
Abstract
As individuals with HIV infection are living longer, the management of psychiatric disorders has increasingly been incorporated into comprehensive care. Individuals were recruited from an outpatient HIV clinic to assess the prevalence and related associations of current psychiatric disorders and biomarkers. Of the 201 participants who completed the interviews, the median age was 43.5 years, and the majority was male and African American. Most were receiving HIV therapy and 78% of those had achieved virologic suppression. Prevalent psychiatric diagnoses included major depressive disorder, generalized anxiety, and agoraphobia. Alcohol and cocaine/crack abuse and dependence were common substance use disorders. Current receipt of HIV therapy was less common among those diagnosed with generalized anxiety disorder. Agoraphobia was the only disorder associated with unsuppressed viral load. Psychiatric and substance use disorders are highly prevalent among an urban HIV clinic population, although we identified few associations between psychiatric diagnoses and HIV diseases status.
Keywords
Introduction
With the transition of HIV infection to a chronic disease model, a significant proportion of care has shifted to the treatment of comorbid conditions in order to improve health outcomes and reduce HIV transmission risk behaviors. 1 Psychiatric disorders are common comorbidities in HIV-infected populations, with mood disorders being highly prevalent. These psychiatric comorbidities create challenges for engagement in care and also increase the likelihood of engaging in high-risk behaviors (unprotected sex, multiple sex partners, heavy alcohol and illicit drug use). 2 –6 Although there are currently no guidelines to manage psychiatric disorders in the HIV clinic setting, these disorders adversely affect the management of HIV infection.
Although the exact role of psychiatric disorders in HIV infection remains unclear, previous research illustrates that depressive symptoms fluctuate during the course of HIV infection with negative consequences, including poor medication adherence and increased likelihood of engagement in high-risk behaviors. 2,7 –9 Specifically, depressive symptomatology has been found to be a prevalent and salient barrier to continued engagement in medical care, control of HIV viremia, medication adherence, and engagement in secondary prevention behaviors among individuals with HIV. 10 –12 Few studies have examined the prevalence and management of psychiatric disorders beyond depression. 13 Psychiatric disorders are not routinely assessed in HIV clinic populations due to time and staffing constraints as well as limited expertise. Furthermore, patients receiving care at HIV clinics are likely to present for care only in this one setting, rather than seeing a mental health clinician, leaving HIV care providers managing patients with complicated multimorbidity. This study was conducted to assess the prevalence of psychiatric disorders and the relationship between these disorders and HIV-related care and health outcomes. Determining the actual prevalence of these disorders will assist in understanding the breadth of the psychiatric morbidity in the patient populations.
Methods
Individuals presenting for care at the Washington University HIV Clinic in Saint Louis, Missouri between February and August 2009 were invited to participate in this study. This clinic served approximately 1700 patients annually and was the largest HIV care provider in the region. All individuals with HIV and 18 years or older were eligible to participate in a 2-hour interview. Individuals were remunerated for participation in the study and were given transportation vouchers, when necessary. The computerized interview was conducted in a private room at the clinic. The study protocol was approved by the Washington University Human Research Protection Office, and all participants provided written informed consent.
We used the Diagnostic Interview Schedule for DSM 4.0 Screener (DIS 4.0) 14 to identify current psychiatric diagnoses (within the past 12 months) through structured interviews with a trained research assistant. Diagnoses are determined based on responses to questions in multiple diagnostic systems. For this study, we assessed current psychiatric symptoms for occurrence, severity, comorbidity with other symptoms, age of onset, and remission. The results are relevant for the diagnosis of psychiatric illnesses within the past 12 months. Thus, the diagnoses are time specific, for example, major depressive episode (MDE) is related to symptoms and events occurring during the preceding 12 months. Specifically, we were interested in focusing our diagnostic interviewing on disorders that were more prevalent such as mood disorders and substance abuse and dependence.
Sociodemographic characteristics, as well as quality of life as measured by the Short-Form 12, were collected. 15 Biomedical markers were abstracted from medical records including current CD4 count, plasma HIV RNA level, use of antiretroviral therapies (ARTs) and other concomitant medications, and incident sexually transmitted infections were collected within the past 12 months. HIV viral load measures were used as proxy for medication adherence. 16 Antiretroviral therapy was defined as the use of ≥3 antiretroviral drugs from 2 or more classes. Virologic suppression was defined as having an HIV RNA of <400 copies/mL.
Statistical Analyses
Descriptive analyses were conducted to identify the prevalence of individual disorders. The associations between sociodemographic factors and HIV-related measures (viral load and CD4 counts) were analyzed by Analyses of Variance (for continuous variables) and chi-square tests (for dichotomous variables). The Pearson product–moment correlation coefficient was calculated to assess relationships between diagnoses. Binary logistic regression analyses were conducted with receipt of antidepressant as a dependent variable to identify the association of these medications with individual diagnoses. HIV viral loads were dichotomized (<400 and ≥400 copies/mL). Education levels were dichotomized: ≤high school graduate/general equivalency diploma or >high school degree. Employment status was dichotomized into unemployed (including receiving disability benefits) and employed (part or full time). Race was dichotomized to White and African American and other minorities. There were fewer than 5 participants who self-identified as Hispanic/Latino, American Indian/Alaska Native, or Asian American. Annual income was dichotomized into ≤ and >US$10,000. Depression severity was dichotomized as those who expressed symptoms of major or other depressive disorders within the past 2 weeks and those who did not. All tests were 2 tailed, and P < .05 was considered significant. Data analyses were performed using SPSS software (version 21.0; Chicago, Illinois).
Results
A total of 201 individuals participated in this study, with the majority of the sample being male, African American, with a median age of 43.5 years. Most of the sample had low income, were unemployed, and attained less than a high school education. Nearly 40% of the sample (n = 77) reported their health as either excellent or very good. More than three-quarters of the sample were currently on ART, among those 78% had viral loads <400 copies/mL. Overall, 69% of the sample was virally suppressed. Details of baseline characteristics are included in Table 1.
Sample Characteristics.a
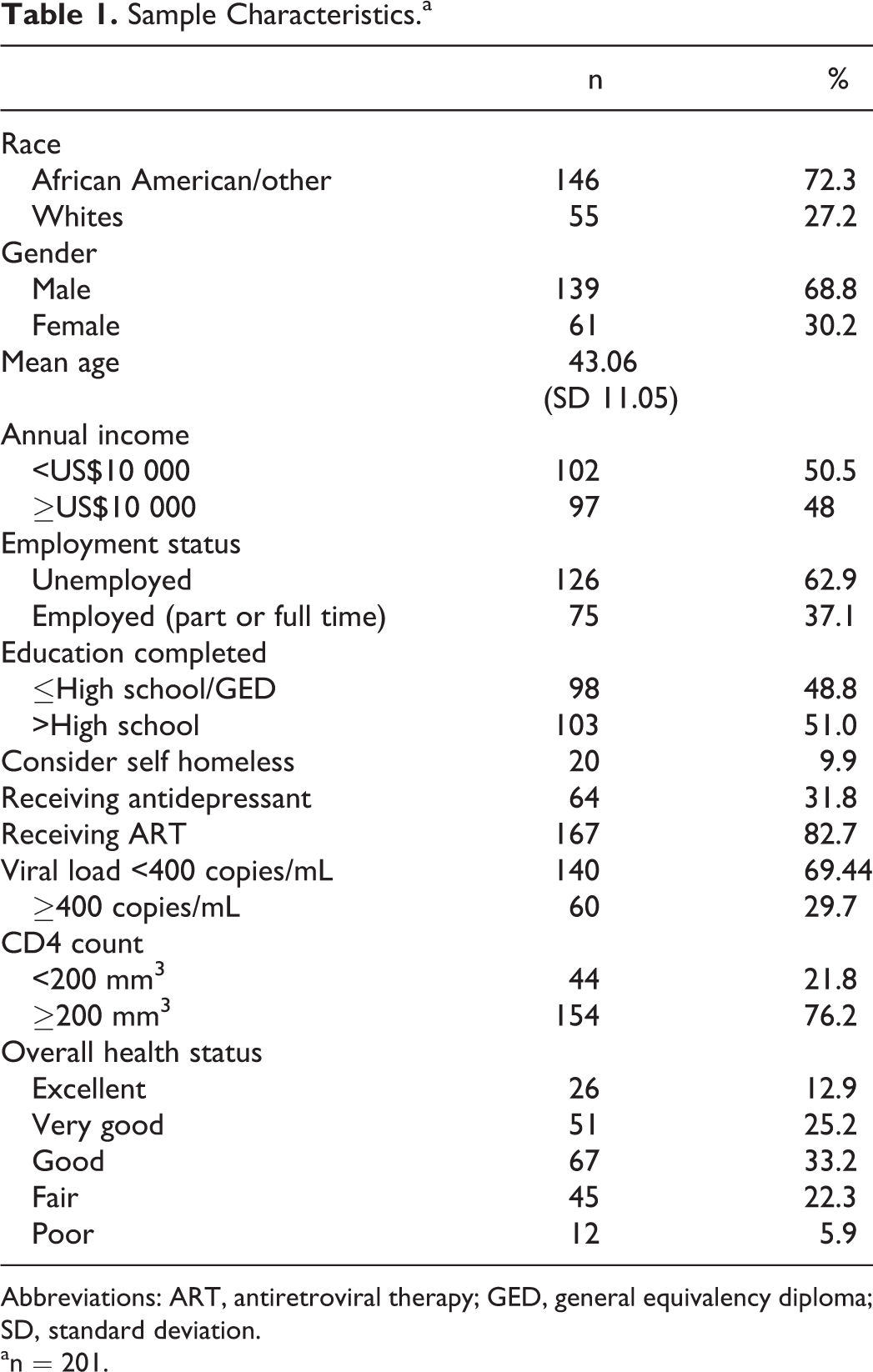
Abbreviations: ART, antiretroviral therapy; GED, general equivalency diploma; SD, standard deviation.
an = 201.
The most prevalent current psychiatric disorders were MDE in the past 12 months (n = 78; 38%), pain disorder (n = 85; 42%), generalized anxiety disorder (GAD; n = 29; 14%), and agoraphobia (n = 32; 15%). Nearly one-fifth (n = 35) of the sample endorsed alcohol dependence. Alcohol abuse (n = 27; 13%) and cocaine dependence (n = 25; 12%) were also prevalent among this sample. More detailed prevalence rates are shown in Table 2. Many of the diagnoses were significantly correlated with one another as 20% of the sample had multiple diagnoses. For instance, MDE correlated significantly with posttraumatic stress disorder (PTSD), GAD, agoraphobia, and alcohol dependence. Substance use disorders were also correlated. Table 3 depicts these associations in a correlation matrix.
Prevalence Rates of Psychiatric Disorders.a
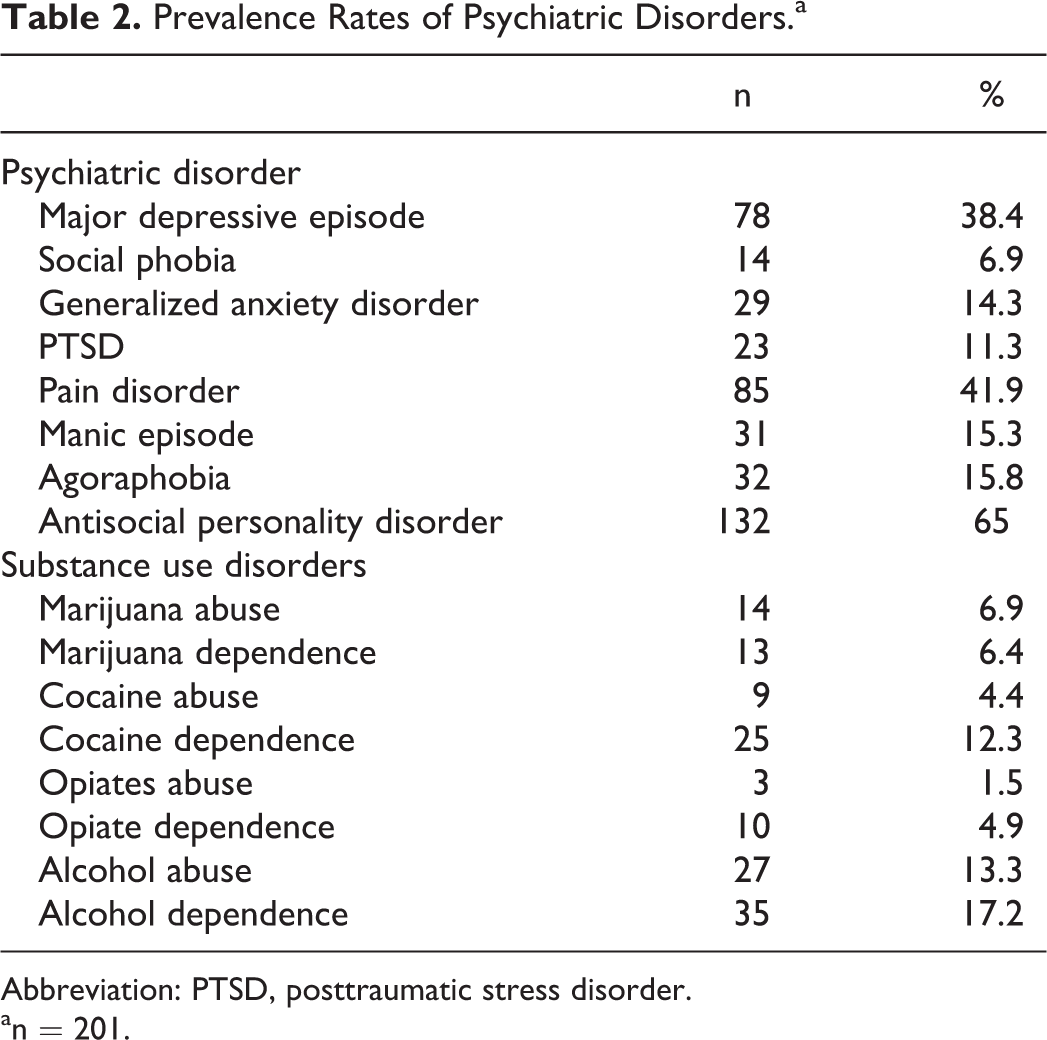
Abbreviation: PTSD, posttraumatic stress disorder.
an = 201.
Correlation Values between Prevalent Psychiatric Diagnoses.a

Abbreviations: GAD, generalized anxiety disorder; MDD, major depressive disorder; PTSD, posttraumatic stress disorder.
aPearson R presented.
bP < .001.
cP < .05.
We also assessed associations between sociodemographic and biomedical factors with individual psychiatric diagnoses. Whites were more often diagnosed with MDE than African Americans (58% versus 35%; P < .05) as well as GAD (26% versus 11%; P < .05). Individuals who endorsed agoraphobia were more likely to report lower perceived overall health (25% versus 13%; P < .05) and to have viral loads >400 copies/mL (24% versus 13%; P < .05) than those who were not diagnosed with agoraphobia. We did not identify any other sociodemographic characteristics that were associated with specific diagnoses (data not shown).
Discussion
Using the DIS 4.0, a validated tool for psychiatric diagnoses, we identified a diverse set of psychiatric disorders and substance use diagnoses that are common among HIV-infected individuals. Overall, psychiatric diagnoses and substance use disorders were quite common. Prevalence rates for mood disorders were high among this sample, with one-third of the cohort reporting an MDE in the preceding 12 months; pain disorder, GAD, agoraphobia, and PTSD. Overall, the sample was managing their HIV infection effectively, which suggests a high level of engagement in care.
This study identified correlations that have been established in other samples, with MDE being correlated with alcohol abuse and dependence and GAD. 17 –19 Providing comprehensive care to persons living with HIV, including addressing psychiatric and substance use disorders, is a significant challenge that requires the expertise of a multidisciplinary team approach. High rates of substance use disorders are likely to interrupt consistent engagement in care, 19 and thus addressing these disorders are a primary area of intervention. Utilizing the medical home model, as well as further training for providers and case managers to identify substance use disorders, will likely provide more successful approaches to improved health outcomes for patients with HIV. 20
Not only does the DIS provide valid and reliable diagnoses of current mood and substance use disorders, 21 –23 it also identifies individuals with antisocial personality disorder (ASPD). We identified 65% of this sample as endorsing ASPD. Given the very high prevalence, we were concerned about the accuracy, as using a lay person may miss some of the sensitivity necessary for this complicated diagnosis, although previous findings suggest high rates of ASPDs among individuals with HIV. 24 –26 Additional research is needed to determine how ASPD is related to HIV infection and whether it affects the course of HIV disease progression, namely medication nonadherence and engagement in HIV transmission risk behaviors.
This cohort also reported high rates of pain disorder, although we cannot determine whether pain is a psychosomatic manifestation of an underlying psychiatric disorder, HIV disease, or another process. 27 Nevertheless, it negatively affects quality of life. Given that this interview was the first time, many of the respondents were able to explore symptoms of psychiatric illness, manifestations of pain and depression may be similar. 28,29 We did find that those individuals who were diagnosed with pain disorders were commonly prescribed antidepressants indicating that the relationship between pain and psychiatric diagnoses needs further exploration. In the context of HIV infection, previous research demonstrates that psychiatric symptom expression is altered by the prescription of pain medications. 30 Thus, pain disorder diagnoses may reflect the initial expression of psychiatric symptoms and opiate abuse and/or dependence.
With current ART, the HIV epidemic is rapidly evolving. Previously, psychiatric symptoms may have been most prominent in newly diagnosed patients due to fear and prognosis and in persons with advanced AIDS due to the severity of their disease. With the transition to a chronic disease model, psychiatric symptoms are just as likely to reflect the complexities of an individual’s nonmedical concerns as their HIV disease status. Thus, care providers must be attuned to psychiatric symptoms at all stages of HIV disease. While antidepressants may not be a panacea for all manifestations of mood disorders, these medications likely serve an important role in the care and management of these comorbidities that are all too common in persons living with HIV infection.
There are several limitations of these findings. We conducted this study in one clinic in a Midwestern urban city. The patient population was recruited during clinic visits and thus may have been more likely to be engaged in care. The rates of psychiatric disorders were higher than uninfected populations, yet we were unable to identify whether these rates would be comparable to low-income populations with other chronic diseases. Although we only identified a relationship between agoraphobia and HIV outcomes, we cannot conclude definitively that these other diagnoses do not affect HIV disease management. It is likely that the individuals who participated in this study were comfortable with these topics and therefore better able to engage in HIV care and manage their HIV infection. Their engagement in care also provides the opportunity to address mental health issues with their medical provider. We were unaware whether patients were currently seeking mental health care in other clinic settings. Further, antidepressant treatment and MDE time frame may not have been identical.
In summary, our data confirm that psychiatric and substance use disorders are very common among HIV outpatient populations, with nearly 20% having more than 1 disorder. Given the evolving chronic disease model for HIV care, effective management of these comorbid disorders is critical but complicated due to limited time and expertise of providers as well as inadequate resources to meet this unmet need. The interplay between pain symptoms and psychiatric symptoms is an area that requires additional research to optimize care for populations with HIV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This publication was supported by the Washington University Institute of Clinical and Translational Sciences grants UL1 TR000448 (PI: Bradley Evanoff) and KL2 TR000450 (PI: Enbal Shacham) from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.