
Abstract
Background
Mental health significantly impacts antiretroviral treatment (ART) adherence in adolescents and young adults with perinatal HIV (AYA-PHIV), posing challenges for healthcare providers. This study investigated the effects of music and counseling programs on mental health and treatment adherence of AYA-PHIV.
Methods
In a randomized controlled study, the participants were assigned to the Music and Counseling Program (Arm 1), the Music Program (Arm 2), the Counseling Program (Arm 3), and a no-intervention group (Arm 4). Before and after 10 weekly sessions of a 90-minute study intervention, ART adherence and mental health questionnaires were completed.
Results
After the intervention, Arm 1 participants had a significantly increased median self-esteem score (17-25, P = .05). A significantly decrease in mean Thai-IHSS scores were observed in Arm 1 and 3 participants.
Conclusions
The study demonstrated that music and counseling programs improved self-esteem and reduced internalized HIV-related stigma in AYA-PHIV. Most participants reported better ART adherence and improved virologic outcomes.
Introduction
In 2023, there were ∼1.01 million adolescents aged 15 to 19 years living with HIV globally. 1 Meanwhile, ∼25 643 adolescents and young adults living with HIV (AYA-PHIV) in Thailand were aged between 15 and 24 years. 2 Adolescence is a critical period marked by cognitive and emotional changes, increasing vulnerability to mental health challenges, particularly for those living with HIV. Mental health conditions such as depression and anxiety, compounded by social stigma, can significantly impact antiretroviral treatment (ART) adherence and overall well-being of AYA-PHIV.3–5
AYA-PHIV are at higher risk for depression, anxiety, and other mental health problems due to some factors, including social support and stigma. 6 HIV-related stigma could also have a negative impact on their mental health, social support, and ART adherence, 7 which placed them at risk for developing HIV drug-resistance and unfavorable treatment outcomes. 8
Several interventions, including education programs, counseling, and enhancing social support from peers, family members, and healthcare professionals, were reported as associated with improving adherence to ART in AYA-PHIV.9,10 Effects of stigma reduction interventions, 11 mental health screening, 12 and self-esteem enhancing interventions 13 on ART adherence were also reported. 14 Addressing psychosocial stressors among Thai AYA-PHIV while providing HIV care is critical (Chantaratin et al, 2022). 15
According to a systematic review and metaanalysis, music therapy was associated with a significant improvement in ART adherence and a reduction in depression and anxiety symptoms in people living with HIV/AIDS. Music therapy was proposed as a possible adjunct to standard ART care in promoting better treatment adherence and mental health outcomes for people living with HIV/AIDS. 16 However, its effects in AYA-PHIV remain obscure. This study aimed to evaluate the efficacy of an integrated music and counseling intervention on mental health and ART adherence of AYA-PHIV with virologic nonsuppression.
Methods
Study Design and Participants
This randomized controlled trial was conducted in Chiang Mai, Thailand, from July 2023 to June 2024. AYA-PHIV were recruited from HIV clinics in Chiang Mai and neighboring provinces. Potential participants were informed about the study and invited to participate. Those who were interested in joining underwent an informed consent process. Inclusion criteria were (1) aged between 15 and 24 years, (2) documented perinatal HIV infection, (3) receiving dolutegravir-based ART regimens at enrollment, (4) had HIV-1 RNA > 50 copies/mL within 1-year prior to enrollment, and (5) having mild to moderate mental health scores (defined as Depression Anxiety Stress Scale (DASS-21) test results from 5 to 10 for depression, from 4 to 7 for Anxiety, from 8 to 12 for Stress, or self-esteem scores ≤20, or Thai Internalized HIV-related Stigma Scale (Thai-IHSS) scores ≥10). Exclusion criteria were (1) documented or suspected major psychological problems as determined by the investigator based on available medical records, (2) having severe or higher mental health scores at screening (the DASS-21 test score ≥ 11 for depression, ≥ 8 for anxiety, or ≥ 13 for stress), (3) having other clinically significant diseases that could interfere with the study participation, and (4) having any other condition or social circumstances that would make study participation unsafe, or complicate study outcome interpretation. Stratified random sampling was used in this study. At enrollment, participants were stratified into four study arms based on age, sex, HIV-1 RNA levels, and mental health scores (Figure 1).

CONSORT 2025 flow diagram, flow diagram of the progress through the phases of a randomized trial of four groups (ie, enrolment, intervention allocation, follow-up, and data analysis).
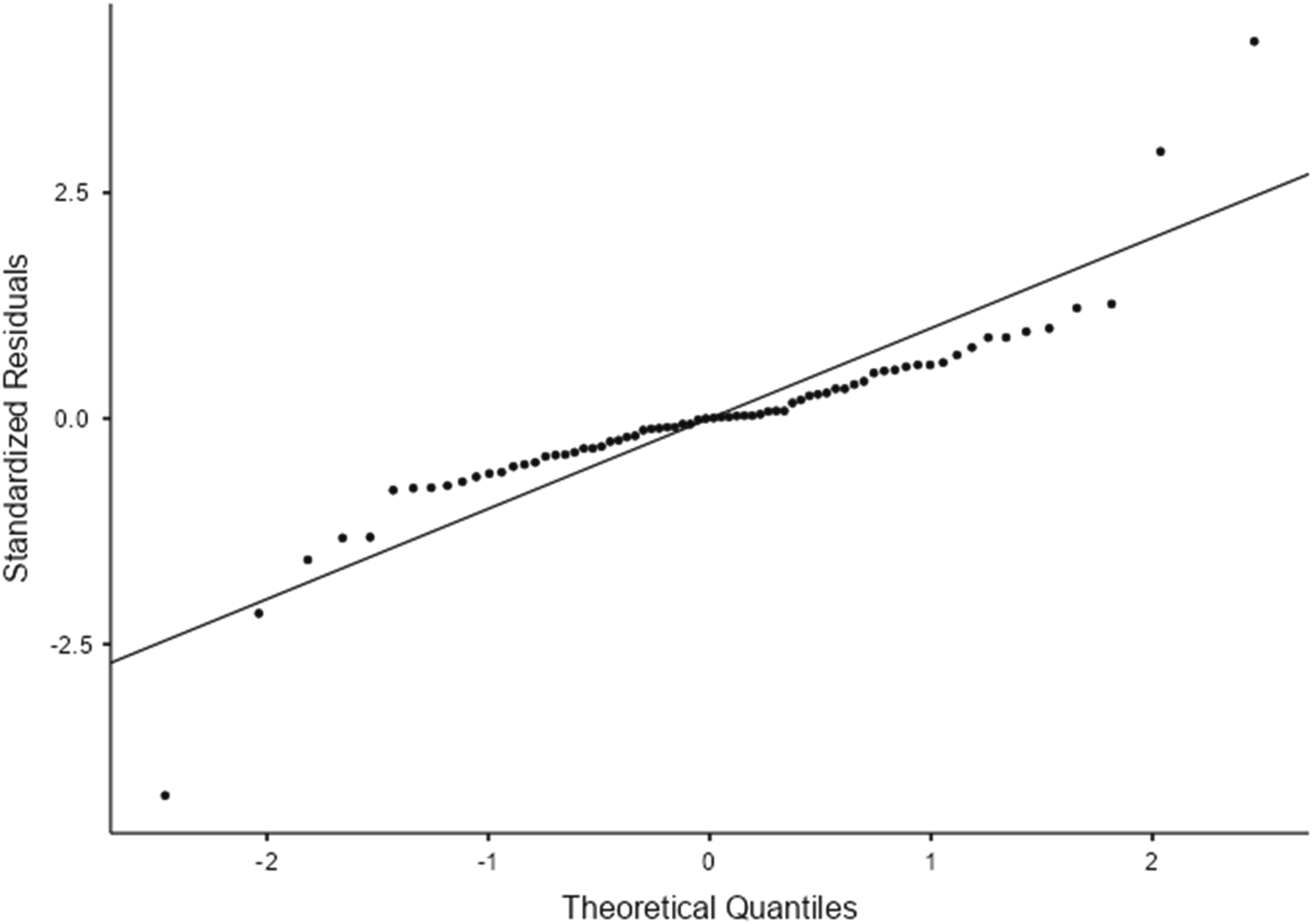
Q–Q plot of standardized residuals from the linear mixed-effects model for depression.

Q–Q plot of standardized residuals from the linear mixed-effects model for anxiety.

Q–Q plot of standardized residuals from the linear mixed-effects model for stress.
Sample Size Justification
The sample size for this study was determined based on feasibility considerations and the recommended size for group-based counseling interventions. Previous literature suggests that counseling groups consisting of approximately five to 10 participants are optimal for facilitating effective interaction, participation, and peer support within the group process.
Given the limited size of the target population and the feasibility of implementing multiple counseling groups within the study setting, a total of 24 participants were recruited and randomly assigned to four groups, with six participants per group. This group size falls within the recommended range for effective group counseling interventions.
Study Interventions
The study is composed of three interventions and a control group. Participants were assigned to the integrated music and counseling program (Arm 1), the music program (Arm 2), the counseling program (Arm 3), or the control group without intervention (Arm 4) by study nurses using the REDCap program on the central computer with limited access.
The intervention consisted of 10 weekly 90-minute sessions facilitated by two trained counseling psychologists. The Integrated Music and Counseling Program (Arm 1) combined Trotzer's concept-based group counseling 17 with structured music interventions, including guided listening and chorus singing, guitar and keyboard playing, and improvisation activities. The music therapy sessions were facilitated by a music professional (a university music instructor). The Music Program (Arm 2) involved passive and active engagement with music, focusing on emotional expression, relaxation, and social connection. The counseling program (Arm 3) followed Trotzer's approach group counseling framework, emphasizing trust-building, self-reflection, and peer support (Niyonzima et al, 2019). 17 Guided discussions and group-sharing activities to address psychological stressors and stigma were conducted.
Study Intervention
Arm 1: Integrated music and counseling program. To create the integrated music and counseling program as well as select the music pieces that were implemented in this study, the investigator evaluated the study participants’ characteristics, preferences, and interests, as well as the counseling group situations. The gathered participants’ characteristics, preferences, and interest data were analyzed. The program was created to be appropriate with the group of participants in Arm 1. The created program was reviewed and approved by the music therapy and Counseling experts.
The integrated music and counseling program was what the intervention participants were attending (90 min/visit, once a week, 10 visits), as shown in Table 1.
The music pieces that were implemented in this study were considered based on the study participants’ characteristics, preferences, and interests, as well as the counseling group situations with expert approval. Participants were asked to rank and select from groups of 3–5 musical pieces. The music pieces that were also considered for use in this study are categorized in Table 2.
Arm 2: Music program. To select the music therapy program as well as the music pieces that were implemented in this study, the investigator evaluated the study participants’ characteristics, preferences, and interests as well as the counseling group situations. The data was analyzed. The program was selected to be appropriate with the group of participants in intervention arm 2. The program created was reviewed and approved by the counseling expert and tested for construct validity in adolescents and young adults living with HIV before being used with research participants.
The music program is what the intervention participants attended (90 min/visit, once a week, 10 visits), as shown in Table 3.
Arm 3: Counseling program. To create the counseling program that was implemented in this study, the investigator reviewed the handbooks and relevant research on group counseling. The data was analyzed. The program was created to be appropriate with the group of participants in intervention arm 3.
The Integrated Music and Counseling Program.
Note: The group counseling stages in the above table are guidelines used to conduct group counseling in this study; however, group counseling in participants living with HIV is flexible according to the group's situation. Each stage may occur later or earlier than planned, or some stages may not occur as planned, such as in the responsibility and work stages.
Music Pieces Were Implemented in This Study.
The Music Program.
The counseling program was what the intervention participants attended (90 min/visit, once a week, 10 visits), as shown in Table 1, but not including the music.
Recruitment and Training of Study Psychological Counselor Staff
The investigator identified the target of two psychological counselor study staff, including the investigator, to be recruited and trained to lead the Intervention sessions. The psychological counselor staff had some experience in mental health and group counseling. Identified psychological counselors were assigned at random to lead the Intervention sessions and received the necessary training.
Training
Designated expert trainers provided training to all study psychological counselors staff to manage safety concerns among participants. The study psychological counselor study staff designated to lead the Music group sessions was trained separately from the psychological counselor staff. Separate training minimized the risk of contamination across treatment arms. The study psychological counselor staff, who were designated to lead the intervention group sessions practiced delivering the sessions during the training.
Study Psychological Counselor Staff Supervision
During psychological counselor supervision sessions, the study staff received ongoing supervision from the expert trainer. The expert trainer used the Zoom application to review any concerns raised during the sessions and problem-solve best practices.
Data Collection and Outcome Measures
At enrolment, baseline demographic data and ART adherence were collected using self-reported questionnaires. CD4 and HIV-1 RNA results were extracted from the National AIDS Program database. Mental health metrics included the Depression Anxiety Stress Scale (DASS-21), Rosenberg Self-Esteem Scale (RSES-10), and Thai Internalized HIV-related Stigma Scale (Thai-IHSS).
The Depression Anxiety Stress Scale (DASS-21) is a self-report scale for measuring depressive, anxious, and stressed emotional states. 20 The test demonstrated internal consistency and validity with the Cronbach's alpha coefficient of 0.82. The Thai version was adapted across cultures and validated. The Rosenberg Self-Esteem Scale (RSES-10) is a commonly utilized instrument that has been evaluated for reliability and validity in a variety of contexts. 21 The revised Thai RSES showed equivalent reliability and improved construct validity compared to the original. The Thai Internalized HIV-related Stigma Scale (Thai-IHSS) is a tool developed by Thai researchers (Uthis et al, 2023). 22 It is composed of 22 items which were considered as meaningful and suitable for the Thai context, including negative thoughts toward self, anticipated negative thoughts, effects of negative thoughts toward self, and effects of negative thoughts toward family and access to healthcare services. A 4-point rating scale (strongly disagree, disagree, agree, and strongly agree) was used; higher scores indicated higher HIV-related stigma.
Biospecimen Collection
We collected hair samples to determine DTG levels as markers of ART adherence at the study entry, week 10, and week 24. Hair sample was collected from the vortex posterior (back of the head) by study nurses in the clinic. At least 20 hair fibers, each 1 cm long, were obtained from the portion of the hair strands closest to the scalp. Participants were advised to avoid hair treatment, wash their hair, and have it dried before coming to the clinic. The hair samples were placed in a piece of foil, labeled, stored in a sealed plastic Ziplock bag with desiccant, and kept at room temperature with light protection prior to shipment.
This randomized controlled trial was registered at the Thai Clinical Trials Registry https://www.thaiclinicaltrials.org/. (Identifier: TCTR20241231002) on December 31, 2024.
The reporting of this randomized controlled trial follows the Consolidated Standards of Reporting Trials (CONSORT) guidelines. 23 The completed CONSORT checklist is provided as the Supplemental File.
Data Analysis
Demographic information was analyzed by using descriptive statistics (frequency distribution), mean (standard deviation, SD), or median (interquartile range, IQR) as appropriate. Intention-to-treat analysis was used for participant outcome measure analysis. The number of session attendance of all randomly selected participants was counted. Overall and within the Integrated Music and Counselling program Intervention and Control Arms, baseline variables (gender, age, severity of mental health ratings, CD4, and viral load suppression status) were compared between participants with and without VL suppression. The lost-to-follow-up rates were compared between arms. The primary outcome analysis focused on the mental health scores, ART adherence scores, and ART concentration in hair samples at week 10. As the data has a nonnormal distribution, nonparametric statistics, including Kruskal-Wallis, Friedman, and Mann-Whitney U-test, were utilized.
Statistical analyses were also performed using linear mixed-effects models (LMMs) to evaluate differences in depression, anxiety, stress, self-esteem, and internalized HIV-related stigma scores, CD4 count, HIV-1 RNA, saliva cortisol, and hair DTG concentration across treatment arms and changes over study visits. Treatment arm, study visit (entry, week 10, and week 24 for depression, anxiety, stress, self-esteem, and internalized HIV-related stigma scores, saliva cortisol, and hair DTG concentration; and entry and week 24 for CD4 count and HIV-1 RNA), and their interaction were specified as fixed effects. Participant-level random effects (random intercepts and random slopes for the arm-by-visit interaction) were included to account for within-subject correlation arising from repeated measurements.
Residuals were assumed to follow a normal distribution. Model parameters were estimated using maximum likelihood, and degrees of freedom for fixed effects were approximated using the Satterthwaite method. Overall effects of fixed factors were assessed using F-tests. Post hoc pairwise comparisons between treatment arms were conducted with Bonferroni adjustment for multiple testing.
Model assumptions were evaluated by inspecting residual diagnostics, including Kolmogorov–Smirnov and Shapiro–Wilk tests, Q–Q plots, and residual-versus-fitted value plots. Statistical significance was defined as a two-sided P-value < .05.
The SPSS Statistics program, version 29, and Jamovi Statistics program, version 2.7,24–29 were used in data analysis of this study.
Results
Demographic Characteristics
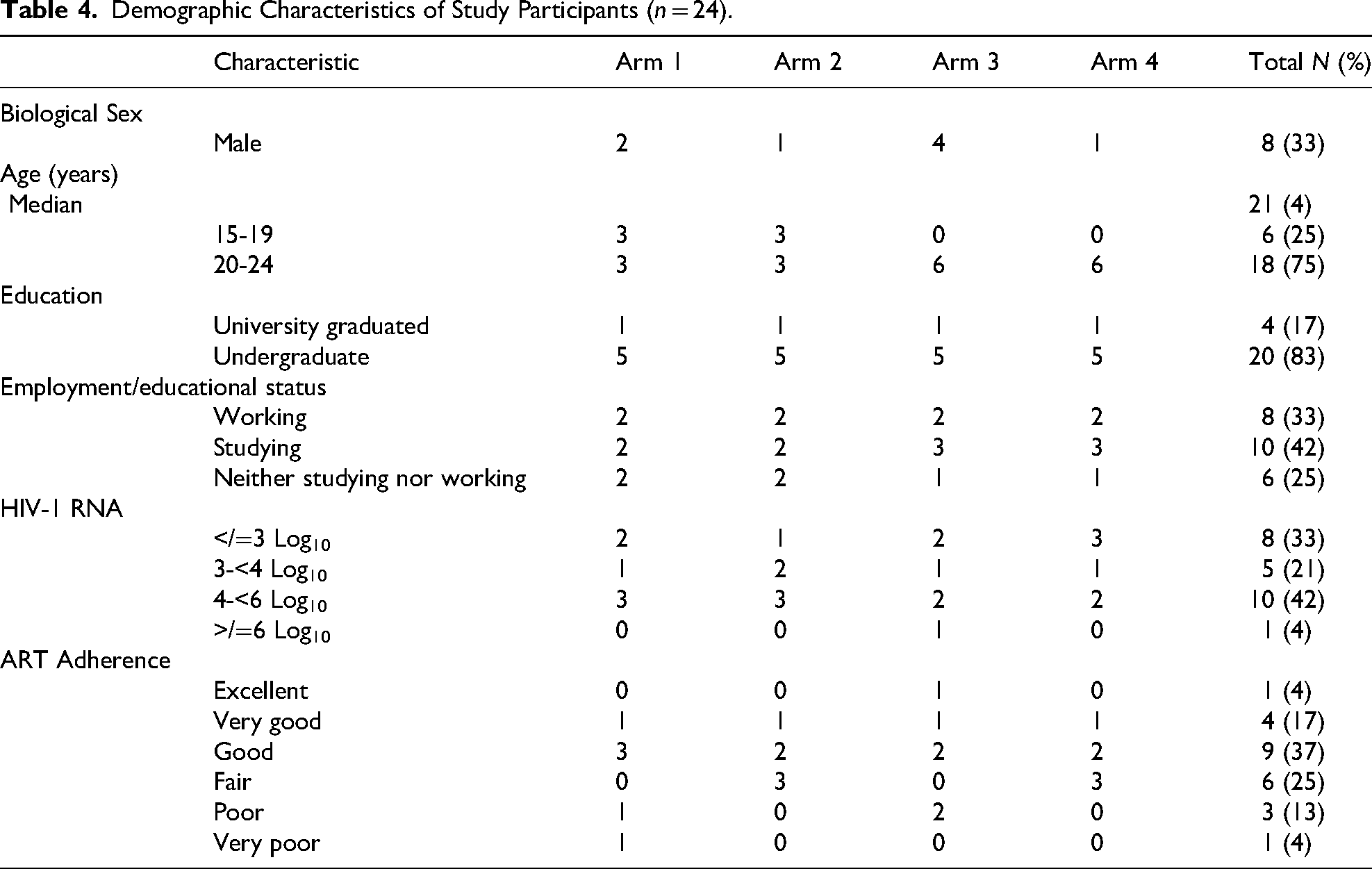
Of the 24 enrolled participants, eight (33%) were male. Their median age was 21.5 years (range 15-24). Four (17%) were university graduates, and 20 (83% were either undergraduate students or had stopped schooling. Eight (33%) were working, 10 (42%) were studying, and six (25%) did neither. Their HIV-1 RNA levels ranged from 116 to 600, 500 copies/mL within the past 12 months before enrollment. There were 16 (42%) with virologic failure (HIV-1 RNA > 1000 copies/mL) (Table 4).
Demographic Characteristics of Study Participants (n = 24).
Mental Health Outcomes
Depression, anxiety, and stress scores were analyzed using a linear mixed-effects model (LMM), with treatment arm, study visit (entry, week 10, and week 24), and their interaction specified as fixed effects, and participant-specific random effects to account for within-subject correlation arising from repeated measurements. A total of 72 observations from 24 participants were included in the analysis.
The omnibus tests of fixed effects indicated no significant main effect of treatment arm on depression scores (F = 0.168, P = .916), anxiety scores (F = 0.141, P = .933), and stress scores (F = 0.0902, P = .964) and no significant main effect of study visit (F = 0.390, P = .685 for depression, F = 5.353, P = .014 for anxiety, and F = 2.5652, P = .110 for stress). In addition, the treatment Arm × Study Visit interaction was not statistically significant (F = 1.811, P = .183 for depression, F = 1.373, P = .299 for anxiety, and F = 1.0106, P = .475 for stress), suggesting that the trajectories of depression anxiety, and stress scores over time did not differ significantly across treatment arms (Table 5).
Fixed Effects Omnibus Tests for Depression, Anxiety, and Stress.

Parameter estimates further indicated that mean depression, anxiety, and stress scores at baseline were ∼2.13, 2.78, and 3.06, respectively, with no statistically significant differences between treatment arms relative to the reference group. No significant changes in depression, anxiety, and stress scores were observed at week 10 or week 24 compared with baseline. Post hoc pairwise comparisons between treatment arms, adjusted using the Bonferroni method, revealed no statistically significant differences across any pairwise contrasts.
The random-effects component showed substantial between-subject variability, with a high intraclass correlation coefficient (ICC ≈ 0.97, 0.799, and 0.782), indicating strong within-subject consistency of depression, anxiety, and stress scores over time (Table 6).
Random Components for Depression, Anxiety, and Stress.

Note: Number of Obs: 72, Number of groups: Participant ID 24.
The Q–Q plot of standardized residuals showed that most observations aligned closely with the reference line in the central quantiles, indicating approximate normality of residuals overall. Deviations from the reference line were observed in both tails, with a few points departing noticeably from linearity, suggesting the presence of mild tail departures and potential outliers (Figures 2–4).
Notably, the model exhibited convergence issues, with an overparameterized random-effects structure relative to the number of observations. This may limit the stability and identifiability of the variance component estimates. Therefore, the results should be interpreted with caution, and sensitivity analyses using a more parsimonious random-effects structure are warranted.
At enrollment, their self-esteem, IHSS, depression, anxiety, and stress scores were Similar across the four arms. AYA-PHIV in Arm 1 (integrated music and counseling program) had significantly increased self-esteem scores at week 10 and week 24. Increasing trends were observed for self-esteem scores of participants in Arm 2 (music program) and Arm 3 (counseling program), although the changes were not statistically significant. There was no change in the self-esteem scores among AYA-PHIV in Arm 4 (the control group).
Self-esteem scores (continuous outcome) were also analyzed using linear mixed-effects models (LMMs) to examine the effects of study arm, study visit (entry, week 10, and week 24), and their interaction. Fixed effects included arm, visit, and arm-by-visit interaction. Random effects were specified at the participant level (Participant ID) with a random intercept and arm-by-visit slopes to account for within-subject correlation of repeated measures. Models were fitted using maximum likelihood estimation with the nloptwrap optimizer, and degrees of freedom were computed using the Satterthwaite approximation. Wald 95% confidence intervals were reported (Tables 7 and 8).
Fixed Effects Omnibus Tests for Self-Esteem.

Random Components for Self-Esteem.

Note: Number of Obs: 72, Number of groups: Participant ID 24.
Residual normality was assessed using Kolmogorov–Smirnov and Shapiro–Wilk tests and Q–Q plots. Given the complexity of the random-effects structure relative to the sample size, model results were interpreted with caution, and sensitivity analyses using simplified random-effects structures were conducted to assess the robustness of findings (Figure 5).
Q–Q plot of standardized residuals from the linear mixed-effects model for self-esteem.
A significantly decreased internalized HIV-related stigma was observed among participants in Arm 1 and Arm 3 at both week 10 and week 24 of study participation. No change was observed in Arm 2 AYA-PHIV and the control arm. No significant change in depression, anxiety, and stress among AYA-PHIV in any intervention arms. In addition, we found participants in Arm 4 (control group) had significantly increased depression scores at week 24 (Table 9).
Self-Esteem and Internalized HIV-Related Stigma in Study Participants.

Self-esteem scores (continuous outcome) were also analyzed using LMMs to examine the effects of study arm, study visit (entry, week 10, and week 24), and their interaction. Fixed effects included arm, visit, and arm-by-visit interaction. Random effects were specified at the participant level (Participant ID) with a random intercept and arm-by-visit slopes to account for within-subject correlation of repeated measures. Models were fitted using maximum likelihood estimation with the nloptwrap optimizer, and degrees of freedom were computed using the Satterthwaite approximation. Wald 95% confidence intervals were reported (Tables 10 and 11).
Fixed Effects Omnibus Tests for Self-Esteem.

Random Components for Self-Esteem.

Note: Number of Obs: 72, Number of groups: Participant ID 24.
Residual normality was assessed using Kolmogorov–Smirnov and Shapiro–Wilk tests and Q–Q plots. Given the complexity of the random-effects structure relative to the sample size, model results were interpreted with caution, and sensitivity analyses using simplified random-effects structures were conducted to assess the robustness of findings (Figure 6).

Q–Q plot of standardized residuals from the linear mixed-effects model for self-esteem.
The LMM showed no significant overall differences in HIV-1-related stigma between study arms, F(3, 9.96) = 0.117, P = .948. In contrast, stigma scores changed significantly over time, F(2, 16.35) = 66.623, P < .001, and a significant Arm × Study Visit interaction was observed, F(6, 11.83) = 24.855, P < .001, indicating differential stigma trajectories across study arms during follow-up (Table 12). Random-effects estimates demonstrated substantial between-participant variability in baseline stigma (intercept variance = 49.10; ICC = 0.965), with additional heterogeneity in individual change patterns across arms and study visits (Table 13).
Fixed Effects Omnibus Tests for HIV-1-Related Stigma.

Random Components for HIV-1-Related Stigma.

Note: Number of Obs: 72, Number of groups: Participant ID 24.
Model diagnostics supported the adequacy of distributional assumptions; inspection of the normal Q–Q plot of standardized residuals showed close alignment with the theoretical reference line, with only minor deviations at the upper tail, indicating approximate normality of residuals (Figure 7).

Q–Q plot of standardized residuals from the linear mixed-effects model for HIV-1-related stigma.
ART Adherence Outcomes
Improved self-report ART adherence was seen during and after the intervention at week 10 and 24, respectively, among AYA-PHIV who participated in Arms 1, 2, and 3, although it did not reach a significant level. The DTG hair level of our study participants ranged from 200 to 4143 pg/mL. While there is no therapeutic range for DTG hair level, we found six participants (one, three, and two participants in Arms 1, 3, and 4, respectively) with increased DTG hair levels by 1.5 times or more when compared to baseline at the study enrollment. However, the decrease in median HIV-1 RNA level was observed in all study arms (Table 14). At week 24, 16 (67%) achieved virologic suppression.
HIV-1 RNA Level at the Study Entry and Week 24 of Participants in Each Arm.

LMMs showed no significant between-arm differences in HIV-1 RNA levels (F = 0.757, P = .612) and no significant main effect of study visit (F = 2.973, P = .142). The Arm × Study Visit interaction was also not statistically significant (F = 1.783, P = .359), indicating comparable viral load trajectories across study arms over follow-up (Table 15).
Fixed Effects Omnibus Tests for HIV-1 RNA.

Fixed-effect estimates were not statistically different from zero, with wide confidence intervals, consistent with substantial between-participant heterogeneity (ICC ≈ 1.00), suggesting that interindividual variability dominated within-person change over time (Table 16).
Random Components for HIV-1 RNA.
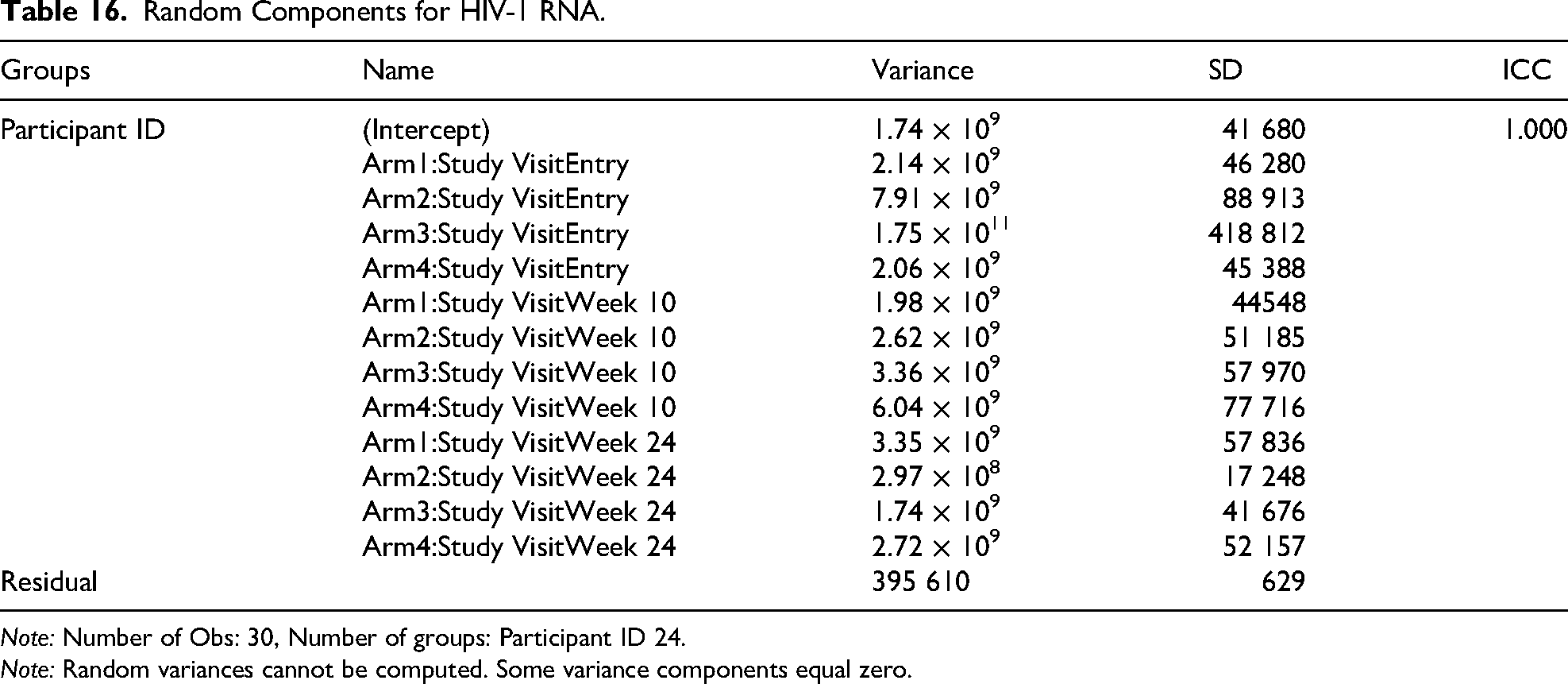
Note: Number of Obs: 30, Number of groups: Participant ID 24.
Note: Random variances cannot be computed. Some variance components equal zero.
Using LMMs with study arm, visit (entry and week 24), and their interaction as fixed effects and participant-level random effects, we found no statistically significant differences in HIV-1 RNA (copies/mL) across study arms (F = 0.757, P = .612), no main effect of visit (F = 2.973, P = .142), and no Arm × Visit interaction (F = 1.783, P = .359).
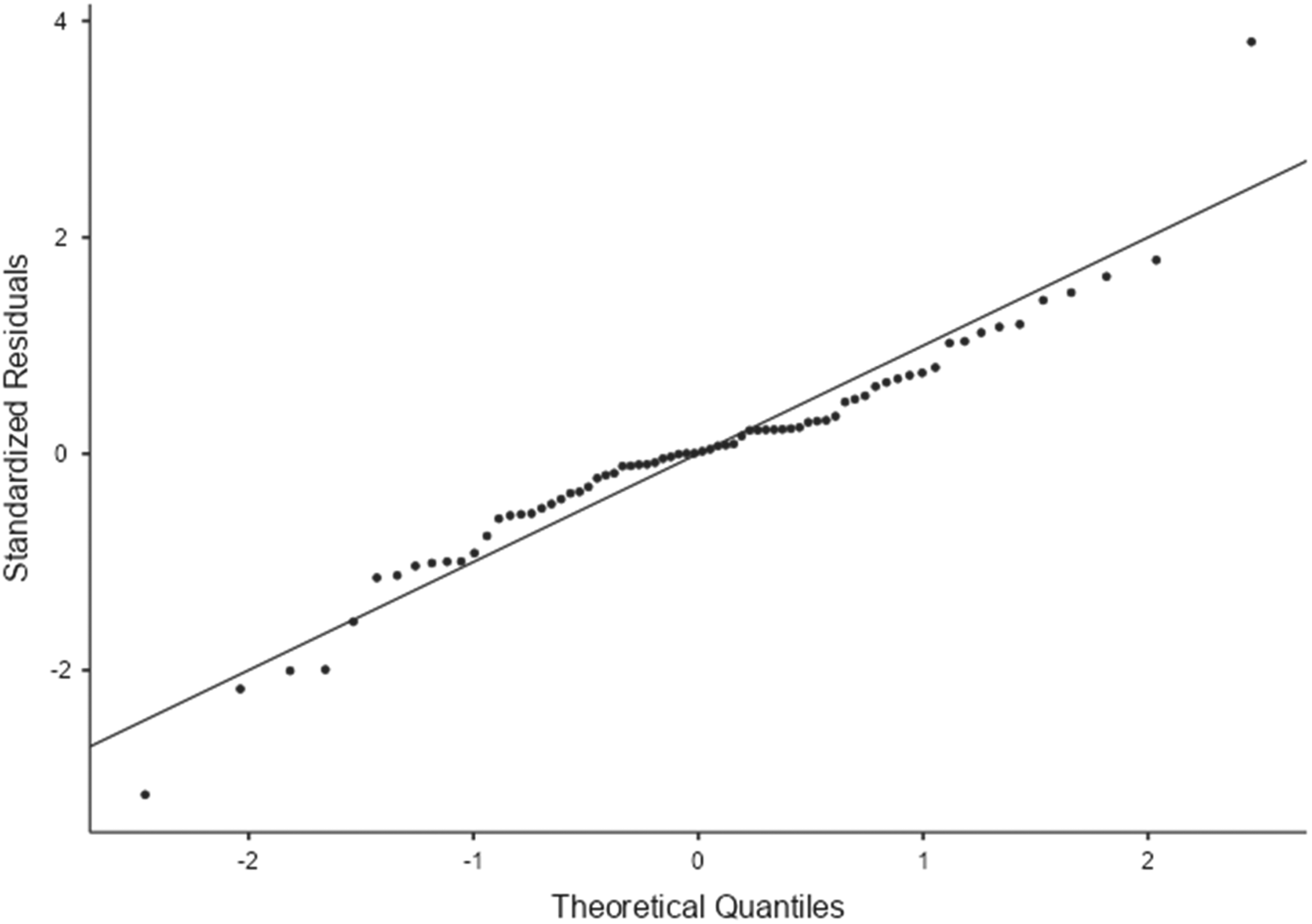
None of the fixed-effect parameter estimates reached statistical significance (P < .05). Substantial between-participant variability was observed, as indicated by large random-effects variances. Visual inspection of the Q–Q plot suggested deviations from normality in the tails of the residual distribution, consistent with the Shapiro–Wilk test indicating potential departures from normality (Figure 8).

Q–Q plot of standardized residuals from the linear mixed-effects model for HIV-1 RNA.
Discussion
This study demonstrated the benefits of the integrated music and counseling program intervention on self-esteem, internalized HIV-related stigma, and ART adherence among AYA-PHIV.
The effect on self-esteem was in line with previous research using music therapy intervention in participants with a diagnosis of “adjustment reaction to adolescence,” in which an increase in self-esteem was reported. 30 In this study we used different music activities, which could affect mental health of AYA-PHIV like another previous study documented increased self-expression and self-esteem from musical performance. 31 Music allows participants to express their emotions and their personalities, which can lead to better mental health and self-esteem. This was documented in a study of a woman with severe bereavement who struggled to define her identity. She improved after music therapy. 32 Engaging in a variety of musical activities can boost one's confidence and sense of self, which is noticeable in a therapeutic setting. 33
Low self-esteem among AYA-PHIV put them at more vulnerable to internalized stigma related to HIV/AIDS, which results from the self-deprecating effects of comparing oneself to stigmatizing social norms about HIV. 30 Our result demonstrated that the integrated music and counseling and the counseling programs were associated with significantly decreased internalized HIV-related stigma in AYA-PHIV. The results are in line with the previous research addressing the benefits of other elements of creativity and HIV, including applied sculpting, drawing, song, and dance,34–38 while empowerment, health promotion, and HIV awareness were more powerful in tackling internalized stigma. More strategies for decreasing internalized stigma associated with HIV were mentioned in a recent systematic review. 39
In addition, the LMM suggested that self-esteem changed over time and that trajectories differed across study arms. However, model nonconvergence and identifiability issues arising from an overparameterized random-effects structure relative to the sample size warrant cautious interpretation of the quantitative estimates. Sensitivity analyses using simplified random-effects structures (reported in the Supplemental Material) yielded directionally consistent findings, supporting the qualitative conclusions regarding differential temporal patterns of self-esteem across arms.
No significant difference was observed in the depression, anxiety, and stress levels among our study participants after intervention. This finding was inconsistent with previous metaanalyses that documented improved anxiety and depressive symptoms. 40 This might be due to the low frequency of anxiety and depression at enrollment and the short follow-up period. Moreover, we could identify other psychosocial stressors during the study period, including breaking up with a boyfriend, failing the university entrance exam, being hospitalized for acute bronchitis, retiring from the university, and encountering physical and psychological abuse, which could explain worsening mental health scores.
Although the residual distribution appears approximately normal in the central range, the observed tail deviations may reflect mild nonnormality or the influence of outlying observations. In the context of a relatively small sample size and a complex mixed-effects structure, such departures could affect the precision of parameter estimates and confidence intervals. Nevertheless, the deviations were not severe, and the normality assumption was considered reasonably met for inferential purposes. These findings support the primary analyses while underscoring the importance of complementary sensitivity analyses and cautious interpretation.
LMMs accounting for within-participant repeated measures indicated temporal changes in HIV-1-related stigma, with model-estimated means showing improvement from baseline across follow-up visits. The magnitude and pattern of change varied by study arm, suggesting context-specific effects of the intervention or care pathways on stigma-related outcomes.
For young people, group intervention seems to be an effective method to promote mental health and general health. Like a study in South Africa using family-based psychosocial intervention in early adolescents living with HIV, improvement in mental health, behaviors, HIV treatment knowledge, stigma, communication, and ART adherence were noted. 41
Reductions in HIV-1-related stigma over time carry important clinical and public health implications, given the well-established associations between stigma, care engagement, disclosure, and treatment adherence. The observed group-specific trajectories highlight the need for contextually tailored stigma-reduction strategies rather than uniform approaches. Such targeted interventions may enhance psychosocial well-being and support sustained engagement in HIV care.
Improved self-report ART adherence and HIV-1 RNA levels were observed during and after the intervention at week 10 and week 24, respectively, among AYA-PHIV in all three intervention arms. The result was consistent with a previous study in Thai AYA-PHIV of similar age using an empowerment intervention, which reported increased ART adherence. 42 They did not have HIV-1 RNA outcome, while we did. Nevertheless, improved ART adherence following group therapy in another study among adolescents with HIV was reported. 44 Unlike the report from a South African study, which reported no significant effect of group counseling on the treatment outcomes. 41
To our surprise, a significantly decreased HIV-1 RNA level was also observed in the control arm when compared to baseline. Study participation could be an explanation for improving adherence. AYA-PHIV might improve their ART adherence due to awareness of being observed, which was previously described as the Hawthorne effect. 43 In another word, this might be explained by the effect of social support, such as positive communication and adherence messages transferred by the study staff while being followed up. A positive provider-patient relationship was reported to be associated with higher ART adherence among people living with HIV. 44 This finding was in line with several previous reports, in which self-compassion was found to be associated with enhanced participation in behaviors that promote health 45 and improved physical well-being and health.46,47
These contextual supports may have functioned as co-interventions, attenuating detectable differences between trial arms. Such “trial effects” or Hawthorne-like effects are well recognized in pragmatic HIV research, particularly in settings where participants receive intensified follow-up, counseling, and monitoring beyond routine care. Other unmeasured factors, including regression to the mean, concurrent programmatic improvements at study sites, or changes in clinical management during the study period, may also have contributed to parallel viral load trajectories across groups. Collectively, these findings underscore the importance of accounting for background psychosocial and service-level supports when interpreting intervention effects on virologic outcomes in real-world HIV care settings.
From an implementation perspective, heterogeneity in attendance and engagement across group sessions may have diluted intervention effects. Group-based formats, while scalable and resource-efficient, may be less responsive to individualized barriers commonly faced by people living with HIV, including stigma, disclosure concerns, family or partner dynamics, and co-occurring psychosocial stressors. These factors are particularly salient in real-world service delivery and may require more tailored or multicomponent approaches to achieve measurable changes in mental health and adherence outcomes.
Notably, the absence of statistically significant effects does not preclude clinical relevance. Small, nonsignificant improvements may still be meaningful in practice when interventions are low-cost, acceptable to clients, and feasible for integration into existing service platforms. Moreover, group counseling may confer additional benefits not fully captured by the primary outcome measures, such as enhanced peer support, normalization of experiences, and improved therapeutic alliance with care providers, which may contribute to longer-term engagement in HIV care.
Although the group counseling program integrated with music did not demonstrate statistically significant superiority over the comparison arms in improving ART adherence, the direction and pattern of change observed suggest a potentially meaningful relationship between participation in the music-enhanced group sessions and engagement in medication-taking behaviors. Music-based activities could facilitate emotional expression, stress reduction, and group cohesion, thereby creating a supportive and nonstigmatizing environment that fostered motivation and self-efficacy related to treatment adherence. Such mechanisms are consistent with psychosocial theories emphasizing the role of affecting regulation, social connectedness, and intrinsic motivation in sustaining long-term adherence behaviors among people living with HIV.
Importantly, the lack of statistically significant between-group differences should not be interpreted as evidence of no clinical or practical relevance. In the context of a small sample size and high levels of background psychosocial support provided to all participants, the incremental benefit of the music-integrated group counseling may have been diluted. Nevertheless, the observed trends underscore the potential value of incorporating creative, culturally sensitive modalities such as music into adherence support interventions, particularly for adolescents and young adults, for whom conventional counseling approaches may be perceived as less engaging. Future trials with an increased number of participants are warranted to further delineate the specific contribution of music-based group counseling to ART adherence and to identify subgroups most likely to benefit.
The study strength included study participants with similar characteristics in each intervention group using random assignment, hair DTG level measurement, and available HIV-RNA results, which reflected HIV treatment adherence and outcomes. Future research should explore larger samples, that is, more than one group assigned to the same intervention, extended follow-up periods, and integration with digital health interventions to sustain ART adherence improvements and strengthen self-esteem.
Conclusion
The study demonstrated that integrated music and counseling programs for AYA-PHIV were associated with improving self-esteem and reducing internalized HIV-related stigma. Study participants reported better antiretroviral treatment adherence and improved virologic outcomes.
We support including psychosocial interventions in comprehensive HIV care strategies, especially for high-risk individuals with mental health or adherence issues. A larger study with an increased sample size is warranted to confirm these findings, improve statistical power, and better delineate the clinical and programmatic implications of group-based counseling interventions within routine HIV care settings. Integrated music and counseling programs could be adopted as they offer promising avenues for enhancing self-esteem and reducing stigma among AYA-PHIV.
Supplemental Material
sj-pdf-1-jia-10.1177_23259582261439584 - Supplemental material for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial
Supplemental material, sj-pdf-1-jia-10.1177_23259582261439584 for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial by Chintana Khamrong, Rattika Thammalangka, Kalunyu Kotchawat, Nakhon Khamrong, Linda Aurpibul, Jakkrit Klaphajone, Teerawan Teerapong and Natthapol Kosashunhanan in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582261439584 - Supplemental material for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial
Supplemental material, sj-docx-3-jia-10.1177_23259582261439584 for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial by Chintana Khamrong, Rattika Thammalangka, Kalunyu Kotchawat, Nakhon Khamrong, Linda Aurpibul, Jakkrit Klaphajone, Teerawan Teerapong and Natthapol Kosashunhanan in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-4-jia-10.1177_23259582261439584 - Supplemental material for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial
Supplemental material, sj-docx-4-jia-10.1177_23259582261439584 for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial by Chintana Khamrong, Rattika Thammalangka, Kalunyu Kotchawat, Nakhon Khamrong, Linda Aurpibul, Jakkrit Klaphajone, Teerawan Teerapong and Natthapol Kosashunhanan in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-5-jia-10.1177_23259582261439584 - Supplemental material for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial
Supplemental material, sj-docx-5-jia-10.1177_23259582261439584 for Effects of Music and Counseling Programs on Mental Health and Antiretroviral Treatment Adherence of Adolescents and Young Adults Living With HIV in Northern Thailand, a Randomized Trial by Chintana Khamrong, Rattika Thammalangka, Kalunyu Kotchawat, Nakhon Khamrong, Linda Aurpibul, Jakkrit Klaphajone, Teerawan Teerapong and Natthapol Kosashunhanan in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
This study would not be possible without the dedication and diligent effort of 24 adolescents and young adults, their parents/guardians, and healthcare providers, Family clinic (IMPAACT) team, RIHES, CMU, my main advisor, Dr Natthapol Kosashunhanan, MD, my co-advisors, Dr Linda Aurpibul, MD, Assoc Prof Jakkrit Klaphajone, MD, and Assoc Prof Dr Teerawan Teerapong.
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from the Human Experimentation Committee (HEC), Research Institute for Health Sciences, Chiang Mai University (certificate approval number 30/2023). Written informed consent was obtained from all participants, consent and assent were also obtained from the caregiver and the participant, respectively, prior to enrollment. This randomized controlled trial was registered at the Thai Clinical Trials Registry. (Identifier: TCTR20241231002). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and reported following the CONSORT guidelines.
Consent to Participate
Before enrollment, participants provided written informed consent for study participation, inclusion, and use of data in publication; for those under 20 years of age, consent and assent were also obtained from the caregiver and the participant, respectively.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Chintana Khamrong received funding from the Research Institute for Health Sciences, Chiang Mai University, Chiang Mai, Thailand, with grant number (grant number 013/2566) that contributed to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.