to analyze the normality of the variables. The chi-square or Fisher exact test was used to confirm the differences in RTS rate between the high-grade fracture group and low-grade fracture group. A t test was used to ascertain the difference in the mean RTS time between the 2 groups. Because Lysholm scores did not conform to a normal distribution, a nonparametric test was used to compare the groups. Group, age, sex, injury time, and meniscal injury were included in univariate logistic regression to explore their relationship with return to any sport.
In addition, survival analyses were performed to compare the likelihood of return to any sport between the 2 groups. The outcome event was defined as patients’ self-reported subjective sense of return to any sport. If the curves intersected with each other, landmark was used to analyze and calculate the hazard ratio (HR) of two groups of return to sports at different time periods. Finally, the log-rank test was used to compare the difference in survival curves between the 2 groups.
All data were analyzed using SPSS (Version 25.0; IBM) and R (Version 4.2.0; R Foundation for Statistical Computing). All tests were 2-tailed, and statistical significance was set at a P value <.05.
Results
Patient Characteristics
Based on the criteria, 190 patients (164 men, 26 women) were included in the study (Figure 1). Among them, 34 patients (17.9%) were in the high-grade compression fracture group, while 156 patients (82.1%) were in the control group. The median times from injury to surgery of the high-grade fracture and control groups were 0.8 months (IQR, 0.2-3.0 months) and 1 month (IQR, 0.2-4.0 months), respectively. In both groups, only a few patients had inactive exercise levels before injury (14.7% in the high-grade fracture group and 5.8% in the control group; P = .148). There were no statistically significant differences in baseline characteristics between the 2 groups (Table 1).
Patient Characteristics and Preoperative Data a
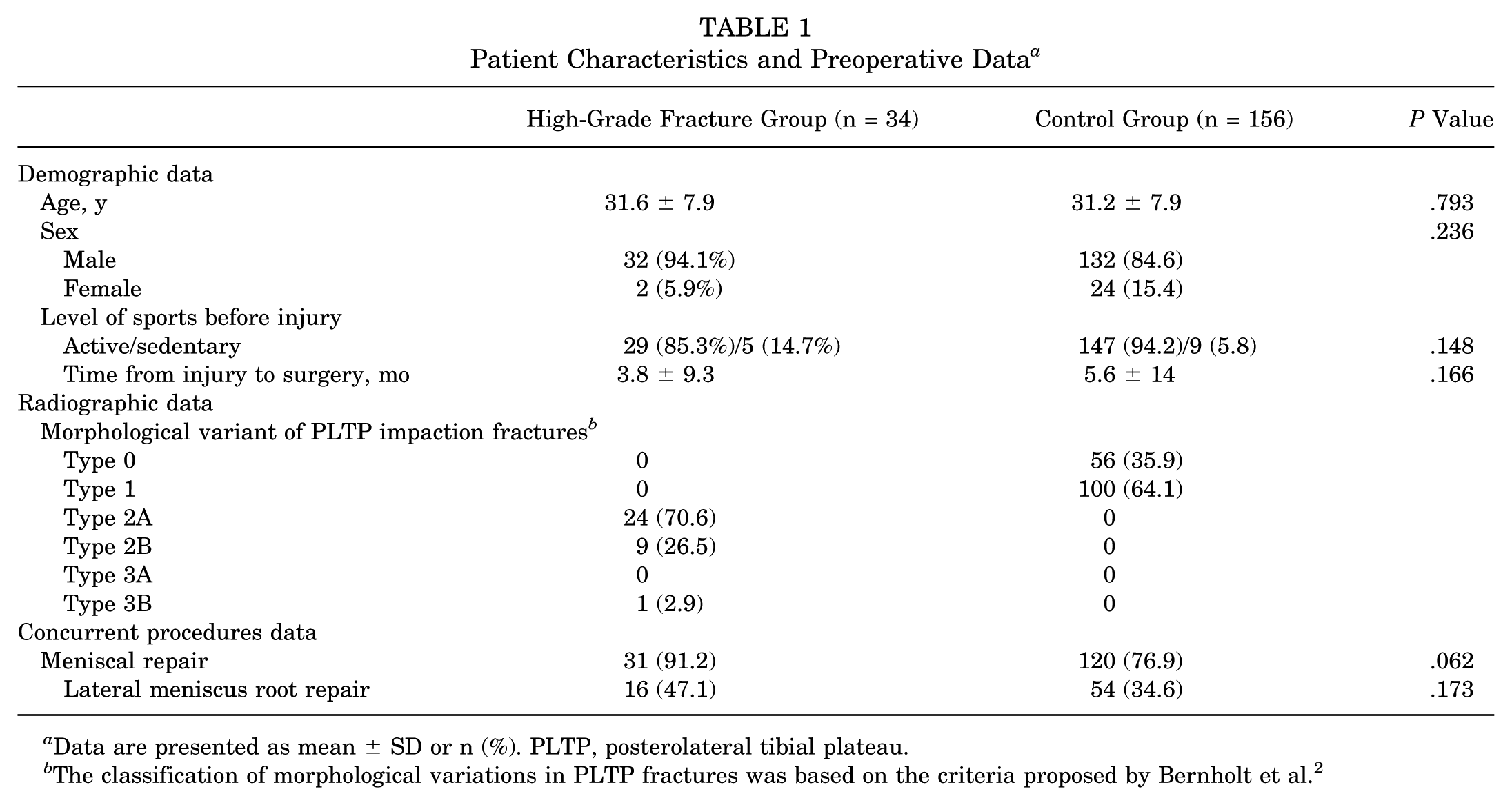
Data are presented as mean ± SD or n (%). PLTP, posterolateral tibial plateau.
The classification of morphological variations in PLTP fractures was based on the criteria proposed by Bernholt et al. 2
Primary Outcomes
The median Tegner score level was 5 (range, 4-6) in the high-grade fracture group and 6 (range, 5-6) in the control knee group (Table 2). For any sports (Tegner score ≥5), the rate of return was lower in the high-grade fracture group than in the control group (71% vs 88.9%; OR, 0.27; 95% CI, 0.116-0.628; P = .002) (Table 3).
Postoperative Follow-up Clinical Evaluation Results a

Data are presented as mean ± SD or median (range).
Rate of Return to 4 Levels of Sports 2 Years After Surgery in Both Groups a

Boldface type indicates a statistically significant difference between the 2 groups (P < .05).
Secondary Outcomes
At the same time, the proportion of the high-grade fracture group returning to level 1/2 (cutting) sports was lower than that of the control group (26.5% vs 46.2%; OR, 0.42; 95% CI, 0.184-0.958; P = .035). However, for strenuous sports (Tegner score ≥6), although recovery rates were lower in the high-grade fracture group than in control group, there was no statistical difference between the 2 groups (48.4% vs 62.7%; OR, 0.493; 95% CI, 0.233-1.044; P = .136). There was also no statistical difference between the 2 groups in returning to play (2.9% in the high-grade fracture group and 10.3% in the control group; OR, 0.265; 95% CI, 0.034-2.071; P = .317) (Table 3). There were no significant differences in postoperative Lysholm scores (89 ± 12.9 for the high-grade fracture group and 90.7 ± 9.9 for the control group; P = .911) and time from surgery to return to any sport (12.1 ± 4 months for the high-grade fracture group and 13.3 ± 5.5 months for the control group; P = .463) between the 2 groups (Table 2). Among the patients who did not RTS, 6 experienced graft rupture within 2 years after surgery (3 in the high-grade fracture group and 3 in control group). There was no statistically significant difference in the failure rate of ACLR grafts between the 2 groups (8.8% in the high-grade fracture group and 2% in the control group; P = .123).
Survival Analysis
In the survival analysis, the curves of the 2 groups overlapped, indicating changes in basic risk at different time periods of follow-up. In this paper, the follow-up time was divided into 2 periods with 17 months as the boundary for landmark analysis. At this time, a P value >.05 of the proportional hazard diagnosis was in line with the assumption of equal proportional risk. There was no significant difference between the 2 groups in the early stage (before 17 months) (HR, 0.85; 95% CI, 0.52-1.17; P = .5136). However, in the later period (after 17 months), although the number of cases returning to any sport increased over time in both groups, the number of cases returning to any sport increased more slowly in the high-grade fracture group (HR, 0.22; 95% CI, 0.07-0.72; P = .0118) (Figure 3). In other words, the high-grade fracture group was 78% less likely to have an RTS event than the control group in the later period.

Kaplan-Meier survival curves (changes in the probability of nonreturn to any sport) for the control group and the high-grade group.
Logistic Regression
In the univariate regression analysis, whether high-grade fractures occurred was a risk factor for returning to any sport (OR, 0.3; 95% CI, 0.13-0.69; P = .005). The remaining factors (including age, sex, injury time, and meniscal injury) had no effect on whether the event of returning to any sport occurred or not in this study (Figure 4). In addition, the multimodel approach also verified this conclusion. Model 1 is a single-factor model for high-grade fractures and RTS, while model 2 incorporates confounding factors such as demographic variables (Table 4).

Forest plot of hazard ratios according to patient characteristics at baseline.
Logistic Regression Analysis of Association Between High-Grade Fractures and Rate of RTS a

RTS, return to sports.
Crude model.
Model adjusted for age, sex, time from injury to surgery, and meniscal repair.
Discussion
The results of this study support the original hypothesis that high-grade impaction fractures of the lateral tibial plateau reduced the rate of return to any sport (Tegner score ≥5) (71% in the high-grade fracture group and 88.9% in the control group; P = .02) and level 1/2 (cutting) sports (26.5% the high-grade fracture group and 46.2% in the control group; P = .035).
The study focuses on the rate of RTS, analyzing the level of RTS from multiple hierarchical perspectives. The proportions of the high-grade fracture group in both returning to any sport and returning to cutting sports was significantly lower than those of the control group (Table 3). In the survival analysis, the high-grade fracture group returned to any sport at a slower rate from 1.5 years after surgery (HR, 0.22; P = .0118) (Figure 3), suggesting that this type of fracture has an adverse impact on long-term prognosis. Impaction fractures of PLTP, especially those of higher grades in morphological classification, may leave residual changes in the bone geometry of the tibial plateau. The change in the geometry of the lateral tibial plateau may have an impact on the degree of knee joint relaxation and kinematics. In particular, the shortening of the anterolateral length of the tibia and the increase in the tibial inclination will aggravate the degree of anterolateral rotational instability10,12,14,18,20 and asymmetric axial pivot movement. In PLTP, impaction fractures with a bone loss ratio exceeding 10% or a depression >2 mm may exacerbate rotational instability in ACL-deficient knees. 10 Similarly, current research has found that an increase in tibial plateau bone loss is associated with a lower Tegner score and rerupture of the ACL.1,3 In addition, since high PLTP impaction fractures are highly associated with lateral meniscus tears, 1 the torn meniscus may not adequately buffer and distribute the pressure. At the same time, the bone loss of PLTP causes the lateral meniscus heel to lose support, and the rotational instability of the knee joint increases. The PLTP extremely severe compression fracture model designed by Milinkovic et al 20 also supports this explanation.
In the univariate analysis, high-grade impaction fractures were significantly associated with a decreased rate of returning to any sport (Figure 4). It has been previously reported that high-grade posterior lateral platform impaction fractures of the tibia are associated with accompanying meniscal and ligament abnormalities, 1 which may affect the prognosis after ACLR. Therefore, statistical analysis was conducted to control the accompanying meniscal or ligament abnormalities. After adjusting for age, sex, injury time, and meniscal injury, high-grade impaction fractures were still associated with return to any sports and cutting sports (Table 4).
In this study, the high-grade impaction fracture group performed significantly worse than the control group in terms of the levels of cutting and rotational sports. Moreover, the risk of secondary rupture of ACL is higher in the high-grade impaction fracture group. Current research has found that high-grade impaction fractures of PLTP increase the translational and anterolateral rotational instability in ACL-deficient knees. 20 The most recent evidence-based clinical practice guidelines developed by the American Academy of Orthopaedic Surgeons for the treatment of ACL injuries (2022 edition) 5 state that anterolateral ligament (ALL) reconstruction or LET surgery may be considered in addition to ACLR for certain patients (those at a higher risk of rotational instability and/or ACL rerupture) despite the lack of long-term clinical evidence. We have reasons to suspect that for patients with a high-grade fracture, ALL or LET procedures will also need to be added during the operation.
Limitations
This study has several limitations. First, the loss to follow-up rate in this study was 19%, which may lead to follow-up bias. Because of the long study period and poor patient compliance, some patients failed to complete the final follow-up. Despite the problem of loss to follow-up, the data quality and statistical processing methods of this study still support the reliability of the conclusions, which can be further verified in the future with larger samples. In addition, owing to the retrospective design of this study, recall bias is possible, which may lead to an underestimation or overestimation of patient-reported outcomes. However, it is anticipated that any impact of recall bias would be minimal as the significant events experienced during recovery are generally considered memorable.
Conclusion
This study shows that high-grade impaction fractures of PLTP are associated with the rate of RTS after ACLR, mainly in the rate of return to any sport and level 1/2 (cutting) sports. Accordingly, the rehabilitation strategies and priorities for such patients should be adjusted to compensate for the impact.
Footnotes
Final revision submitted January 2, 2026; accepted January 8, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was partially supported by the Shenzhen Health Economics Association (No. 202353), the Shenzhen Science and Technology Innovation Committee Projects (No. JCYJ20220530160218040), the Teaching Reform Research Project of Shenzhen University (No. JG2022165), the General Program for Clinical Research at Peking University Shenzhen Hospital (No. LCYJ2020005), the Guangdong Sports Bureau (No. GDSS2020N002), the Natural Science Foundation of Guangdong Province (No. 2017A030310616), the Shenzhen “San-Ming” Project of Medicine (No. SZSM202211019), and the Medical Scientific Research Foundation of Guangdong Province (Nos. A2017202 and A2024319). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Institutional Review Board of Peking University Shenzhen Hospital (IRB No. 2024-072).
Date Accessibility Statement
Data are available on reasonable request.