
Abstract
Background:
A proximal rectus femoris (PRF) avulsion is primarily seen among elite-level athletes, which may require surgery after failed nonoperative treatment. Although suture bridge repair is a common surgical technique to treat these injuries, it is unclear whether a knotted or knotless suture bridge construct is biomechanically superior.
Purpose:
To biomechanically compare the failure load, stiffness, and number of cycles until failure of knotted versus knotless suture bridge repair for PRF avulsions.
Study Design:
Controlled laboratory study.
Methods:
A total of 8 pairs of fresh-frozen human cadaveric hemipelvises were included in this study. The PRF was harvested, along with its bony insertion at the anterior inferior iliac spine. Specimens underwent nondestructive testing in the intact state to assess linear stiffness. Each pair of specimens was randomly assigned to undergo knotted or knotless suture bridge repair. After surgical repair, the specimens underwent biomechanical testing consisting of a preconditioning phase, followed by pull to failure to assess the failure load, elongation at failure, stiffness, and mode of failure.
Results:
There was no difference in the failure load between knotless and knotted suture bridge repair (244 ± 124 vs 241 ± 136 N, respectively; P = .97). Elongation at failure was lower with the knotless construct compared with the knotted construct (19.7 ± 10.8 vs 34.3 ± 6.3 mm, respectively; P = .02). The most common mode of failure was suture anchor pullout. Intact stiffness was not significantly different between the knotless and knotted groups (56.0 ± 14.7 vs 57.4 ± 19.5 N/mm, respectively; P = .99). Repair stiffness of the knotless group was not significantly different from the intact state (50.9 ± 12.6 vs 56.0 ± 14.7 N/mm, respectively; P = .79). The knotted group exhibited significantly lower repair stiffness compared with the intact state (38.3 ± 19.0 vs 57.4 ± 19.5 N/mm, respectively; P = .01). The knotless group demonstrated significantly higher stiffness as a percentage of the intact state compared with the knotted group (93.7% ± 21.1% vs 65.0% ± 22.1%, respectively; P = .03).
Conclusion:
This study demonstrated that the failure load between knotless and knotted suture bridge repair was not significantly different. However, stiffness as a percentage of the intact state in the knotless group was significantly higher than that in the knotted group. Therefore, this study suggests that the knotless suture bridge repair technique may be a better surgical option than the knotted suture bridge repair technique to restore stiffness of the PRF.
Clinical Relevance:
Elucidating a biomechanically superior repair method for PRF avulsions may inform optimal surgical techniques for treating these injuries, leading to lower failure rates and superior outcomes in patients.
A proximal rectus femoris (PRF) avulsion is a relatively rare injury, mainly observed in high-level athletes participating in sports that involve repetitive kicking and sprinting (accounting for <0.5%-1.5% of hip injuries in athletes).2,8,14 The surgical indication for PRF repair has been reported for high-level athletes with both tendons avulsed or full-thickness tears after failed nonoperative treatment. 23 Suture bridge repair and tenodesis have been the 2 common repair techniques for PRF avulsions.7,10,12,23 A previous biomechanical study investigated the biomechanical strength of suture bridge repair versus tenodesis. 17 The findings of that study indicated that suture bridge repair exhibited superior biomechanical strength compared with tenodesis.
To optimize suture bridge techniques, biomechanical studies have been published comparing knotted and knotless suture bridge constructs for rotator cuff repair and Achilles tendon repair.1,4,6,15 However, there is no study that has compared the biomechanical strength of knotted versus knotless suture bridge repair of the PRF. Of note, a previous study reported that knotted repair had a higher risk of retears compared with knotless repair for rotator cuff tears. 21 Most biomechanical studies found that knotted suture bridge techniques showed better initial strength, with higher failure loads, compared with knotless suture bridge techniques in the setting of rotator cuff repair.4-6,11,25 However, some studies found no significant difference in the failure load and stiffness between the 2 methods.15,16,19 Consequently, the biomechanical superiority between knotted and knotless suture bridge techniques remains controversial.
The objective of this study was to compare failure characteristics among 3 PRF tendon conditions: intact tendon, knotted suture bridge repair, and knotless suture bridge repair. We hypothesized that knotted suture bridge repair would result in a higher failure load, stiffness, and number of cycles until failure compared with knotless suture bridge repair. This investigation aimed to shed light on the biomechanical aspects of the different repair techniques, ultimately contributing valuable insights to guide optimal treatment decisions for PRF injuries.
Methods
Specimen Preparation
A total of 8 pairs of fresh-frozen human cadaveric hemipelvises (16 specimens total; mean age, 44.4 years [range, 27-62 years]; 5 male and 3 female) with no evidence of a previous injury or abnormality were acquired. A priori power analysis (G*Power Version 3.1) based on data from a previous study indicated that a sample size of 8 pairs (mean difference, 121.7; standard deviation of difference, 80.7; power, 0.8) was required to perform a paired t test. 9 The specimens had been donated to a tissue bank for medical research and were purchased by our institution. Institutional review board approval was unnecessary because tissue was donated for research use, no genetic information was used, and no contact was made with the donor's family. Specimens were excluded for previous known injuries or surgery to the pelvis, a history of osteoporosis, and age >65 years.
The specimens were thawed for 24 hours before dissection and testing. The specimens were placed in a supine position, and exposure of the rectus femoris was achieved using an open approach. The rectus femoris was followed proximally to its origin in the anterior inferior iliac spine (AIIS). A bone block, including the AIIS with the rectus femoris attached, was harvested from the iliac bone using a bone saw. Dissected specimens were stored at −20°C until the day before testing. The posterior half of the iliac wing was potted in a custom-made cylindrical mold using polymethyl methacrylate (Fricke Dental).
Biomechanical Testing of Intact State
The region of the tendon to be fixed during testing was supported with a wrap and sutures to minimize damage from clamping to the specimen. The potted iliac wing was secured within a custom fixture that was attached to the base of a dynamic tensile testing system (ElectroPuls E10000; Instron), and the musculotendinous portion of the rectus femoris was fixed to the end effector of the testing machine via a custom clamp (Figure 1). Specimens were clamped between 3 and 7 cm distal to the anterior superior iliac spine enthesis. Pilot testing was performed to verify that slippage at the clamps did not occur when loads exceeding 300 N of tension were applied. The applied loading direction was configured such that an inferior shear force was applied between the rectus femoris enthesis and the anterior superior iliac spine.

Biomechanical testing setup. (A) Front view and (B) side view of the biomechanical testing setup are shown. The potted anterior superior iliac spine was secured to the base of the dynamic tensile testing system, and the proximal rectus femoris was fixed within a clamp that was attached to the end effector of the dynamic tensile testing system.
Initially, all specimens underwent nondestructive testing in the intact state. Specimens were preconditioned with a 0.5-Hz cyclic loading protocol from 25 to 100 N of tension over 50 cycles. The specimen was then pulled to 20 mm of displacement at 1 mm/s. After intact testing, the tendon was removed from the AIIS using a surgical scalpel (No. 15 blade) in preparation for treatment.
Surgical Techniques
Each pair of specimens was randomly assigned to 2 treatment groups. One specimen of the pair was treated with knotted suture bridge repair, and the other specimen of the pair was treated with knotless suture bridge repair. The knotted and knotless suture bridge techniques in the present study were performed following the techniques in previous studies.6,7,23 All surgical procedures were performed by a fellowship-trained orthopaedic surgeon (H.N.). Images of the surgical procedure are shown in Figure 2.
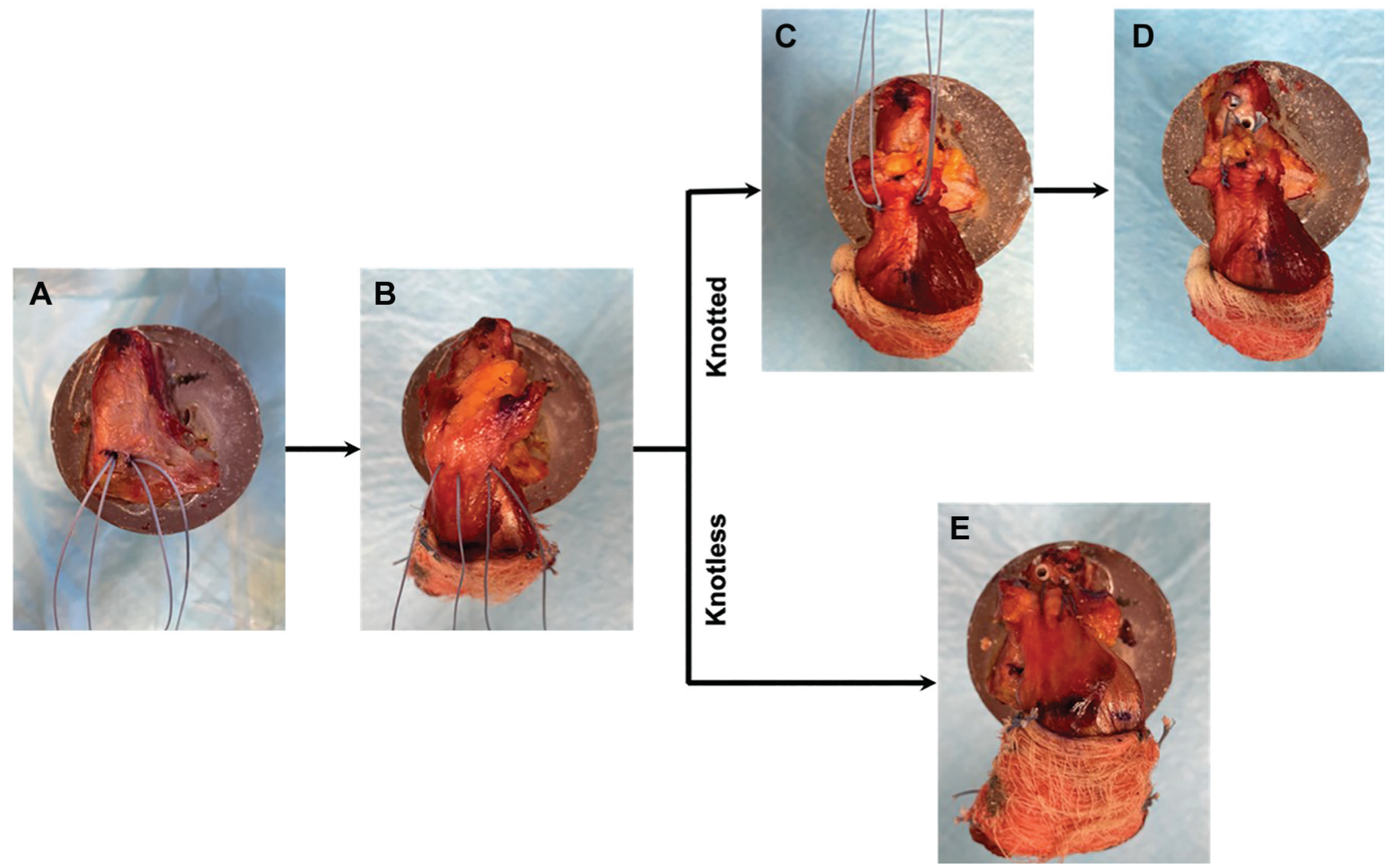
Surgical procedure. (A) Overall, 2 single-loaded suture anchors were placed 10 mm apart at the distal site of the anterior inferior iliac spine (AIIS). (B) The sutures from each anchor were threaded through the proximal rectus femoris tendon in a horizontal mattress fashion about 10 mm distal to the proximal end of the tendon. (C) For the knotted suture bridge technique, the sutures were tied with 4 knots. (D) One limb of the suture from each previously placed anchor was threaded through the eyelet of a knotless anchor, and then, the knotless anchor was placed at the proximal site of the AIIS to create the suture bridge. (E) For the knotless suture bridge technique, the suture bridge was created without knot tying.
For the knotted suture bridge technique, 2 single-loaded suture anchors (BioComposite SutureTak [2.4 × 12 mm] with No. 2 FiberWire; Arthrex) were placed 10 mm apart at the distal site of the AIIS, and the sutures from each anchor were threaded through the PRF tendon in a horizontal mattress fashion about 10 mm distal to the proximal end of the tendon. The rectus femoris tendon was tensioned to the bone at its approximated intact footprint with 4 hand-tied knots, leaving the free ends of the suture intact. One limb of the suture from each previously placed anchor was threaded through the eyelet of a knotless anchor. The knotless anchor (BioComposite SwiveLock [4.75 × 19.1 mm]; Arthrex) was placed at the proximal site of the AIIS. The same process was repeated for the remaining sutures using one more knotless anchor.
For the knotless suture bridge technique, 2 single-loaded suture anchors (BioComposite SutureTak [2.4 × 12 mm] with No. 2 FiberWire) were positioned and placed in a fashion identical to that used for the knotted suture bridge technique. The 2 tails of the suture attached to each anchor were threaded through a common perforation in the rectus femoris tendon about 10 mm from the proximal end of the tendon. Without tying any knots, one strand of the suture from each anchor was threaded through a knotless anchor (BioComposite SwiveLock [4.75 × 19.1 mm]) and placed at the proximal site of the AIIS. The same process was repeated for the remaining sutures using one more knotless anchor.
Biomechanical Testing of Repair State
Specimens underwent testing through a sequence of cyclic loads representative of a progressive postoperative rehabilitation protocol. A previous study reported an average maximum net force on the rectus femoris during walking to be approximately 500 N. 13 Recognizing the time-zero nature of the study, a 0.5-Hz cyclic loading protocol was applied to the specimen from 25 N to the maximum load in increments of 75 N every 50 cycles. If the specimen did not fail after reaching 325 N, the specimen was then pulled at 1 mm/s to failure. A maximum load of 325 N, which is 65% of the in vivo rectus femoris load of 500 N, was selected to account for reduced time-zero loading seen in the clinic. 13 The failure load, elongation at failure, stiffness, and mode of failure were recorded for each specimen. Linear stiffness was calculated from the linear portion of the resulting force-displacement curve, and stiffness as a percentage of the intact state was calculated for both repair groups.
Statistical Analysis
Statistical analyses were performed using MATLAB (MathWorks), and data were expressed as means ± standard deviations. The normal distribution of failure load, elongation at failure, and stiffness data was verified using the Shapiro-Wilk test. Paired t tests were used to compare failure load and elongation at failure between the repair groups. Stiffness data were compared between repair groups as well as between the repair state and the intact state within each repair group using paired t tests. Statistical significance was defined as P < .05.
Results
Failure
Failure load and mode of failure of the repair groups are reported in Table 1. The failure load of the knotless suture bridge repair group (244 ± 124 N) was not significantly different than that of the knotted suture bridge repair group (241 ± 136 N) (P = .97) (Figure 3). Elongation at failure of the knotless group (19.7 ± 10.8 mm) was significantly lower than that of the knotted group (34.3 ± 6.3 mm) (P = .0154) (Figure 3).
Failure Load and Mode of Failure


Failure load (left) and elongation at failure (right) for the knotless suture bridge repair group and the knotted suture bridge repair group. Data are presented as means and standard deviation bars. Statistical significance was defined as P < .05.
No specimens failed at the clamp. All specimens in the knotless group failed via SutureTak anchor pullout. In the knotted group, 6 specimens (75%) failed via SutureTak anchor pullout, and 2 specimens (25%) failed via SwiveLock and SutureTak anchor pullout (Table 1).
Stiffness
Data for intact and repair stiffness of both groups are reported in Table 2. Intact stiffness of the knotless suture bridge repair group (56.0 ± 14.7 N/mm) was not significantly different than intact stiffness of the knotted suture bridge repair group (57.4 ± 19.5 N/mm) (P = .994). Repair stiffness of the knotless group (50.9 ± 12.6 N/mm) was not significantly different than intact stiffness of the knotless group (56.0 ± 14.7 N/mm) (P = .791). Repair stiffness of the knotted group (38.3 ± 19.0 N/mm) was significantly lower than intact stiffness of the knotted group (57.4 ± 19.5 N/mm) (P = .0096) (Figure 4). Stiffness as a percentage of the intact state of the knotless group (93.7% ± 21.1%) was significantly higher than that of the knotted group (65.0% ± 22.1%) (P = .0264) (Figure 5).
Stiffness


Stiffness of the intact and repair states for the knotless suture bridge repair group (left) and the knotted suture bridge repair group (right). Black lines indicate that the groups are significantly different to each other. Data are presented as means and standard deviation bars. Statistical significance was defined as P < .05.

Stiffness as a percentage of the intact state for the knotless suture bridge repair group (left) and the knotted suture bridge repair group (right). Black lines indicate that the groups are significantly different to each other. Data are presented as means and standard deviation bars. Statistical significance was defined as P < .05.
Discussion
This study demonstrated that the failure load of the knotless suture bridge repair group was not significantly different to that of the knotted suture bridge repair group. However, elongation at failure of the knotless suture bridge repair group was significantly smaller compared with that of the knotted suture bridge repair group. In addition, stiffness as a percentage of the intact state in the knotless suture bridge repair group was significantly higher than that in the knotted suture bridge repair group. The results of this study suggest the biomechanical superiority of the knotless suture bridge technique in terms of restoring stiffness of the PRF.
Comparisons of the results observed in this study to results in the literature are mixed. Among the biomechanical studies that have investigated the biomechanical properties of the knotted versus knotless suture bridge technique, the majority reported that the knotted suture bridge technique displayed superior time-zero biomechanical properties, including a greater ultimate load to failure, compared with the knotless suture bridge technique.4-6,11,25 Other studies, however, reported no significant difference in maximum failure load and stiffness between the knotted and knotless techniques in the context of rotator cuff repair.15,16,19 Furthermore, one previous study reported that the knotless technique for rotator cuff repair showed significantly higher stiffness compared with the knotted technique for rotator cuff repair, which supports our result. 19 Conversely, 2 previous studies showed the opposite result, reporting the knotted construct as having higher stiffness than the knotless construct.5,11
Biomechanical outcomes are largely a function of an effective repaired footprint. Although the present study did not evaluate the footprint contact characteristics for PRF repair, previous biomechanical studies regarding rotator cuff repair reported that the knotless suture bridge technique had an improved self-reinforcement effect, without diminishing footprint contact, compared with the knotted suture bridge technique.18,22 These studies explained that medial knots do not improve footprint contact but lead to tenodesis during rotator cuff repair, thus stress shielding the lateral tendon from self-reinforcement and concentrating the stress at the medial row; thus, the tendon load is not as readily transmitted and converted to a tendon compressive force over the repaired footprint. The authors concluded that medial knots are not always biomechanically advantageous.
The results observed in the current study are largely in agreement with results from clinical outcome studies. Prasathaporn et al 20 reported that there was no significant difference in the overall retear rate between the knotless and knotted suture bridge techniques for rotator cuff repair, and both techniques demonstrated similar clinical outcomes. However, their results showed that the type 2 (failure at the musculotendinous junction with a healed footprint) retear rate was significantly greater after knot-tying repair and that the type 1 (failure at the tendon-bone interface) retear rate was significantly greater after knotless repair. 20 Xiao et al 26 reported that the clinical outcomes (retears, shoulder function score, shoulder mobility, and pain) of arthroscopic rotator cuff repair with the suture bridge technique with or without a knotted medial row were equivalent. Sundaram et al 24 reported no statistically significant difference in functional outcomes (Constant score; University of California, Los Angeles score; and American Shoulder and Elbow Surgeons score) between knotted and knotless transosseous double-row techniques for arthroscopic rotator cuff repair.
While biomechanical and clinical outcomes are mixed in comparing knotted versus knotless repair, previous literature has reported differences in operating cost and time between the 2 repair methods. Burns et al 3 conducted a study to determine the cost-effectiveness of the knotted versus knotless suture bridge technique for rotator cuff repair. Their results showed a statistically significant difference in the median implant cost, with the knotless group having a higher cost than the knotted group. They found that more anchors were used in the knotless group, with the knotted group requiring a median of 4 anchors and the knotless group requiring a median of 5 anchors. The procedure time was cut in half with knotless repair (43.5 minutes) versus knotted repair (80 minutes). The operating room time also was reduced by approximately 40% (79.5 minutes for knotless and 121 minutes for knotted). Once operating room costs were considered, the median cost was found to be significantly lower in the knotless group. No statistically significant differences were found between the groups in terms of clinical outcomes (visual analog scale; Simple Shoulder Test; American Shoulder and Elbow Surgeons score; and University of California, Los Angeles score). Thus, they concluded that the knotless technique for rotator cuff repair required less procedure time and cost less overall than the knotted technique and resulted in equivalent clinical outcomes. 3 However, that was a study regarding rotator cuff repair, and there is no such study available regarding PRF repair.
Limitations
This study has several limitations that could have potentially affected the conclusions of this investigation. The use of cadaveric specimens could potentially alter the quality of biological bone and tendon tissue. The age of the specimens was relatively higher than that of patients who usually suffer from a PRF injury. Therefore, the quality of the rectus femoris in cadaveric specimens may not be representative of muscle quality in vivo. Moreover, the biological effects of healing and the physiological effects of loading on the repair site are unknown because this study was performed at time zero, immediately after surgical repair, when the healing process had not occurred. In addition, because the footprint of the AIIS was small and the area in which a suture anchor could be inserted was limited, a slightly smaller anchor was used as the distal anchor. As a result, the mode of failure was pullout of the distal anchors in almost all specimens. A further study using different combinations of suture anchors should be conducted in the future.
Conclusion
This study demonstrated that the failure load between knotless and knotted suture bridge repair was not significantly different. However, stiffness as a percentage of the intact state in the knotless group was significantly higher than that in the knotted group. Therefore, this study suggests that the knotless suture bridge technique may be a better surgical option than the knotted suture bridge technique to restore stiffness of the PRF.
Footnotes
Final revision submitted November 11, 2024; accepted December 16, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Surgical supplies were donated by Arthrex. S.U. is a consultant for Smith & Nephew and ConMed Linvatec. M.J.P. has received royalties from Smith & Nephew, Arthrosurface, Bledsoe, ConMed Linvatec, DJO, SLACK, and Elsevier; is an owner/shareholder in Arthrosurface, MJP Innovations, Vail Valley Surgery Center, and Vail MSO Holdings; is a shareholder in MIS, EffRx Pharmaceuticals, Olatec, iBalance (Arthrex), Manna Tree Partners, Stryker, Trimble, 3M, Bristol Myers Squibb, Pfizer, AbbVie, and Johnson & Johnson; is a board member of the International Society for Hip Arthroscopy and Vail Health Services; is cochairman of the Steadman Philippon Research Institute; has received educational support from Smith & Nephew, ConMed Linvatec, Ossur, Arthrex, and Siemens Medical Solutions; has received speaking fees and consulting fees from Smith & Nephew, MIS, Olatec, and NICE Recovery Systems; and has received hospitality payments from Siemens Medical Solutions and Synthes. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.