
Abstract
Background:
Rectus femoris injuries are common among athletes, especially in kicking sports such as soccer; however, proximal rectus femoris avulsions in athletes are a relatively rare entity.
Purpose/Hypothesis:
The purpose of this study was to describe and report the results of an original technique of surgical excision of the proximal tendon remnant followed by a muscular suture repair. Our hypothesis was that this technique limits the risk of recurrence in high-level athletes and allows for rapid recovery without loss of quadriceps strength.
Study Design:
Case series; Level of evidence, 4.
Methods:
Our retrospective series included 5 players aged 31.8 ± 3.9 years with acute proximal rectus femoris avulsion injuries who underwent a surgical resection of the proximal tendon between March 2012 and June 2014. Four of these players had recurrent rectus femoris injuries in the 9 months before surgery, while 1 player had surgery after a first injury. Mean follow-up was 18.2 ± 12.6 months, and minimum follow-up was 9 months. We analyzed the age, sex distribution, physical examination outcomes, type and mechanism of injury, diagnosis, treatment and complications during surgery, postoperative follow-up, and time to return to play. The Lower Extremity Functional Scale (LEFS) and Marx scores were obtained at 3-month follow-up, and isokinetic tests were performed before return to sports. A telephone interview was completed to determine the presence of recurrence at an average follow-up of 18.2 months.
Results:
At 3-month follow-up, all patients had Marx activity scores of 16 and LEFS scores of 80. Return to the previous level of play occurred at a mean of 15.8 ± 2.6 weeks after surgery, and none of the athletes suffered a recurrence. Isokinetic test results were comparable between both sides.
Conclusion:
The surgical treatment of proximal rectus femoris avulsions, consisting of resection of the tendinous part of the muscle, is a reliable and safe technique allowing a fast recovery in professional athletes.
Quadriceps muscle strains frequently occur in sports that require repetitive kicking and sprinting efforts. 4,5,7,14,17,18,24,27,34 Thigh strains, including hamstring and quadriceps muscles, have been reported as the most common injuries among professional soccer players. 18,19,34 Most muscle strains occur in response to eccentric loading, with the resultant injury occurring near the musculotendinous junction. 15,16
In the quadriceps muscle group, the rectus femoris crosses both the hip and knee joints and is therefore most often injured during eccentric loading. Indeed, the most common type of quadriceps injury is an intramuscular strain of the musculotendinous junction. 3 The direct head of the rectus femoris originates at the anterior inferior iliac spine, and the reflected head in the upper region of the acetabulum. Its tendon stretches from the distal third of the quadriceps muscle forming an extensive myotendinous structure down to the tendinous insertion at the upper pole of the patella. The incidence of rectus femoris tears in soccer players is less than 1%, and most frequently occur at the myotendinous junction. 20 In general, there is no consensus on an appropriate treatment for rectus femoris avulsions in high-level athletes.
We present an original surgical technique consisting of excision of the proximal tendon of the rectus femoris followed by a muscle-to-muscular suturing of the remnant belly. Our purpose was to describe and report the results of an original technique of surgical excision of the tendon remnant followed by a muscular suture repair. Our hypothesis was that this technique limits the risk of recurrence in high-level athletes and also permits a fast recovery with minimal loss of strength and the ability to return to the high demands in performance of professional soccer players.
Methods
We carried out a retrospective study of rectus femoris injuries in professional soccer players. We included in the study all the professional soccer players diagnosed with complete proximal rectus femoris tears who were operated on by our service between November 2012 and October 2014. All 5 players suffered an acute injury (<3 weeks), which occurred as sudden onset of pain while playing. All injuries were eccentric mechanisms. In the 9 months before surgical treatment, 4 of the 5 players had a minimum of 2 recurrent rectus femoris injuries, consisting of partial intrasubstance strain at the myotendinous proximal insertion. Despite conservative treatment, these players sustained a new complete avulsion injury, which was then treated by surgical excision. One player had surgical treatment after his first avulsion injury involving the 2 tendons.
We analyzed the age, sex distribution, physical examination, type and mechanism of injury, diagnosis, treatment and complications during surgery, postoperative follow-up, and time to return to play. Physical examination showed a retraction of the quadriceps muscle belly, which moved distally when contracted. A magnetic resonance imaging study of both tendons was performed in all cases to confirm the lesion (Figure 1). All patients, regardless of previous injury, were offered immediate surgical intervention. The mean (±SD) delay between injury and surgery was 9.8 ± 2.9 days. Conservative treatment was performed, consisting of rehabilitation with ice, stretching, manual therapies, and a graduated strengthening program for 2 weeks during the injury surgery delay.
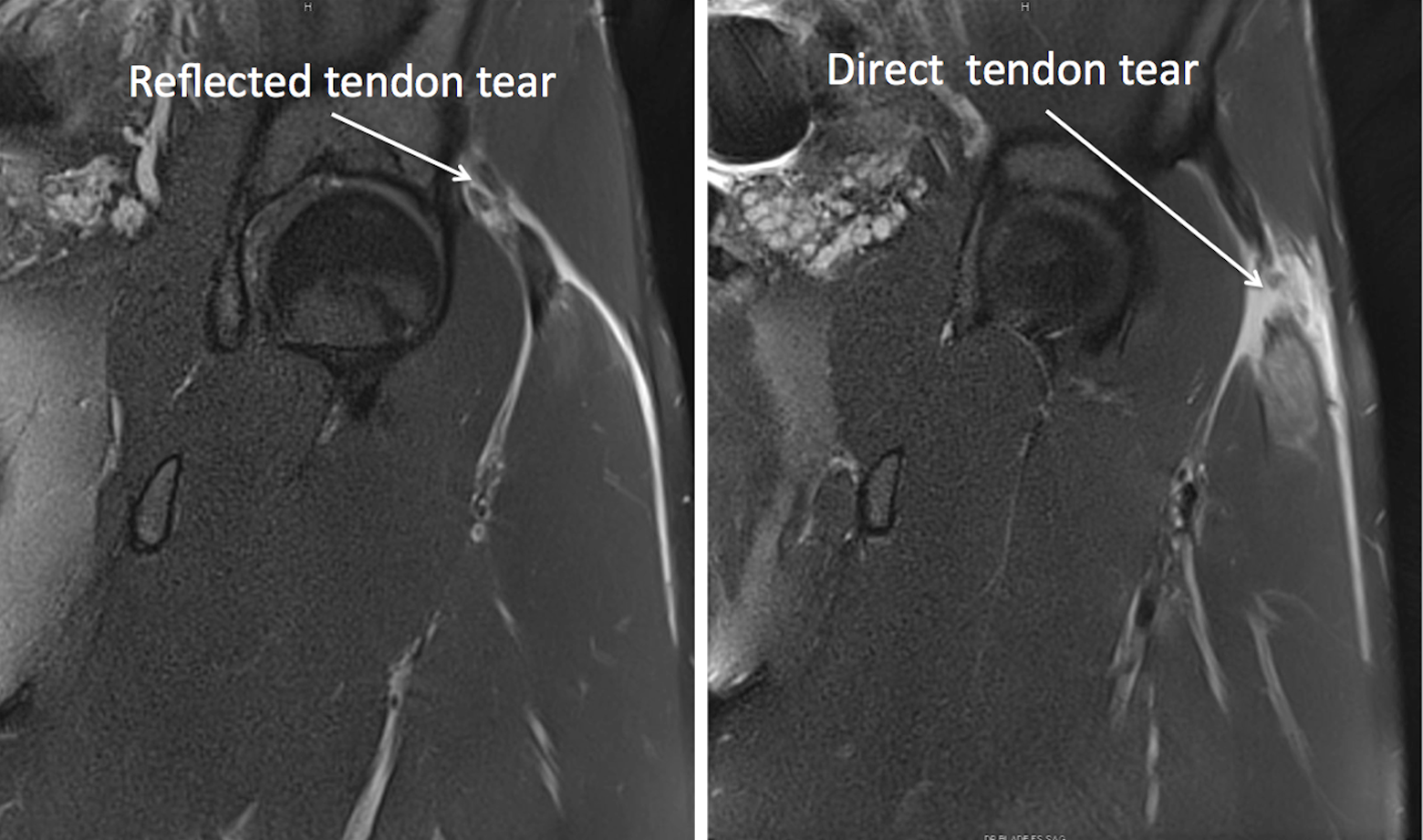
Magnetic resonance image demonstrating a reflected tendon tear and a direct tendon tear in the same patient.
Surgical Technique
We used the Hueter anterior approach sparing the tensor fascia lata. 11 With the patient in the supine position, the incision starts from the anterior superior iliac spine, and extends distally for 10 cm in line with the outer border of the patella, anterior to the tensor fascia lata muscle belly (Figure 2). The incision is completed lateral to the interval between the tensor fascia muscle and the sartorius to minimize the risk of a lateral femoral cutaneous nerve injury. By developing the interval within the tensor fascia, the lateral femoral cutaneous nerve remains medial to the sartorial fascia and is avoided in the superficial dissection. At this point, the proximal avulsion of the rectus femoris is visualized and the hematoma encountered. One must precisely identify the 2 parts of its tendinous insertion, namely, pars directa and reflecta (Figure 2). Excision of both the heads is then performed. The belly of the remnant muscle is sutured with resorbable sutures without tension to the surrounding muscle (vastus lateralis) in a side-to-side fashion. A suction drain is placed and the wound closed (see the Video Supplement).

(A) Anatomic landmarks for the Hueter anterior approach. (B) The tensor fascia lata (TFL) muscle is retracted laterally. (C) Reflected tendon and direct tendon identification. (D) Excised tendon.
Postoperative Rehabilitation Protocol
Immediate mobilization was allowed after surgery. Patients were on crutches for 2 weeks with weightbearing as tolerated. From weeks 2 to 6, a rehabilitation program was implemented based on progressive stretching of the quadriceps group, with active and passive range of motion. From weeks 6 to 10, muscular strengthening was implemented and progressed as tolerated. At 2 months, sport-specific training was implemented, and return to play was allowed when the patient was pain free and completed sport-specific training. At 3 months, isokinetic testing was performed for all patients to compare the quadriceps maximal concentric strength moment at 60° for the healthy and operated knee. The conventional ratio (concentric hamstring to concentric quadriceps) and the functional ratio (eccentric hamstring to concentric quadriceps) of the healthy and operated extremities were also investigated.
Follow-up
All 5 five patients were observed clinically until physician release for return to play. At 3 months postoperatively, Lower Extremity Functional Scale (LEFS) and Marx activity scale results were obtained.
4,25
The patients were subsequently contacted for telephone interview by an independent investigator with an average follow-up of 18.2 months (range, 8-32 months). As part of the questionnaire, 2 specific questions were asked: Have you had any recurrence of injury? Can you confirm how many months were required for you to return to your previous level of play after surgery?
Results
The mean age at surgery (±SD) was 31.8 ± 3.9 years. All patients suffered from avulsion of the proximal rectus femoris attachment.
Among the 5 professional soccer players, 3 were midfielders and the other 2 were strikers. All of them returned to their preinjury level of play and currently play with their corresponding Premiere League team. The mean time from surgery to return to play in competition was 15 ± 1.4 weeks (Table 1).
Patient Demographics

a Partial intrasubstance strain at the myotendinous proximal insertion.
At 3 months postoperatively, all athletes had a Marx activity rating of 16 of 16 and an LEFS score of 80 of 80. There was no recurrence of injury reported by any of the athletes. One hematoma occurred in the postoperative course in 1 player, and no other complications were encountered.
No deficit of strength was found in 2 players (players 2 and 3), low to moderate deficit of strength was found in 1 player (player 5), moderate to high deficit of strength was found in 2 players (players 1 and 4), as noted by the postoperative isokinetic test (Table 2).
Postoperative Isokinetic Test Interpretations

a Maximal concentric strength moment at 60 deg/s (hamstrings) divided by the maximal concentric strength moment at 60 deg/s (quadriceps).
b Maximal eccentric strength moment at 30 deg/s (hamstrings) divided by the maximal eccentric strength moment at 240 deg/s (quadriceps).
Discussion
The athletes in our study had an excellent clinical outcome as defined by both the Marx activity rating score and LEFS score. All 5 athletes returned to the previous level of play after surgical intervention in 15 ± 1.4 weeks. To our knowledge, this is the first study investigating the surgical treatment of excision of the proximal musculotendinous junction of the rectus femoris in professional soccer players.
Currently, there is no consensus on the management of such injuries with nonoperative treatment forming the corner stone and surgery being reserved for the nonresponders. 12,19 Gamradt and Brophy 12 reported a return to play in 69.2 days for 11 high-level National Football League athletes with rectus femoris avulsion treated conservatively. 12 Generally, muscle reinsertions are performed by suturing the tendon back to the bony attachment using anchors. 6,20,22,32 There is lack of clarity on the rate of recurrence after reattachment, with most studies reporting no recurrence in the operated patients. In 1 study, reattachment was performed in 4 of 10 professional athletes followed by a platelet-rich plasma (PRP) injection. 13 The authors reported a noteworthy quick return to sport at 3.8 months with surgical repair and PRP use. On the other hand, this result should be cautiously interpreted as long as use of PRP in skeletal muscle injuries is controversial. 1,8,28 Other authors have reported a return to sports between 5 and 10 months after surgical repair. 22,32 A tendon-bone reinsertion surgery may have disadvantages, as the healing of tendon to bone is a long and complex process leading to a histologically different enthesis than the natural one. Newsham-West et al, 26 in their study in 2007, demonstrated that the normal fibrocartilage layer at the enthesis is replaced by fibrous tissue after reattachment of tendon to bone. Various other studies have also shown that the surgical reattachment of tendon to bone often fails and presents difficulty in healing due to the failure of regeneration of this specialized fibrocartilage layer in an intra-articular model 2,31,33 as well as in an extra-articular environment. 10,23 Newsham-West et al 26 also noted that the healing of tendon to bone takes a long time and may be complete by approximately 2 years.
Four of our 5 cases had recurrent rectus femoris tears despite conservative treatment in the 9 months after the first injury. After surgery, all of them returned to play and none of them had a new injury at a minimum follow-up of 9 months. By resecting the remodeling tissue, the problem of chronic strain and inflammation affecting the remnant attachment is eliminated, whereas an intermuscular suture permits integral healing in a tension-free manner, thereby producing a strong repair. This can potentially decrease the chance of recurrence, which is of particular concern in professional athletes. Muscle-to-muscle suturing also heals faster than the healing at the enthesis.
Despite leading to moderate-high deficit of strength in 2 of 5 players, there was no impairment on return to play to elite professional soccer. We propose a treatment algorithm based on our experience including 2 treatment options: conservative treatment and surgical resection (Figure 3). In our experience, we have observed a higher recurrence rate of muscles injuries in professionals than in amateur athletes.
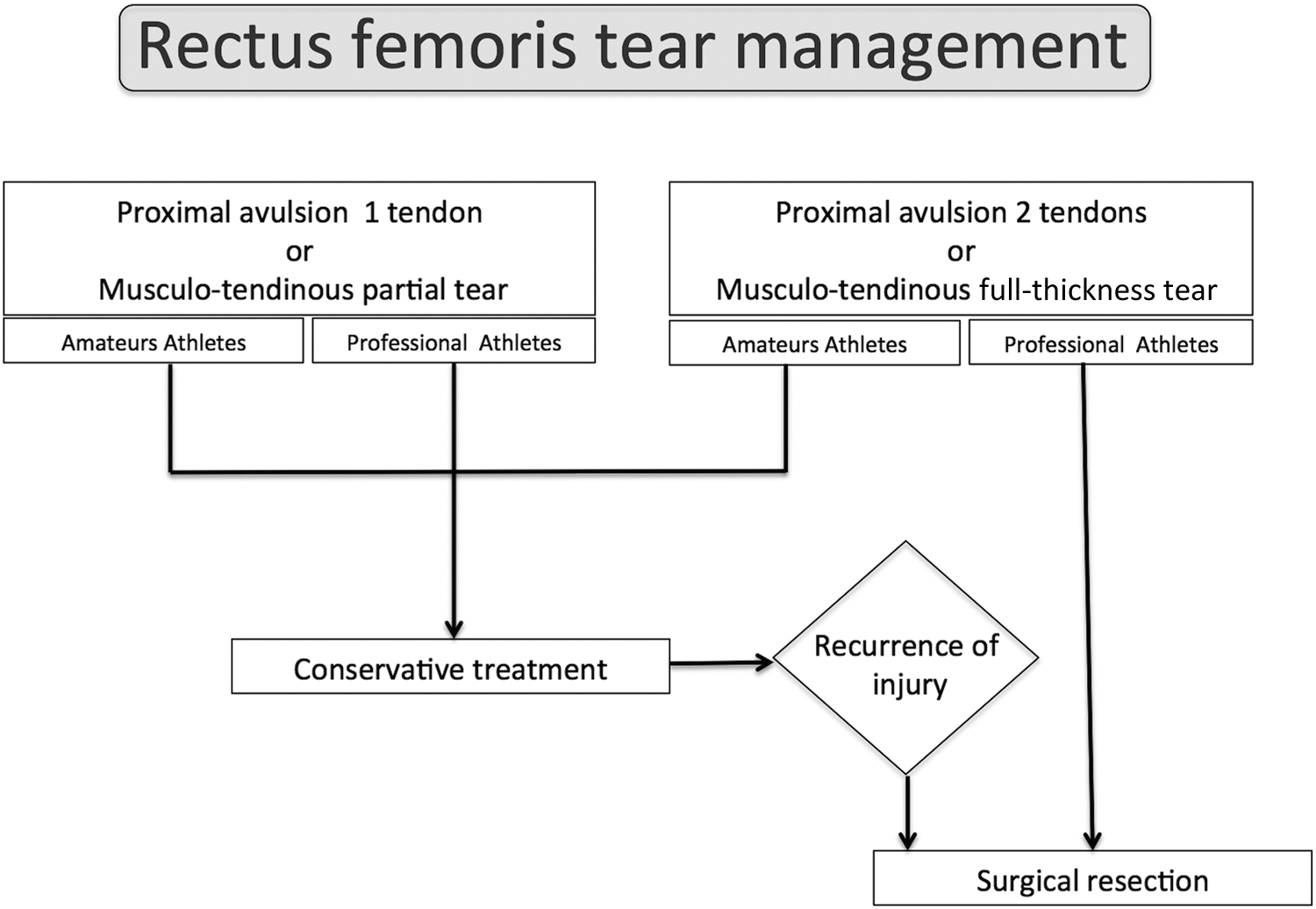
Treatment algorithm.
Avulsions of the direct head of the rectus femoris are well documented, but injuries of the reflected head are not mentioned in literature. We believe that the solitary remnant attachment of the rectus femoris may be subjected to excessive forces, especially during highly demanding sporting activities, causing persistent pain and recurrence of injuries. In addition, proximal or distal avulsions of the rectus femoris with retraction are commonly seen in the clinics as bulging on performing an active muscle contraction. Most of these patients have no complaints, therefore reattachment of the tendon may not be necessary as it will prolong the recovery time compared with excision and side-to-side suturing. In our experience, this technique is safe with no complications, permitting early and successful return to preinjury level of play.
The quadriceps tendon is formed by the confluence of individual tendons of 4 muscles inserting onto the superior pole of the patella. In fact, the rectus femoris head plays a minor role in the overall function of the thigh muscle group. Consequently, the quadriceps maintains good function even after the excision of the proximal attachment.
9
This can be explained by 1 of 2 mechanisms: The functional overload of an injured muscle’s synergists may cause compensatory hypertrophy of the remaining quadriceps muscles.
29,30
A lateral force transmission through the connective tissues within and surrounding the injured but neurologically intact rectus femoris muscle may contribute to the total force on the quadriceps tendon.
21
Our study has some weaknesses. We have no comparative group with a short follow-up and only a few cases. We also do not know the exact mechanism of the injury. Nevertheless, our treatment is the first to demonstrate a successful surgical intervention without recurrence and full return to play. In addition, all patients completed sport-specific training regimens and were asymptomatic before being released.
Conclusion
The surgical treatment of proximal rectus femoris avulsions, consisting of resection of the tendon, is a reliable and safe technique in professional athletes. Our results are encouraging given that all of our patients returned rapidly to professional soccer competition without recurrence after a long follow-up. Further investigation is needed to confirm these initial findings.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S-C. is consultant for and receives royalties from Arthrex. M.T. is consultant for Arthrex.
Ethical approval for this study was obtained from The Institutional Review Board of the ethical committee of the Hopital Privé Jean Mermoz and the Centre Orthopédique Santy (Ref. Study 2015-19).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.