
Abstract
Background:
Rotator cuff tears are common injuries that are reliably treated with arthroscopic repair, producing good to excellent results. The Western Ontario Rotator Cuff (WORC) index is a validated disease-specific instrument used to assess patient outcomes; however, no study to date has correlated WORC index with treatment failure.
Purpose:
To evaluate the WORC index as a predictor for successful treatment in arthroscopic rotator cuff repair. An additional purpose was to identify patient and tear characteristics associated with risk of treatment failure.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This study reviewed a total of 500 patients who underwent arthroscopic rotator cuff repair with a minimum of 2-year follow-up. Patient charts were reviewed for treatment failures, defined as persistent or recurrent shoulder pain or weakness, leading to further workup and identification of a failure to heal or recurrent tear by magnetic resonance imaging. Patient demographic and comorbidity data were gathered and correlated with risk of failure. All patients completed WORC questionnaires, and scores were correlated with risk of treatment failure.
Results:
There were 28 (5.6%) treatment failures at a median 28 weeks (SD, 42 weeks) postoperatively. Patients claiming workers’ compensation were 3.21 times more likely (odds ratio; P = .018) to fail treatment. Posterior interval tears (those including infraspinatus) were 3.14 times more likely (P = .01) to fail than anterior interval tears. Tear size was associated with treatment failure; the odds of failure was 3.24 for a 2-tendon tear and 5.83 for a 3-tendon tear (P = .03). Tears involving the nondominant arm were associated with an increased risk of failure by a factor of 3.04 (95% CI, 1.01-9.11; P = .047). A WORC score ≥80 was associated with a 95% probability of treatment success at 1 year.
Conclusion:
After arthroscopic rotator cuff repair, patients with WORC scores ≥80 at 1 year have a 95% probability of successful treatment and likely do not benefit from continued follow-up visits. Furthermore, several risk factors were identified that may influence outcomes after rotator cuff repair, including workers’ compensation, location of tear, tear size, and hand dominance.
Rotator cuff tendon tears are common injuries presenting with shoulder pain and dysfunction. A review of the literature found the total prevalence of rotator cuff tears to be 30.4% in cadaveric specimens and 38.9% in the ultrasound evaluation of asymptomatic individuals. 30 Arthroscopic rotator cuff repair is an increasingly frequent 11 and reliable treatment option for symptomatic rotator cuff tears, offering good to excellent results in both function and quality of life. 3,7,10 Markov decision modeling has also shown rotator cuff repair to be cost-effective for all ages and to produce net cost savings to society as compared with conservative treatment. 27
Failure of rotator cuff repair has been estimated to vary from 7% to >90% in the literature and contributes to increased utilization of health care resources and decreased patient satisfaction. 10,23 Furthermore, while studies have shown varying rates of improvement for those whose tears healed and for those whose did not, 6,12,15,17,34 some studies have shown that patients with recurrent tears can have few symptoms. 13,21,25,32 Consequently, the most important factor after arthroscopic rotator cuff repair is whether or not the patient’s symptoms warrant further surgical intervention. Recently, studies have sought to identify factors leading to inferior outcomes after rotator cuff repair. Patient age, tear characteristics, fatty infiltration, and smoking status are among the variables found to be associated with failure to heal and inferior clinical outcomes. 9,22,26,28
To date, no study has sought to correlate a patient-reported outcome score with the risk of treatment failure in arthroscopic rotator cuff repair. The aim of this study was to evaluate a validated patient-based outcome instrument, the Western Ontario Rotator Cuff (WORC) index 20 as a predictor of treatment success in arthroscopic rotator cuff repair. In addition, we sought to identify preoperative patient and tear characteristics that are associated with an increased risk of symptomatic treatment failure in this population of patients.
Methods
We performed a retrospective review of our database of patients who underwent arthroscopic rotator cuff repair at a single institution over a 4-year period (2009-2013). This database was established as a quality improvement initiative at our institution to capture patient outcomes after surgical interventions, including arthroscopic rotator cuff repair. All patients who undergo surgery are introduced to the program and free to enroll. Patient information is deidentified and stored on encrypted servers on-site. Patients are evaluated postoperatively and given regularly occurring outcome questionnaires. All operations were performed by 1 of 11 board-certified or board-eligible orthopaedic surgeons at a large ambulatory surgery center. An institutional review board approved the study proposal, and informed consent had been previously gathered at the time of database enrollment.
Our inclusion criteria included adult patients (>18 years old) with a primary rotator cuff tear treated with arthroscopic repair. Patients were excluded if they did not have a tear repaired, underwent conversion to open repair, failed to follow up for a minimum of 2 years postoperatively, or chose not to participate in our institution’s outcome database. It is our practice that all patients diagnosed with a rotator cuff tear are offered physical therapy as a first-line treatment, and if symptoms fail to respond to conservative management, surgical intervention is offered.
All participating patients who underwent arthroscopic rotator cuff repair during the collection period were asked to complete a WORC questionnaire prior to surgery to establish a baseline, preoperative score. Postoperatively, they were instructed to return for regular clinical follow-up as determined by the treating surgeon and to complete yearly WORC questionnaires. Records were retrospectively reviewed for demographic data, medical history, workers’ compensation status, and characteristics such as age, sex, hand dominance, body mass index, and smoking status. Intraoperative details were obtained from the standardized operative report, which allowed determination of tear size and additional findings or procedures performed. In addition to arthroscopic rotator cuff repair, patients underwent subacromial decompression, distal clavicle excision, biceps tenodesis or tenotomy, and/or labral debridement at the discretion of the treating surgeon.
Rotator cuff tears were characterized by tear size, defined as number of tendons involved, and taken from the intraoperative findings as recorded in the operative report. Magnetic resonance imaging (MRI) scans were reviewed to determine rotator cuff muscular atrophy.
All patients underwent similar rehabilitation at the discretion of the treating surgeon. Patients were placed in shoulder immobilizers for the first 6 weeks postoperatively. Physical therapy was typically performed at home, with an emphasis on regular pendulum/Codman exercises. After 6 weeks of immobilization, patients were started on formal outpatient physical therapy, which included passive motion initially with graduation to active motion and strengthening. Most patients returned to unrestricted activities after 12 weeks postoperatively.
Patients returned for regular postoperative follow-up visits and were evaluated by the treating physician. Clinical documentation from patient visits was reviewed and evaluated for treatment failure. The primary endpoint in this study was success or failure of the operative treatment. Treatment success was defined as a patient reporting good results in postoperative clinical documentation and not reporting symptoms to warrant further workup. Treatment failure was defined as a patient complaining of persistent or recurrent shoulder pain and/or weakness in clinical follow-up, leading to further workup and identification of a failure to heal or recurrent tear by MRI. Patients with symptoms but an intact rotator cuff by MRI were not classified as failures in this study. Rotator cuff integrity was not evaluated with advanced imaging in those patients reporting good results and without shoulder symptoms. The definition of treatment failure was chosen to identify those patients who would be candidates for revision arthroscopic rotator cuff repair. Those patients with treatment failures were treated nonoperatively with physical therapy and possibly steroid injections, or they underwent revision repair.
Continuous outcome variables were presented as medians ± 1 SD. All demographic data and tear characteristics were treated as independent variables, and logistic regression analyses were used to test the relationships among these variables and treatment failure. All multivariate analyses were adjusted for tear size and workers’ compensation. Kruskal-Wallis nonparametric tests were used to identify differences in WORC outcome scores across pre- and postoperative time intervals. Mann-Whitney tests were used to evaluate relationships among WORC scores, patient variables, and rotator tear characteristics across all time intervals. Odds ratios (ORs) and 95% CIs were calculated and reported to estimate effect size. WORC scores were compared between the treatment success and failure groups, and a logistic regression model was used to calculate the probability of clinical treatment failure based on WORC scores at 1 year. All statistical analyses were performed with Stata Statistical Software (v 14; StataCorp).
Results
A total of 500 patients were enrolled and completed a minimum of 2-year follow-up, with 68 (14%) completing 5-year follow up. During the study period, 1451 patients underwent arthroscopic rotator cuff repair at our institution and were eligible for enrollment but either chose not to enroll or failed to complete the minimum 2-year clinical follow-up. The demographics and relevant clinical data are presented in Table 1.
Demographic and Clinical Data of Patients and Rotator Cuff Tear Size a
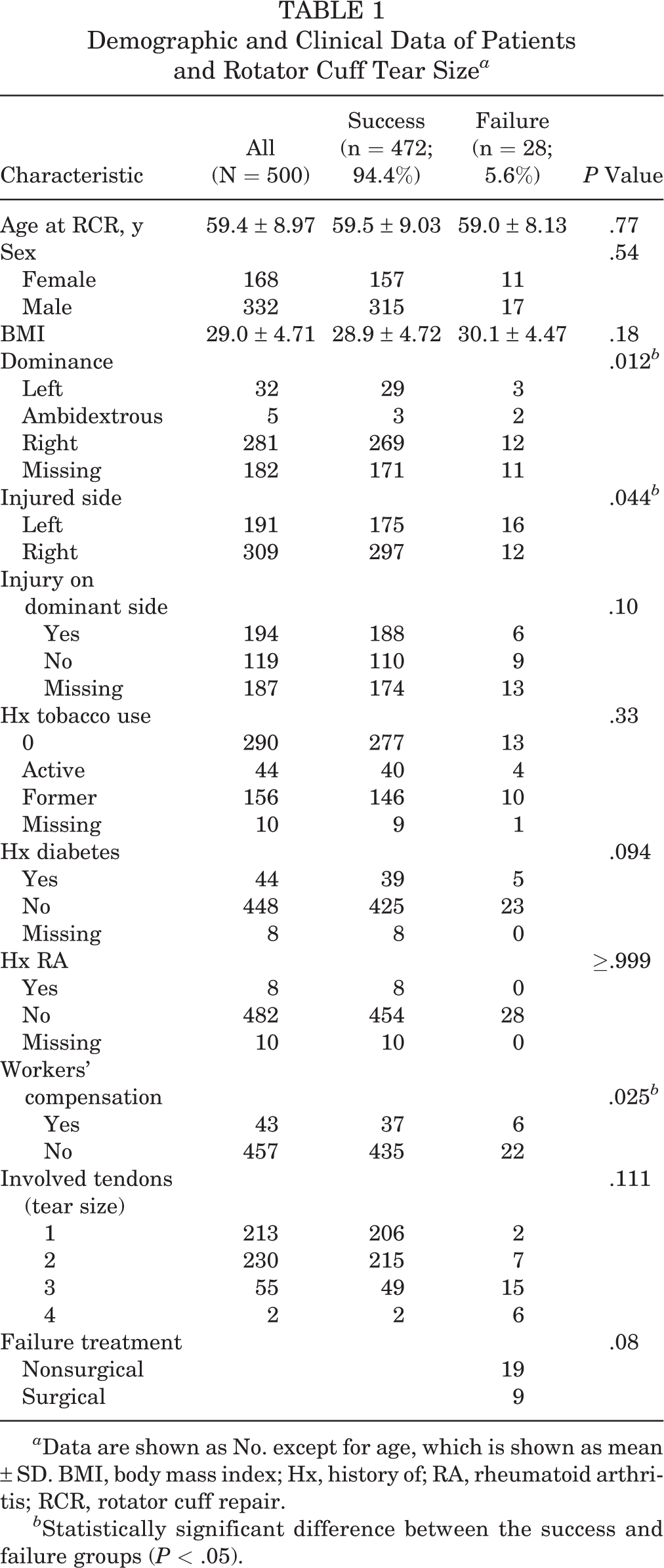
a Data are shown as No. except for age, which is shown as mean ± SD. BMI, body mass index; Hx, history of; RA, rheumatoid arthritis; RCR, rotator cuff repair.
b Statistically significant difference between the success and failure groups (P < .05).
There were 332 men and 168 women included in the study. The mean age of patients was 59 years at the time of surgery. Of those included in the study, 44 patients were diabetic; 190 patients had hyperlipidemia; and the mean body mass index was 29.0. The number of patients endorsing active or former tobacco use was 200. There were 43 (8.6%) patients claiming workers’ compensation. There were 281 right hand–dominant, 32 left hand-dominant, and 5 ambidextrous individuals; the remaining 182 patients had incomplete records. Of the 313 patients with complete records, 194 rotator cuff tears involved the patient’s dominant side.
There were 213 single-tendon tears, 230 two-tendon tears, 55 three-tendon tears, and 2 four-tendon tears. Muscular fatty infiltration was identified in 95 patients. In addition to arthroscopic rotator cuff repair, 460 patients underwent subacromial decompression; 104, distal clavicle excision; 311, biceps intervention; and 357, debridement of the labrum. The 311 biceps interventions included 89 (29%) debridements, 147 (47%) tenotomies, 56 (18%) arthroscopic tenodeses, and 19 (6.1%) open tenodeses.
At final follow-up, there were 28 treatment failures (5.6%) diagnosed at a median of 28 weeks (SD, 42) postoperatively. Nine (32%) patients in the treatment failure group underwent revision surgery, while the rest elected to not seek further surgical intervention. Risk factors associated by univariate analysis with treatment failure are shown in Table 2. Patients claiming workers’ compensation had an OR of 3.21 (OR, 3.21; 95% CI, 1.22-8.40; P = .018) of failing operative treatment. The odds of a treatment failure in tears involving the infraspinatus was 3.14 (OR, 3.14; 95% CI, 1.31-7.54; P = .01) as compared with those that did not involve the infraspinatus. Tear size was associated with treatment failure, and for each additional tendon involved, the odds of failure increased by a factor of e^[ln(1.80)] (OR, 1.80; 95% CI, 1.06-3.06; P = .03). The odds of a treatment failure was 3.24 for a 2-tendon tear and 5.83 for a 3-tendon tear. On multivariate analysis, tears involving the nondominant side were associated with an increased odds of failure (OR, 3.04; 95% CI, 1.01-9.11; P = .047) as compared with those involving the dominant side.
Results of Linear Regression Models Investigating Variables of Interest and Their Association With Treatment Outcome a
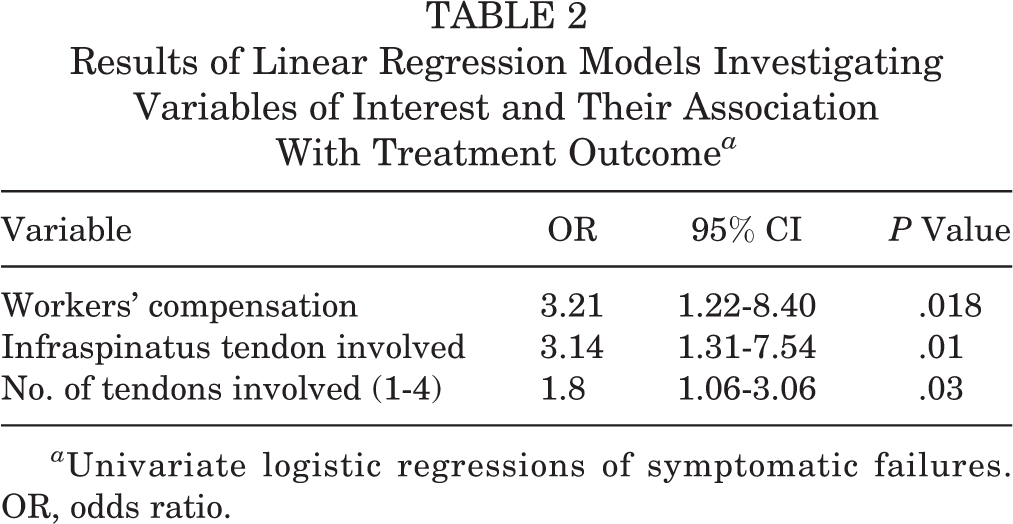
a Univariate logistic regressions of symptomatic failures. OR, odds ratio.
Patient-reported WORC scores are presented in Table 3. There were no significant differences in preoperative WORC scores when controlled for demographic variables, tear characteristics, and workers’ compensation status in patients who ultimately failed treatment versus those who did not. The treatment failure group did report significantly lower postoperative WORC scores than the treatment success group at 1- and 2-year follow-ups (P < .001) (Figure 1).
Total WORC Scores by Year for All Patients and by Treatment Success and Failure a

a WORC, Western Ontario Rotator Cuff index.
b Of the 500 patients, only 400 fully completed the WORC questionnaire preoperatively. 100 patients omitted 1-2 questions which makes the entire WORC questionnaire unusable.

Total WORC scores by postoperative year for all patients, those with treatment success, and those with treatment failure. There was a statistically significant difference between the success and failure groups at 1- and 2-year follow-ups (P < .001). Values are presented as median ± SD. WORC, Western Ontario Rotator Cuff index.
Overall, WORC scores increased significantly at postoperative 1 year as compared with preoperative scores (P < .001). Subsequent WORC scores at 2 years and 5 years were not statistically different from scores seen at 1 year. Interestingly, at 5 years of follow-up, the significant difference in WORC scores between the success and failure groups disappeared. Age older than 55 years, workers’ compensation, and tears that included the infraspinatus were all associated with decreased WORC outcome scores at baseline and postoperatively. According to logistic regression modeling, patients who had a WORC score ≥80 at postoperative 1 year demonstrated a ≤5% probability of treatment failure in the first 2 years (Figure 2). No WORC score threshold was found in the logistic regression models that confidently predicted a treatment failure, suggesting a low specificity for this instrument in identifying patients who will ultimately fail.

Linear regression model evaluating WORC score at 1 year as associated with probability of treatment failure. WORC, Western Ontario Rotator Cuff index.
Discussion
Arthroscopic rotator cuff repair offers patients a reliable means of symptomatic relief from pain and disability associated with rotator cuff tears. This study demonstrated a marked improvement in patient-reported outcomes by means of the WORC score. Median patient WORC scores improved from 41.1 preoperatively to 92.7 at 1 year postoperatively, and this improvement was maintained at 2 and 5 years postoperatively. Our study demonstrates favorable outcomes for arthroscopic rotator cuff repair, similar to prior peer-reviewed studies. 10,18,20,29 The strength of this study is the use of the patient-reported WORC score, which has been designed and validated to measure disability associated with rotator cuff tears. 20
The treatment failure rate after 2 years, as defined in our study, was 5.6% and represents the cohort of patients whose symptoms of pain and disability postoperatively led to further imaging and a diagnosis of failed rotator cuff integrity. As such, this methodology focuses on patients who may be candidates for revision surgery. This did not include asymptomatic tendon defects, which could be identified by advanced imaging and reported as a failure of tendon healing rate. We also did not capture patients who had significant symptoms (pain, stiffness, weakness) but an intact cuff on MRI. Recent literature estimates this rate of failure to be 5% to 57%, depending on the initial size of the rotator cuff tear. 4,23,35,36 It is important to note that this rate of failure does not reflect an expected failure of treatment, since a majority of these patients do not experience symptoms; therefore, from the perspective of patients, surgery is a success, and they would not be candidates for revision surgery based on the criteria of pain and dysfunction. The principal goal of surgery is improving symptoms and alleviating disability, and this outcome cannot be assessed by postoperative imaging but rather by patient-reported outcome.
The patients in our study who met the criteria of treatment failure had significantly worse WORC scores at 1 and 2 years postoperatively as compared with those deemed successful. While it is expected that patients who are doing well would score higher on the WORC and not seek further treatment as opposed to patients who fail treatment, our study is the first to offer a quantitative threshold to differentiate these groups. Logistic regression modeling revealed a WORC score of 80 to be the cutoff value. If a patient has a WORC score ≥80 at 1 year postoperatively, then the likelihood of treatment failure in the first 2 years is ≤5%. This cutoff offers the WORC as a clinically useful tool in the postoperative evaluation and surgical decision making of patients after arthroscopic rotator cuff repair. A patient with a WORC score ≥80 will have a ≤5% chance of demonstrating symptoms significant enough to be defined as a treatment failure with a corroborating imaging study and therefore to be a candidate for revision surgery. These patients would likely be served best with reassurance and physical therapy as opposed to further diagnostics. Interestingly, our analysis did not uncover a WORC score threshold associated with treatment failure, suggesting that this instrument may have poor specificity for identifying patients who fail treatment by our definition.
Posterior interval–based tears (ie, those rotator cuff tears that included the infraspinatus tendon) were associated with more poor outcomes and higher rates of treatment failure, with an OR of 3.14 (95% CI, 1.31-7.54; P = .01). This finding is consistent with previous reports that posterior tears represent a more chronic, degenerative variety of tear. Kim et al 19 reviewed ultrasonograms of 360 rotator cuff tears and found degenerative tears to most commonly arise from a posterior location between the supraspinatus and infraspinatus or wholly within the infraspinatus tendon. A cadaveric model by Araki et al 1 demonstrated anterior interval tears to more likely propagate at lower loads as compared with posterior tears, which offers a plausible biomechanical explanation for the disparity in chronicity of anterior versus posterior tears.
Additionally, hand dominance was found to affect the risk of treatment failure; this, to our knowledge, has not been previously reported. In our multivariate analysis, involvement of the nondominant arm was associated with a failure by a factor of 3.04 (OR; 95% CI, 1.01-9.11; P = .047). The reason for this is unclear but could be related to an activity and usage difference between the shoulders or to better neuromuscular coordination and preinjury conditioning in the dominant shoulder versus the nondominant shoulder. There is no literature on the topic for rotator cuff injuries; however, there are studies demonstrating limb dominance to modulate the risk of anterior cruciate ligament tears, with the nondominant leg having a higher risk of injury. 5,31
As demonstrated in previous studies, the size of the rotator cuff tear was associated with treatment failure. 8,10,14,24,33 In our multivariate analysis, the odds of treatment failure increased for each addition tendon involved. Two-tendon tears had an 3.24 odds of failure and 3-tendon tears, 5.83 odds. Other studies have reported the failure rates of rotator cuff repairs by tear size. Cho and Rhee 8 reported a failure to heal in 4.3% of small tears, 12.7% in medium tears, and 41.5% in large and massive tears. Gulotta et al, 14 in their review of 193 rotator cuff tears, reported the odds of a tendon defect on ultrasonogram to increase by 1.76 for every centimeter-in-length increase of the rotator cuff tear, and multitendon tears were 5.56 more likely to have a defect. However, the authors found no significant correlation between tendon healing and clinical outcomes. The strength of our analysis is a much larger cohort and a focus on patient-reported clinical outcome, with poor outcomes subsequently evaluated by advanced imaging.
Patients claiming workers’ compensation were found to present with symptomatic failures at a much higher rate than their counterparts, with an OR of 3.21 (95% CI, 1.22-8.40; P = .018). Their WORC scores were also markedly lower than those of patients not claiming workers’ compensation both before and after surgery, which is consistent with many other studies. 2,10,16
This study has several limitations. The most important is the accompanying limitations of a retrospective review of a prospectively collected database study. All eligible patients who were treated at our institution were invited to participate, and during this study period, 1451 patients underwent arthroscopic rotator cuff repair and were therefore eligible. Ultimately, 500 patients completed the 2-year follow-up, representing only 34.5% of the patient population treated during that time frame. We are unable to speculate whether the cohort of patients who did not participate or were lost prior to 2-year follow-up are doing better or more poorly than our study cohort, and this could have biased the results. We also recognize that we did not have complete data for some variables in our study group. This was especially notable for hand dominance, in which only 318 of our 500 patients had these data available. Routine postoperative imaging is not the standard of practice at our institution and so was not performed in the treatment success group. Additionally, our definition of success differs from other studies in the literature, and symptomatic patients with an intact rotator cuff tear were not included in our failure group.
Conclusion
The important contribution of this study is that we were able to determine that a postoperative WORC score ≥80 is associated with a ≤5% likelihood of treatment failure and need for revision surgery within the first 2 postoperative years. Furthermore, we saw that improvement in the WORC outcome score was notable at 1 year and did not markedly change in the years to follow, suggesting that the clinical utility of patient follow-up after 1 year is low. Known patient factors, such as workers’ compensation status and tear size, contributed to this risk, but so did hand dominance, which has not been described before. This information should aid surgeons by offering a WORC threshold of ≥80 at 1 year as a predictor of good long-term outcomes.
Footnotes
Acknowledgment
The authors thank Paul Lender for his contributions in data analysis and statistics.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the HealthPartners Institute Research Subjects Protection Program.