
Abstract
Adherence to antiretroviral therapy (ART) is lower in adolescents with HIV (AWH) than in any other age group, partly due to self-regulatory challenges during development. Mindfulness and acceptance training have been shown to support psychological flexibility, a self-regulatory skill that potentially improves adolescent adherence to medication. We assessed the effect of weekly group-based mindfulness and acceptance training sessions on ART adherence among older adolescents (15–19 years) in Kampala, Uganda. One hundred and twenty-two AWH (median age 17, range 15–19 years, 57% female) receiving care at a public health facility in Kampala were randomized 1:1 to receive 4 weekly 90-min group sessions facilitated by experienced trainers or standard-of-care ART services. The training involved (Session 1) clarifying values, (Session 2) skillfully relating to thoughts, (Session 3) allowing and becoming aware of experiences non-judgmentally, and (Session 4) exploring life through trial and error. At baseline, postintervention, and 3-month follow-up, psychological flexibility was measured using the Avoidance and Fusion Questionnaire for Youth (AFQ-Y8), and self-reported ART adherence was assessed using the Morisky Medication Adherence Scale (MMAS-8). At baseline, the intervention and standard-of-care arms had similar psychological flexibility (AFQ-Y8 score:15.45 ± 0.82; 15.74 ± 0.84) and ART adherence (MMAS-8 score: 5.32 ± 0.24; 5.13 ± 0.23). Retention through the study was moderate (71%). Completion of mindfulness and acceptance training was associated with a significant reduction in psychological inflexibility at the 3-month follow-up (AFQ-Y8 score: 12.63 ± 1.06; 14.05 ± 1.07, P = .006). However, no significant differences were observed in self-reported adherence to ART at the 3-month follow-up (MMAS-8 score: 5.43 ± 0.23; 4.90 ± 0.33, P = .522). Group-based mindfulness and acceptance training improved psychological flexibility in this population of adolescents on ART in Uganda but did not significantly improve ART adherence. Future research should explore integrated approaches that combine behavioral management training with other empowerment aspects to improve ART adherence among AWH.
Introduction
Antiretroviral therapy (ART) has improved HIV treatment and changed the face of a once deadly infectious disease to a manageable chronic condition.1,2 Antiretroviral therapy can effectively suppress the HIV viral load, improve the immune function, and control the risk of opportunistic infections, thus, enabling a stable and healthy life for people living with HIV/AIDS (PLWHA). 3 To maximize the clinical benefits of ART, adherence to the treatment plan is important. 3 Successful ART programs are highly dependent on optimal adherence and sustained care engagement 4 ; further, slowed progression to AIDS, sustained viral load suppression (VLS), reductions to ART resistance, and lengthened survival rates are all achieved through maintenance of a >95% daily oral dosing of ART. 5
While the benefits of ART in the treatment of HIV are well known, adherence to treatment plans remains a challenge among PLWHA,1,6,7 particularly among adolescents with HIV (AWH),8–10 who are approximated to be 1.7 million in number globally. 3 Adherence to ART is even poorer among older adolescents (15–19 years). 11 Older AWH interrupt treatment more often than adults, are more difficult to retain in care compared to young adolescents (10–14 years), 12 and are at a higher risk of HIV-related mortality. 3 In Uganda, an estimated 170,000 young people are living with HIV, 13 of which about 90% have acquired it vertically through their parents and 10% through sexual exposure, 14 yet they are also the only group where HIV-related mortality is on the rise, amidst a decline in other groups such as children and adults with HIV.15–17 Of the individual, interpersonal, community, and health systems challenges, the increase in HIV-related mortality is largely attributed to lapsed adherence to ART.16,18,19 Young people are less adherent to medical regimens compared to adults 8 and those with vertically acquired HIV report poorer adherence than those with behaviorally acquired HIV. 14 Studies using VLS data, a key indicator of medication success among PLWHA, show that in 2017, only 39.6% of young people in Uganda achieved VLS, compared to 74.2% of adults. 20 Several other studies have also reported lapsed adherence to ART among AWH in Uganda.15,17,21,22
Adherence to ART is affected by several variables ranging from socio-economic factors such as poverty and lack of food, psychosocial and individual factors such as discrimination, stigma, anxiety, and mode of transmission to treatment-related factors such as late initiation, long-term use, pill burden, and drug fatigue.18,23–25 In addition to the structural factors that might be beyond individual control, lapsed adherence to ART among AWH is further attributed to the developmental changes at the onset of puberty which affects health-seeking behaviors.2,26
Adolescence as a life stage influences perceptions, beliefs, attitudes, and evaluations of the severity of disease 27 and, is marked with heightened vulnerability to risk, reckless behaviors, and insecurities.28,29 Concurrently, adolescence coincides with changes in the social environment, such as spending more time with peers, as well as an increase in autonomy. 30 For AWH, adolescence also means taking personal responsibility for one's health.29,31 When such unprecedented life changes combine with the stigma that arises out of living with HIV, AWH experience cognitive dissonance characterized by self-hate, blame, entanglement with thoughts (cognitive fusion), and obsessing about the suppression of negative thought experiences (experiential avoidance). 32 Since the mind is the doorway through which individuals experience life events, 33 such mental experiences affect psychosocial pathways to care among AWH.31,34–36
Individual attributes such as self-control and emotion regulation help build resilience which is needed when dealing with challenges that accompany living with a chronic condition.33,37,38 However, during adolescence, such executive attributes are still underdeveloped, which presents self-management challenges that affect health-seeking behaviors among AWH. 39 Thus, interventions that promote self-regulation can benefit AWH.19,40 Furthermore, such approaches should also be able to promote resilience and self-acceptance which are functional responses that influence mental health and HIV treatment outcomes. 19
Mindfulness and acceptance-based interventions (MABIs) have the potential to promote self-regulation, resilience, and self-acceptance among young people41,42 through a mechanism called psychological flexibility, the ability to live consciously aware of life challenges but deliberately making choices that are personally meaningful.43–45 MABIs, through targeting psychological flexibility, address cognitive fusion (a state where individual behaviors are dominated by particular thoughts) and experiential avoidance (obsessing about suppressing negative thoughts),41,46 processes that can impact adherence to medication among young people.32,47 Furthermore, there is growing evidence that directly connects psychological flexibility to adherence to lifelong treatments.48,49 Psychologically flexible people deal with unpleasant experiences associated with daily treatment openly and elaborately, making choices that serve personal values rather than suppressing such experiences.49–52 To improve adherence to ART among AWH, approaches that promote behavioral management skills such as MABIs need to be evaluated and possibly included in the standard-of-care (SOC) offered to AWH.
One particular model based on mindfulness and acceptance philosophy that is specifically designed for young people is the Discoverer-Noticer-Advisor-values (DNA-v) intervention. The DNA-v is derived from Acceptance and Commitment Therapy (ACT), which is a cognitive behavioral approach that helps people relate better with painful and unhelpful thoughts and experiences over which they may have little or no control.32,53 The DNA-v uses age-appropriate metaphors, language, and techniques to support the development of 3 functional classes of behavior coined in the acronym DNA: the Discoverer involves learning to explore the world through trial and error, the Noticer involves developing better awareness and self-awareness, and the Advisor involves becoming familiar with and developing a relationship with one's inner voice. 41 All 3 behaviors promote psychological flexibility and work in service of values. 41 The DNA-v can be offered as individual therapy, one-on-one sessions between the provider and the client focused on individual needs, or as group therapy involving 2 or more clients focusing on common concerns. 41 In HIV treatment and care, group programs are encouraged because they promote experience sharing, reduce stigma, and improve self-esteem. 54
Interventions based on mindfulness and acceptance philosophies have growing evidence supporting the mental health of people living with chronic conditions55–57 including adolescents.58–60 However, literature linking such psychotherapies to adherence to medication among people with HIV is lacking. Thus this study aims to evaluate the effect of the DNA-v model on improving adherence to ART among AWH through an open-label group treatment trial. We hypothesize that the intervention group will report higher psychological flexibility and improved adherence to ART at the end of the trial.
Methods
Study Design and Setting
We conducted an open-label group treatment trial with individuals randomly assigned to either the DNA-v intervention or to the current SOC procedures and collected data on self-reported ART adherence and psychological flexibility at 3 time points: baseline, 4 weeks postintervention, and at 3-month follow-up. Participants were recruited from Kisenyi Health Center IV (KHC), an urban public health facility in the Kisenyi zone, Rubaga division of the Kampala district. The KHC is administratively managed by the Kampala Capital City Authority and serves a catchment population of about 1 million people within the central business district. The KHC offers free HIV care services and serves approximately 590 AWH.
Participants
The participants were older adolescents receiving care at the KHC. Inclusion criteria were: (a) being 15–19 years old, (b) an HIV-positive diagnosis, (c) attending care at the participating study clinic, and (d) the ability to speak and understand Luganda or English (the most commonly spoken languages in Kampala City). AWH with cognitive impairments or disabilities, those planning to move out of the catchment area during the study period, or those participating in an HIV care study were excluded. Recruitment of participants began on 1 November 2022 and ended on 3 December 2022.
Procedures
Once administrative clearance was offered by the city authority, we were able to access anonymous medical records to screen participants for eligibility. A list of eligible AWH was generated and were contacted telephonically by clinic staff supporting the study. Adolescents who expressed interest in the study were scheduled for individual appointments to inform and obtain consent/assent which was followed by a group briefing and later baseline assessment. Participants were then randomly assigned to the intervention or control group using allocation sequences prepared by an external bio-statistician. Allocation concealment was done using sealed serialized brown opaque envelopes that were kept by the statistician.
Randomization
Participants were randomly allocated to the intervention or control group using computer-generated random numbers. The block randomization method was used for allocating AWH to the intervention or control groups and, to achieve a 1:1 randomization ratio, we used a block size of 6 with equal individuals assigned to the 2 arms per block. Participants allocated to the intervention arm received the DNA-v training and the SOC, while participants who were allocated to the control group continued with the SOC only. To minimize contamination, the research team worked closely with healthcare providers to schedule sessions on non-clinic days to reduce the possibility of unplanned meet-ups among participants, furthermore, the team also encouraged participants not to discuss the training with non-group members until it was completed. This was an open-label randomized study because healthcare providers (counselors at the adolescent clinic) participated in recruitment, administration of the intervention, and the assessment of outcomes. The intervention flow process is shown in Figure 1.
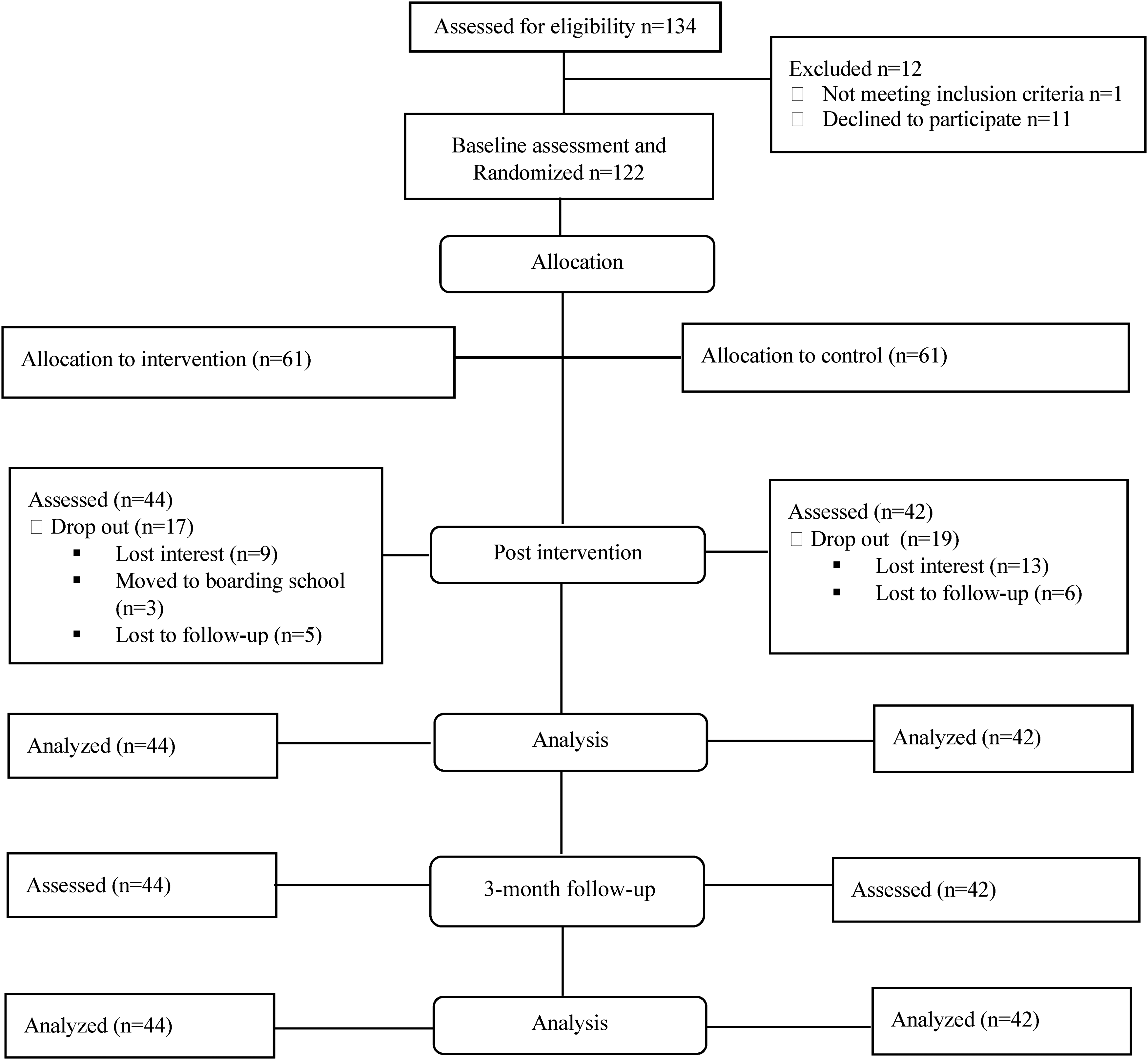
Flow diagram of the intervention process.
Study Intervention
The DNA-v
The DNA-v intervention was delivered to AWH as life skills training responding to the developmental needs of young people. 41 We split participants in the intervention arm into 4 sub-groups ranging between 11 and 12 participants. After creating sub-groups, we designed a session schedule to guide the implementation of the intervention. The first author, who is trained in using the DNA-v model, and the second author, who is trained in the therapeutic use of mindfulness and acceptance, delivered 4 90-minute sessions to each sub-group across 4 weeks, meeting once a week at the clinic premises. We conducted measures at baseline, postintervention (at 4 weeks), and follow-up (after 3 months). Participants were reimbursed $10 (37,000 Uganda shillings) every week to compensate for their time and transport costs. The session content is detailed in Table 1.
Content and Activities of the DNA-v Training with AWH. 61
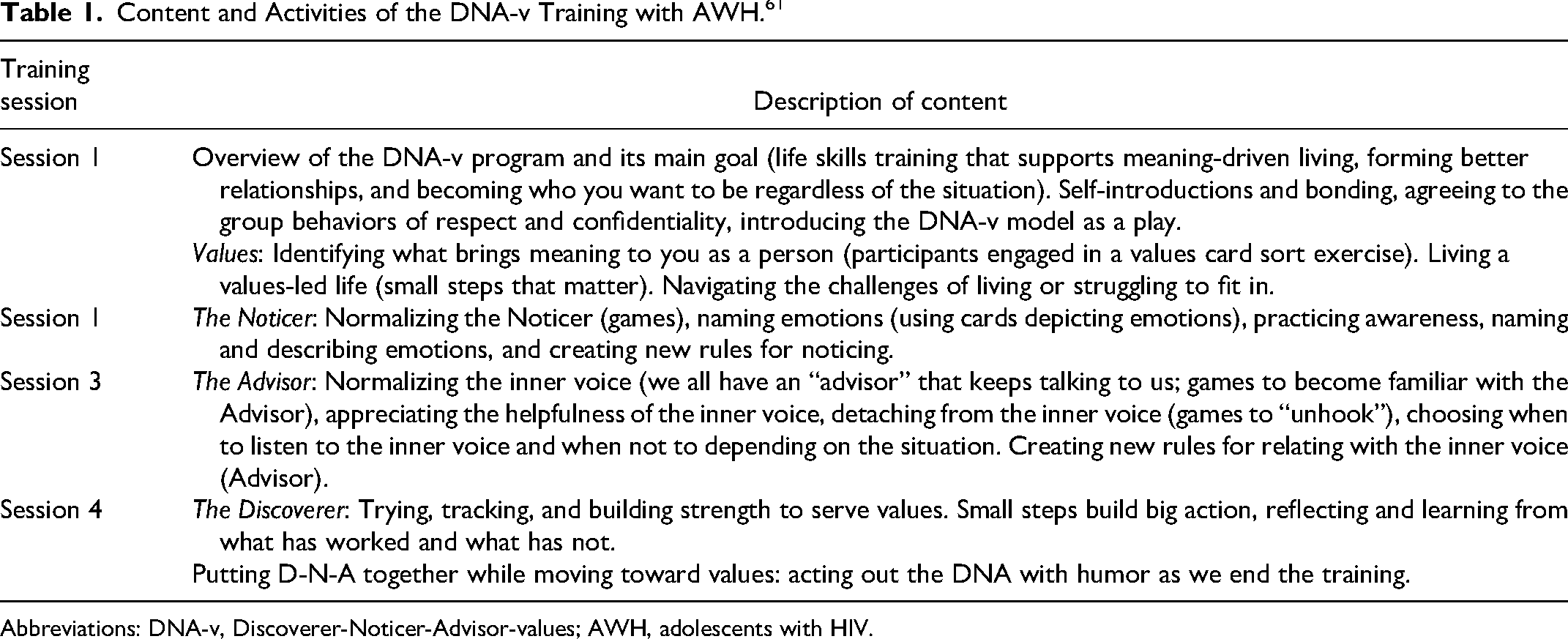
Abbreviations: DNA-v, Discoverer-Noticer-Advisor-values; AWH, adolescents with HIV.
Standard-of-Care
The SOC involved a combination of clinic-based strategies routinely used to support AWH. The services are offered during adolescent clinic days or as weekend programs by trained healthcare providers or young adolescent peer leaders. Services include psychosocial assessment (using the HEADSS tool for gathering information on home, education, eating, employment, activity, drugs, sex, sexuality, and suicidal ideation), and support (either individual or group-based, led by a healthcare worker to discuss disclosure of status, stigma, discrimination, treatment, loss and bereavement, and transitioning for AWH turning 18). 62 Psychosocial support is combined with health education such as information about ART (available care packages, benefits, side effects, and managing lifelong treatment), information on growth and development such as sexual reproductive health (antenatal care, safe deliveries, and postnatal care), life skills education, counseling on substance use, nutrition services, pregnancy testing, and contraceptive methods. 62 The SOC also involved participation in teen drama clubs which often run during school holidays and intensive adherence counseling administered to AWH with ≥1000 copies/mL after ≥6 months of ART.
Measures and Outcomes
We measured adherence to ART using the Morisky Medication Adherence Scale (MMAS-8). 63 The MMAS-8 is comprised of 8 items designed to facilitate the recognition of barriers to and behaviors associated with (intentional and unintentional) adherence to chronic medication. Response options for the MMAS-8 are “yes” or “no” for items 1–7, while item 8 has a 5-point Likert response scale ranging from 0 to 4. In scoring the MMAS-8, each “no” is rated as 1 and each “yes” is rated as 0 except for item 5 which is reverse coded. Item 8 is divided by 4 when calculating a summated score. Total scores range from 0 to 8, representing low adherence ≤6, medium adherence = 6 to <8, and high adherence = 8. The MMAS-8 has demonstrated acceptable reliability when used with PLWHA (α = .66). 64
We measured psychological flexibility using the Avoidance and Fusion Questionnaire for Youth (AFQ-Y8). 65 The AFQ-Y8 is an 8-item instrument where participants rate their level of agreement with statements targeting cognitive fusion and experiential avoidance such as “my thoughts and feelings mess up my life.” The AFQ-Y8 is scored on a 5-point Likert scale underpinned by a single factor. Scores range from 0 to 24, with higher scores indicating higher levels of psychological inflexibility and lower scores indicating psychological flexibility. The AFQ-Y8 has excellent internal consistency (α = .90), and test–retest validity (r = .80) 66 and is recommended for measuring psychological flexibility among adolescents. 66
The study questionnaire was administered in either English or Luganda and the translation involved 2 bilingual native speakers of both languages. One translated the original English tool into Luganda and the other back-translated the Luganda version into English. The back-translated and original English tools were compared and inconsistencies were addressed. Both versions of the tool were then pilot tested with adolescents in another public health facility which was not part of the study.
Statistical Analysis
The sample size was based on a Swedish and Australian study on the effectiveness of ACT for adolescent mental health where a mean difference of 4.09 was considered (SD = 5.13). 67 Confidence interval and power of 80% was used leading to a sample size of 52 participants in each group. To compensate for a 10% loss to follow-up, the sample size was increased to 116 (58 in each group). Baseline characteristics were compared using the Student's t-test for continuous variables while the categorical variables were compared using the Fisher's exact and chi-square tests. We compared the intervention and control groups at 3 time points: baseline, postintervention, and 3-month follow-up. The means and standard errors of the 2 outcomes of psychological flexibility and adherence were summarized for each time point in both the control and intervention groups. We performed repeated measures analysis of variance (ANOVA) after testing for the homogeneity of variances assumption (sphericity) using Mauchly's test. We then performed the repeated measures test with a P value of .05 considered as statistical significance. We conducted post hoc pairwise comparisons of means for psychological flexibility using the Bonferonni adjustment and adjusted the P value. Participants who withdrew before the 3-month follow-up assessment were excluded from the final analysis. Analyses were conducted using SPSS version 25.0 and followed an intention-to-treat analysis approach.
Ethical Approval and Informed Consent
Ethics approval was granted by the Makerere University School of Medicine Research and Ethics Committee (Mak-SOMREC-2021-176), and the Uganda National Council for Science and Technology (HS1656ES). We also obtained administrative clearance from the Kampala Capital City Authority, the body that manages all public health centers in the city. AWH who were 18 years and above provided written informed consent while those below 18 years of age provided assent, with written consent provided by their caregivers. Caregivers were not treated as participants and did not provide study data. The consent form was in both Luganda and English languages and participants were given sufficient time to read or be read the form in their language of preference and to ask any questions. The consent/assent process was conducted in a private room at the clinic with a healthcare provider present to witness that participation was voluntary.
Study methods and results followed the 2010 CONSORT checklist for reporting parallel group randomized trials. 68 The study protocol was registered on ClinicalTrials.gov (NCT05010317) and a full study protocol is available from the corresponding author.
Results
Description of the Study Population
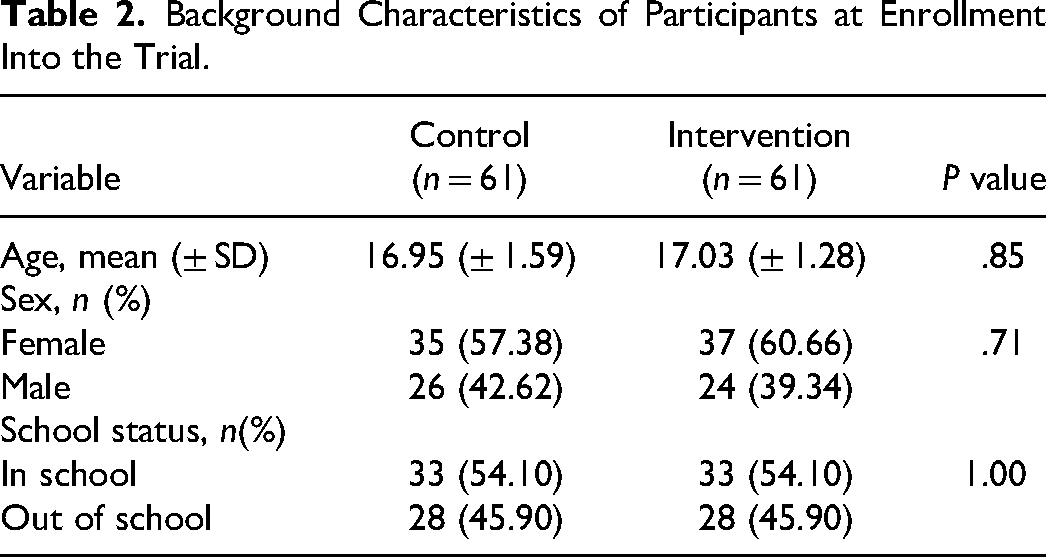
We randomly allocated 61 participants to each study arm and conducted evaluation at 3 time points (baseline, postintervention, and 3-month follow-up). The mean age of the participants, sex, and school status (whether in school or not) did not differ significantly across groups at baseline as shown in Table 2. Furthermore, the level of psychological flexibility and self-reported adherence to ART also did not differ significantly between the 2 groups at baseline, while at 3-month follow-up, significant differences were recorded in psychological flexibility but not in self-reported adherence to ART as shown in Table 3.
Background Characteristics of Participants at Enrollment Into the Trial.
Group Comparisons at 3 Time Points Using Repeated Measures ANOVA.
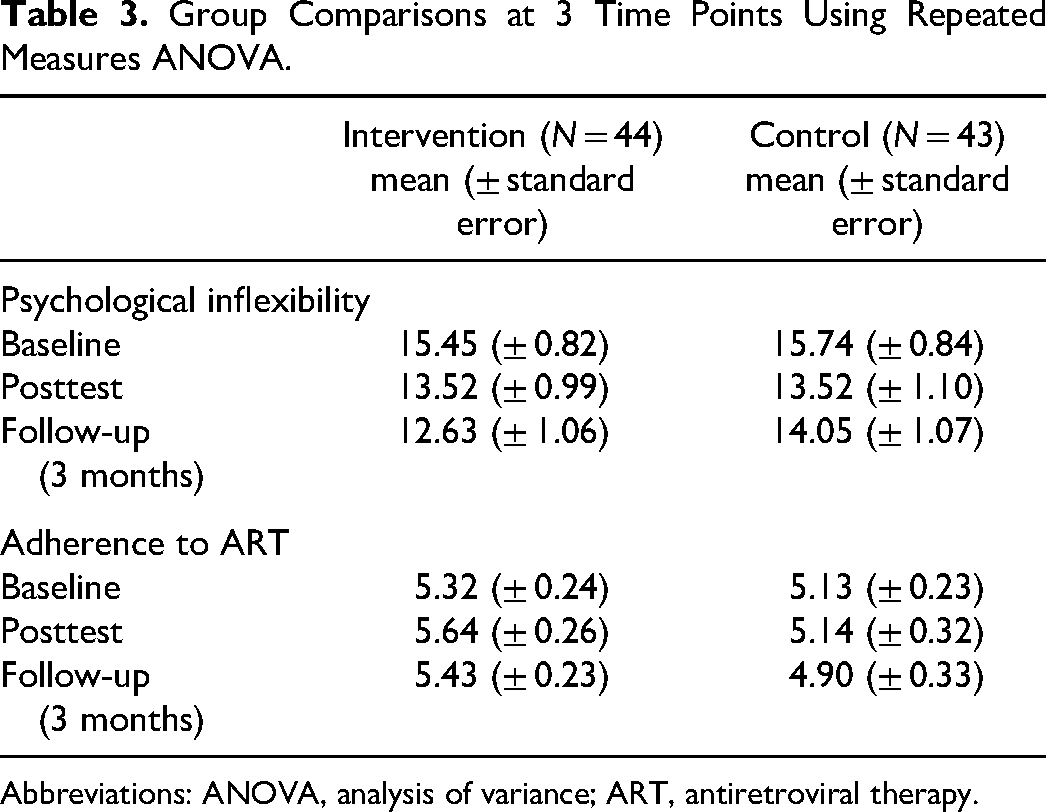
Abbreviations: ANOVA, analysis of variance; ART, antiretroviral therapy.
Outcome Measures
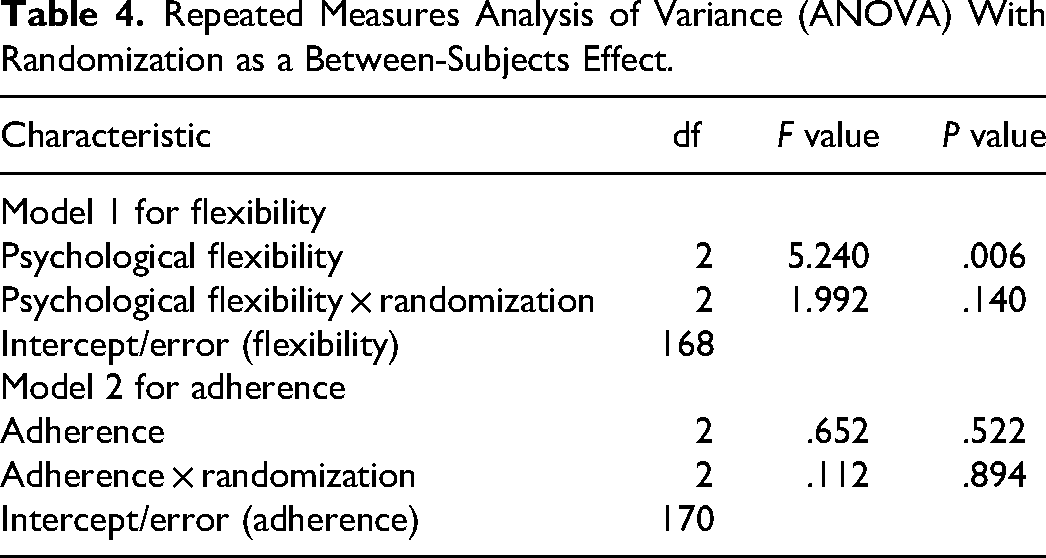
From the repeated measures analysis, we found that there was a significant difference in mean scores for psychological flexibility across the 3 time points (F = 5.240, P = .006) as shown in Table 4. For adherence, there was no statistically significant difference between mean scores across the 3 time points irrespective of the initial randomization (F = 0.652, P = .522) as shown in Table 4. We further performed a post hoc analysis for psychological flexibility as shown in Table 5.
Repeated Measures Analysis of Variance (ANOVA) With Randomization as a Between-Subjects Effect.
Post hoc Pairwise Comparisons of the Psychological Flexibility Means Using the Bonferroni Adjustment.
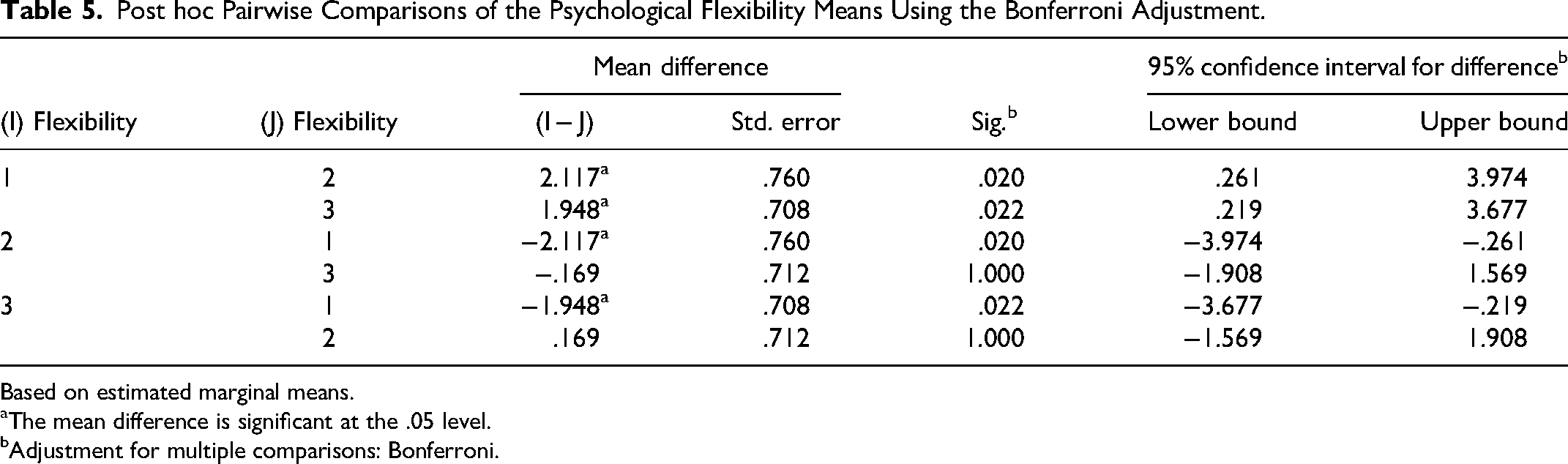
Based on estimated marginal means.
The mean difference is significant at the .05 level.
Adjustment for multiple comparisons: Bonferroni.
For psychological flexibility as a mechanism of change underlying MABIs, in the intervention arm, we found that Mauchly's test for sphericity was fulfilled with P = .761. We performed post hoc pairwise comparisons of the means using the Bonferroni adjustment, which showed that there was a significant difference between the baseline psychological flexibility mean scores and postintervention scores (15.45, 13.52, P = 0.020) and also baseline psychological flexibility scores and follow-up scores (15.45, 12.63, P = .022) as shown in Table 5. There were no significant differences noted between the comparison of the mean scores between the postintervention scores and 3-month follow-up scores (13.52, 12.63, P = 1.00) as shown in Table 4. In the control arm, we found that Mauchly's test for sphericity was fulfilled with P = .368. Repeated measures ANOVA determined that mean psychological flexibility did not differ significantly across the 3 time points (F = 1.991, P = .140) as shown in Table 4. No post hoc comparisons of the means were performed for this group.
For adherence to ART, overall, there were no significant differences between the intervention and control arms at all 3 time points. In the intervention arm, we found that Mauchly's test for sphericity was fulfilled with a P = 1.00. Repeated measures ANOVA determined that mean adherence did not differ significantly across the 3 time points (F = 0.652, P = .522) as shown in Table 4. No post hoc pairwise comparisons of the means were performed using the Bonferroni adjustment. Similarly, in the control arm, Mauchly's test for sphericity was fulfilled with a P = .813. Repeated measures ANOVA determined that mean adherence did not differ significantly across the 3 time points (F = 0.112, P = .894), and no post hoc pairwise comparisons of the means were performed.
Discussion
In this study, we evaluated the effect of the DNA-v on psychological flexibility and adherence to ART among AWH. Results from the study contribute to the evidence that is needed to support the integration of mindfulness and acceptance-based strategies into care services offered to AWH in Uganda. We compared the effect of the DNA-v to the SOC on improving psychological flexibility and self-reported adherence to ART among older AWH (15–19 years) receiving care at an urban clinic in Kampala. We hypothesized that participants receiving the DNA-v intervention would report higher levels of psychological flexibility and improved adherence to ART at postintervention and 3-month follow-up compared to the SOC group. Results from the study show that the intervention group reported higher levels of psychological flexibility as hypothesized, however, both groups did not differ significantly in self-reported adherence. That is, results suggest that the DNA-v as an MABI has the potential to improve psychological flexibility among AWH but does not necessarily result in improved adherence to ART. To our knowledge, this is the first study to test the effect of the DNA-v on improving psychological flexibility and adherence to ART among AWH in a low-resource context through a controlled trial. Although similar studies have used MABIs with adults living with HIV and have tested for mental health outcomes, 69 studies conducted with AWH are rare and highlight our critical contribution to the literature.
Higher levels of psychological flexibility reported in the intervention group but not in the control group at the follow-up stage indicate that psychological flexibility as a self-regulation skill can be trained and improved among AWH. This observation is important for HIV treatment and care of AWH who experience developmental changes that require enhanced levels of self-management for coping. Psychological flexibility denotes becoming open to life experiences non-judgmentally, dealing with difficult situations with awareness, and deliberately making choices that bring meaning to an individual.32,44 Since living with HIV presents numerous challenges, developing skills that help one approach challenges with openness, is therapeutic. Our findings are consistent with literature that identifies psychological flexibility as a skill that can improve with time through deliberate training or psychotherapy.43–45 Moreover, the results concur with studies that found improved levels of psychological flexibility among adolescents who were exposed to DNA-v training.42,67 By improving psychological flexibility among AWH, our results confirm that MABIs are transdiagnostic and can address a range of emotional and behavioral challenges across conditions. 70
The study did not find a significant difference between groups on self-reported adherence to ART. Results suggest that while the DNA-v training could have helped AWH develop self-regulatory skills by improving psychological flexibility, such a transformation did not impact adherence to ART. This could mean that adherence to ART among AWH is influenced by a range of factors that may extend beyond behavioral regulation. The study findings diverge from the literature that suggests that through psychological flexibility and values clarification, MABIs help patients make active treatment choices including adhering to treatments. 71 Results further deviate from research findings indicating that interventions that promote self-efficacy and self-acceptance which are core components of psychological flexibility result in improved adherence among people with HIV. 72 Furthermore, results do not align with studies that found ACT to yield improved adherence to medication among patients with chronic conditions. 73 Nevertheless, it is worth noting that while MABIs may empower patients to make values-consistent choices such as adhering to a treatment regimen, such individual-level choices may be compromised by high-level social and economic factors that impact the entire cascade of care. In low-resource settings such as Uganda, factors such as abject poverty limit access to food, while high levels of stigma and discrimination are suffered at home, in the community, and at school due to misconceptions about HIV. The far distances to health centers are an access barrier, while unreliable family support due to the loss of biological parents, and school arrangements which limit privacy 15 may affect health-seeking choices AWH make regardless of their levels of resilience. This may partially explain why the vast majority of studies reporting a positive association between mindfulness and acceptance skills and medication adherence have been conducted in resource-rich contexts.
The study findings, however, are consistent with the literature which highlights that behavioral change approaches that target adherence often register limited success. 74 The findings are also in line with the literature that suggested that PLWHA interventions that promote psychological flexibility only improve overall well-being but do not explain intentional or unintentional non-adherence to ART. 69 Furthermore, our results confirm earlier findings that adherence to ART is affected by a range of factors that may go beyond individual control and have the power to compromise individual choices or meaning. 75
Although there were no significant differences between groups on self-reported adherence to ART, within-group mean differences showed that participants in the intervention arm had improved adherence scores at posttest and 3-month follow-up adjusting for baseline scores compared to the SOC group. As adherence is a salient challenge among AWH, this minor improvement is still promising and can inform follow-up studies. Furthermore, since the study is based on self-reported measures which can be subject to bias, more objective measures such as pill counts or electronic monitoring systems could provide alternative findings. This observation is supported by a systematic review that found large–medium effect sizes among studies that measured adherence by pill count or electronic event monitoring systems. 74 Nevertheless, subjective assessments are still valid measures of adherence and have widely been used across HIV studies.64,76
Strength and Limitations
The study had notable strengths. First, randomizing participants helped to balance the study groups and thus controlled for possible confounders that could have affected the interpretation of the results. The use of this rigorous design lowered the risk of bias, which is critical when generating evidence that can influence the uptake of health interventions. Secondly, adding a follow-up period to the study was another strength. The 3-month follow-up helped to gauge whether the impact of the intervention could be sustained.
Notwithstanding these strengths, the study had some limitations. Foremost, the results may have been affected by the high rate of attrition, given that more vulnerable participants may have dropped out. However, since groups were almost equivalent at baseline and attrition did not differ significantly between conditions at 3-month follow-up, its effect is likely to be minimal. Nevertheless, smaller numbers in randomized conditions could still provide useful insights. Furthermore, while our 3-month follow-up is still considered sufficient to identify consistency in the behavioral patterns, multiple follow-up assessments (eg, at 6, 9, and 12 months) would have given a clearer picture of the sustainability of the intervention effect. Taken together, the study provides a starting point for future studies with larger samples and longer follow-ups to generate additional evidence.
Conclusion
Adherence to ART remains a significant challenge among AWH and may best be addressed by a comprehensive strategy that incorporates various components of care. The results from this study demonstrate that while an MABI for young people did not improve self-reported adherence to ART among AWH, it led to improvements in levels of psychological flexibility. Although adherence was the primary outcome measure, improvements in psychological flexibility are promising for addressing care concerns that may improve adherence in the long run. Given that psychological flexibility represents a set of self-regulation components (self-acceptance, self-efficacy, and resilience), strengthening it as a skill among AWH can result in better clinical outcomes. Since the literature connecting MABIs to adherence to ART among adolescents is still in its infancy, future studies are needed with larger samples, and longer follow-up periods evaluating psychological flexibility as a mechanism of change underlying MABIs with objective measures of adherence.
Footnotes
Acknowledgments
The authors wish to thank Louise Hayes, Joseph Ciarrochi, and Ann Bailey for permitting us to use the DNA-v model. We also thank the Institution for Adherence for licensing the use of the adherence scale, the management and staff of Kisenyi Health Center IV in Kampala for allowing the study to be conducted there, the adolescents who participated in the study, the Makerere University Behavioral Social Science project (Mak-BSSR), and the research team: Kelly Gonzaga Kyagaba, Joseph Balikuddembe, and Hope Kirabo.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fogarty International Center (FIC), the National Institute of Alcohol Abuse and Alcoholism (NIAAA), and the National Institute of Mental Health (NIMH), of the National Institutes of Health (NIH) under the Award Number D43 TW011304. The study was also supported by the Makerere University Research and Innovations Fund (Mak-RIF). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (![]()