
Abstract
Women living with HIV (WLWH) experience depression, anxiety, and posttraumatic stress symptoms at higher rates than their male counterparts and more often than HIV-unaffected women. These mental health issues affect not only the well-being and quality of life of WLWH, but have implications for HIV management and transmission prevention. Despite these ramifications, WLWH are under-treated for mental health concerns and they are underrepresented in the mental health treatment literature. In this review, we illustrate the unique mental health issues faced by WLWH such as a high prevalence of physical and sexual abuse histories, caregiving stress, and elevated internalized stigma as well as myriad barriers to care. We examine the feasibility and outcomes of mental health interventions that have been tested in WLWH including cognitive behavioral therapy, mindfulness-based interventions, and supportive counseling. Future research is required to address individual and systemic barriers to mental health care for WLWH.
What Do We Already Know About This Topic?
Individuals living with HIV are at high risk for mental health concerns including stress, depression, and PTSD, that can detrimentally impact their self-care and management of HIV.
How Does Your Research Contribute to the Field?
This article increases awareness of the burden and contributing and sustaining factors of mental illness specific to women living with HIV, along with research on mental health treatments for this population.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
This article demonstrates the need to expand the research and dissemination of evidence-based mental health treatments for women living with HIV.
Overview and Epidemiology of Mental Illness Among WLWH
There are over 17 million women worldwide and a quarter million women in the U.S. living with HIV. 1 Women constitute over half of individuals living with HIV globally 2 and nearly a quarter of those living with HIV in the U.S. 3 Women living with HIV (WLWH) are more likely to have comorbid mental health conditions, 4 concurrent mental and physical health comorbidities, 5 and worse overall mental health, 6 than men living with HIV and HIV-negative women. 7 This may be due, in part, to women with mental illness being in vulnerable positions associated with HIV acquisition (e.g., including intimate partner violence, inconsistent condom use, bartering sex, history of other sexually transmitted infections) as compared to women without mental health problems. 8 Alternatively, HIV diagnosis may lead to mental illness symptomatology or exacerbate existing mental illness symptoms for women due to stigma and psychological stress associated with disease management. For example, women experience more than 3 times as many mental health issues after, as compared to before, their HIV diagnosis. 9 Thus, established gender disparities in mental health conditions including depression, 10 anxiety, 11 and posttraumatic stress disorder 12,13 may be exacerbated in the context of HIV. 9 Women also tend to be diagnosed with and begin receiving treatment for HIV in later stages of infection than men 14 and the prevalence of neuropsychiatric issues increases in later stages of HIV infection. 15 In addition, HIV disparities associated with gender, race/ethnicity, poverty, and rural location, along with their intersectionality, may also contribute to poor mental health among WLWH.
Psychiatric illness among WLWH has been linked to worse antiretroviral therapy (ART) medication adherence and medical appointment attendance, 16 -19 which may play a role in health-related quality of life. Given the prevalence of co-morbid HIV and mental illness alongside the clinical ramifications of this intersectionality, our objective was to synthesize the current understanding of the specific mental health problems experienced by WLWH along with the implications on overall health. Furthermore, we sought to describe existing interventions tailored to this vulnerable population and identify areas for future research. We included special sections on pregnant and parenting WLWH due to the distinct clinical implications for behavioral health among this population.
Method
For this narrative review, we conducted a comprehensive literature search using PUBMED, Cochrane Library, and PsycINFO databases. The search terms were “Women* or female* or girls* or pregnant* or perinatal* or postpartum*” AND “HIV* or AIDS* or human immunodeficiency virus* or acquired immunodeficiency syndrome*” AND “mental illness* or mental health* or psychiatric* or depression* or mental health intervention* or psychosocial intervention* or therapy* or mental health treatment* or depression treatment*.” All relevant papers were identified and reviewed for inclusion criteria by 2 members of the research team (EMW and VW). We included papers that reported on 1) WLWH, including women of trans experience, and 2) psychological health or illness and/or therapeutic or psychosocial interventions specifically designed to address mental illness among WLWH. We excluded papers that did not explicitly report results for WLWH and those that reported only on neurodegenerative or neuropsychiatric conditions to limit the scope of the review to the most prevalent mental health conditions faced by WLWH. Articles that met these criteria were included and described in this narrative review.
Ethical Approval and Informed Consent
Ethics approval was not required for this narrative review.
Stress and Stigma Among WLWH
WLWH face unique stressors that contribute to mental health issues. A meta-analysis of studies looking at stress and coping among WLWH found that perceived health status and functional limitations are major sources of stress despite the widespread availability of ART. 20 Around the world, many women face issues with access to and acceptability of community-based health services for HIV. 9,21,22 Following receipt of an HIV diagnosis, women report stress over their interpersonal relationships, disclosure of their HIV status, 23 and management of their sexual and reproductive health. 9,24 In addition, WLWH from low, mid, and high-income nations tend to have higher rates of intimate partner violence than the general population, 25,26 which is linked to poor mental health. 25
In the U.S., more than four-fifths of WLWH are racial/ethnic minorities. 2 Ethnic/racial minority WLWH have reported higher levels of perceived stress than the general population, 27 potentially due to the intersection of health status, race, poverty, health care accessibility, and gender-based discrimination. 9,28 The experience of racism may also contribute to HIV-related stigma in women. 29 WLWH in the U.S. and Canada report higher levels of HIV stigma than men with HIV. 30,31 WLWH exist within several intersections vulnerable to stigma: first, as persons living with HIV; second, as persons with much higher risk for mental health issues or symptoms which may be worsened by HIV as a stigmatized illness; third, as women; fourth, (if applicable) as racial and ethnic minorities. Stigma, discrimination, and social prejudice negatively impact the social and psychological health and well-being of persons living with HIV; They are associated with low social support, poor physical and mental health, and a poorer quality of life, and can delay or impede their getting help and treatment for mental health concerns and/or HIV. 32,33 Perception and internalization of HIV stigma is associated with greater depressive symptoms and poorer psychological adjustment to HIV diagnosis and management. 17,34 -36 For example, a longitudinal study of Black, African American, and Caribbean WLWH in Canada found a significant correlation between HIV-related stigma, gender-based discrimination, racism, and depression. 37 More broadly, stigma associated with HIV has been linked to anxiety, depression, poor self-esteem, and poor adherence to care. 38 The combination of WLWH’s physical, functional, interpersonal, and systemic stressors likely contributes to the burden of mental health issues in this population, including depression, trauma-related symptomatology, and anxiety.
Mental Health Conditions of Women Living With HIV
Depression
Depression is prevalent among WLWH. Studies conducted in the U.S. show that, compared to HIV-seronegative women, rates of major depressive disorder diagnoses are 4 times as high in WLWH 39 and WLWH experience significantly worse depressive symptom severity. 27,39,40 Further, symptoms of depression are highly prevalent; they were endorsed by 82% of respondents in a study of WLWH from 94 countries. 9 U.S. WLWH have rates of depressive disorder and symptoms up to twice as high as men living with HIV 4,41,42 and WLWH in Iran and the U.S. report more severe depressive symptomatology. 43 -45 Of concern, depressive disorders among individuals living with HIV is often underdiagnosed, particularly for women 46 and it is estimated that less than half of U.S. WLWH are adequately treated for depression. 47
Studies conducted in the U.S. have found that depression among WLWH is associated with challenges with interpersonal relationships. For example, depressive symptoms in WLWH is associated with lowered functioning within their families and a decreased ability to fulfill responsibilities at home. 40 There is a negative correlation between depression and disclosure of HIV-positive status 48 and perceived social support. 48,49 Thus, depression among WLWH can worsen social isolation, perpetuating and exacerbating the depressive symptoms and disorder.
Depressive disorders among WLWH globally are associated with an increased health burden including greater HIV disease progression, more severe HIV-related symptomatology, and increased mortality. 50 -56 In a 7-year longitudinal study of 765 WLWH from the HIV Epidemiology Research Study in the U.S., Ickovics and colleagues found that, after controlling for clinical and treatment factors, women with chronic depressive symptoms experienced significantly greater declines in CD4 counts than those without chronic depressive symptoms and were twice as likely to die than women with minimal to no depressive symptoms. 41 Similarly, data from the U.S. multi-site Women’s Interagency HIV Study (WIHS) also found that chronic depression was associated with greater HIV disease progression and mortality. 57 In fact, analyses of WIHS data showed that the association between depressive symptoms and mortality was greater in magnitude than the association between failing to initiate ART and mortality, and hazard of death for depressed women not on ART was over 7 times that of non-depressed women on ART. 54 Symptoms of depression include disrupted memory, concentration, appetite, and sleep—all factors that can contribute to alterations in sleep/wake cycles or medication administration in relation to meals. These data underscore the need to aggressively identify and treat depressive symptoms when present as a means to optimize HIV-related care.
The impact of depression on HIV disease progression and mortality among WLWH may be multifaceted. 58 Depression can negatively affect the immune system, with several possible mechanisms having been postulated including chronic inflammation. HIV induces immune activation in the brain which may lead to tryptophan depletion and a resultant reduction in serotonin, thus exacerbating or maintaining depressive symptoms. 59 In addition, several behavioral consequences of depression can impact HIV health outcomes. International studies have shown that depressive symptomatology impedes the activation required to begin and maintain antiretroviral medication and disease management. 16,17 Symptoms of depression that may act as potential barriers to medication and disease management include feeling helpless, disempowered, and negativistic, 17 difficulty concentrating, 16 fatigue, poor sleep 60 and the tendency for self-neglect. 61 In studies conducted in the U.S., Turan and colleagues found that for WLWH, depression mediates the relationship between internalization of HIV stigma and lower ART adherence, in part through decreased social support and increased loneliness, a relationship that was particularly strong for Hispanic and non-Hispanic Black women. 17,36
Trauma-Related Mental Health Issues
Depression and trauma are closely linked in WLWH globally. 62 Studies from the U.S. have found a strong association between history of childhood trauma, intimate partner violence, and depression among WLWH. 63,64 WLWH from low, mid, and high-income nations report high rates of exposure to traumatic events, especially intimate partner violence, 26 and posttraumatic stress symptoms. 63,65 -67 In fact, a meta-analysis of psychological trauma and posttraumatic stress disorder (PTSD) in WLWH in the U.S., Western Europe, Scandinavia, Australia, and New Zealand found that approximately 70% of study participants reported experiencing abuse in their lifetimes and 30% had recently experienced PTSD, more than 5 times the rate for recent PTSD among women in the general population. 68 Additionally, a study of 1223 HIV-positive mothers recruited from 22 sites across the U.S. reported that 23% of the sample met screening criteria for PTSD. 69 Of note, the study found that the majority of HIV-positive mothers with comorbid psychiatric disorders at screening, especially a combination of PTSD, depression, and/or anxiety, still met criteria for 1 or more of these disorders 1 to 3 years later and only 4.5% were receiving mental health treatment at screening. 69
Traumatic experiences have been shown to have deleterious effects on the mental and physical health of WLWH. 63,70,71 According to studies conducted in the U.S., greater posttraumatic stress symptomatology has been linked to lower T-cell counts in WLWH 65 and experiencing more traumatic events is associated with worse medication adherence, greater likelihood of virologic failure, 72,73 and higher HIV-related mortality. 74 Findings from a systematic review and meta-analysis found that WLWH with a history of intimate partner violence had significantly lower odds of using and adhering to ART and achieving viral suppression. 19 Further, trauma has been implicated in high-risk acquisition or transmission behavior for women with or at risk for HIV infection internationally. 75 -80 Given the high prevalence of depression and trauma in WLWH, their shared association with HIV disease progression and transmission are of critical concern.
Anxiety
In addition to depression and posttraumatic stress symptomatology, prior research has found that WLWH report more severe anxiety symptoms than HIV-negative women. 27,39 Clinical levels of anxiety have been reported as high as 40% in the U.S. and Canada. 81,82 Anxiety disorders and severe anxiety symptomatology tend to be more common among WLWH than in men living with HIV as reported in studies from the U.S. and Iran. 4,45 Anxiety in WLWH may be related to HIV-related stigma. 82 For women of reproductive age, worries over reproductive health concerns such as fear of perinatal transmission and perceived judgment regarding reproductive desires may also be a source of anxiety. 82 Anxiety among individuals living with HIV has been shown to be related to disease progression and lead to worse quality of life. 83 A summary of common mental health conditions among WLWH can be found in Table 1.
Summary of Research Findings on Common Mental Health Conditions Among Women Living With HIV.

HAART: Highly Active Antiretroviral Therapy; ART: Antiretroviral Therapy; PTSD: Posttraumatic Stress Disorder; PTSS: Posttraumatic Stress Symptoms.
Mental Health Among Pregnant, Postpartum, and Mothers Living With HIV
Pregnant and postpartum WLWH face additional challenges with potential attendant mental health consequences. Pregnancy and the postpartum period are times of significant biological, social, and psychological changes for women 84 and women are at increased risk for depression, anxiety, obsessive compulsive disorders, and postpartum psychosis in this window. 85,86 Many WLWH must also confront perceived stigma from obstetric providers, disclosure of HIV-status as it is related to the pregnancy, and stress regarding prevention of perinatal HIV transmission, a study from Uganda found. 23 Moreover, violence and abuse do not abate with pregnancy or birth. One prospective cohort study of pregnant WLWH in the U.S. found that 9% experienced partner abuse or violence during pregnancy or the postpartum. 87 A U.S.-based study reported that women who experienced intimate partner violence during pregnancy have poorer ART adherence and take longer to achieve viral suppression. 88
Prior international research has found more severe perinatal depressive symptoms in WLWH with worse perceived social support, stress, and internalized stigma. 29,49,89,90 While not all study findings are uniform (see, for example, 91 -93 ), some U.S. studies have found heightened levels of depression for perinatal WLWH as compared to HIV-negative perinatal women, 49,94 even after controlling for the somatic symptoms that are shared by both pregnancy and depression such as fatigue and changes in appetite. 49 Two international meta-analyses of perinatal depression in WLWH found 36-44% prevalence of antenatal depression and 21-31% prevalence of postnatal depression, assessed by positive screening or diagnostic clinical measures. 95,96 A study of 273 pregnant and postpartum WLWH at a HIV Perinatal Center in Los Angeles, found that women with a CD4 nadir less than 200 cells/mm3 were 3 times more likely to have a perinatal depression diagnosis than mothers with a CD4 count above 500 cells/mm 3 . 94 Depression and anxiety during the perinatal period have implications for self-care, care of the neonate, and prevention of perinatal HIV transmission. 97 Specifically, perinatal depression among U.S. and Kenyan WLWH has been linked to suboptimal ART adherence, substance misuse during pregnancy, 94 and lower rates of HIV care initiation. 97 A systematic review and meta-analysis of low, middle and high-income countries demonstrated that only 73.5% of pregnant women achieved optimal ART adherence. Selected barriers to adherence included depression, alcohol and drug use, and psychosocial issues. 98 A comprehensive international literature review looking at the mental health of HIV Seropostive women during pregnancy and postpartum period concluded that psychiatric symptoms, especially depression were widespread globally and clinical and structural interventions were necessary. 99
Beyond the early postpartum period, parenting WLWH face a number of stressors that can negatively affect their mental health and quality of life. Parenting WLWH must balance caregiving responsibilities with their own HIV care. 100 Among parenting U.S. WLWH, experiencing both stressful life events and parenting stress is associated with HIV treatment non-adherence, specifically missed ART doses and missed medical appointments. 18
Mental Health Treatment for Women Living With HIV
Given the prevalence of stressors and mental health conditions faced by WLWH and the connection between mental illness symptoms and suboptimal disease management, accessible and acceptable mental health interventions tailored to the unique needs of this population are crucial. Despite this need, there is a significant gap in evidence-based mental health interventions for WLWH 101 -103 and disparity in mental health care access and utilization. For example, it is estimated that less than half of depressed WLWH in the U.S. are adequately treated. 47 When the need for mental health treatment for WLWH is met, the benefits go beyond improvement in psychological symptoms. Two studies from the WIHS cohort demonstrated that mental health service usage was associated with increased use of ART and decreased mortality. 57,104 Some notable exceptions have attempted to address this gap in mental health treatment, incorporating stress management, cognitive-behavioral, and supportive modalities. These are described below.
Management of Stress
Although the research on formal psychosocial mental health interventions for WLWH is incomplete, there has been considerable research on coping among this population. Coping behaviors such as self-care, stress management, cognitive flexibility, and maintaining social support networks have been linked to better mental and physical quality of life among WLWH in the U.S. 20,27,67,105 Further, the coping behaviors of engaging in supportive relationships and positive self-appraisal are associated with psychological and spiritual growth in U.S. WLWH. 106,107 Specifically, the type of coping in which a woman living with HIV engages is predictive of medication adherence, with avoidant behaviors associated with more missed doses and active coping predictive of better adherence. 48,108 Spirituality and prayer are also coping tools that WLWH use to combat stress and distress. 20,109,110 A study of 142 Puerto Rican WLWH in New York City found that spirituality was protective against depression and that self-esteem and sense of mastery mediated the relationship between spirituality and depression. 111
Mental Health Treatment Studies: Psychosocial Interventions
Effective, acceptable, and culturally competent mental health treatments are necessary given the prevalence and specific needs of WLWH. Much research has focused on treatments that integrate psychosocial components into interventions for improving antiretroviral medication adherence, other health behaviors, or overall health, 112 as compared to interventions with the primary aim of decreasing the burden of mental illness. Of the psychosocial interventions that have been tested and reported for this population, many utilized evidence-based approaches such as cognitive behavioral therapy techniques, motivational interviewing, interpersonal effectiveness skills, and relaxation. 112 A summary of the published interventions is depicted in Table 2.
Summary of Published Mental Health Interventions for Women Living With HIV.
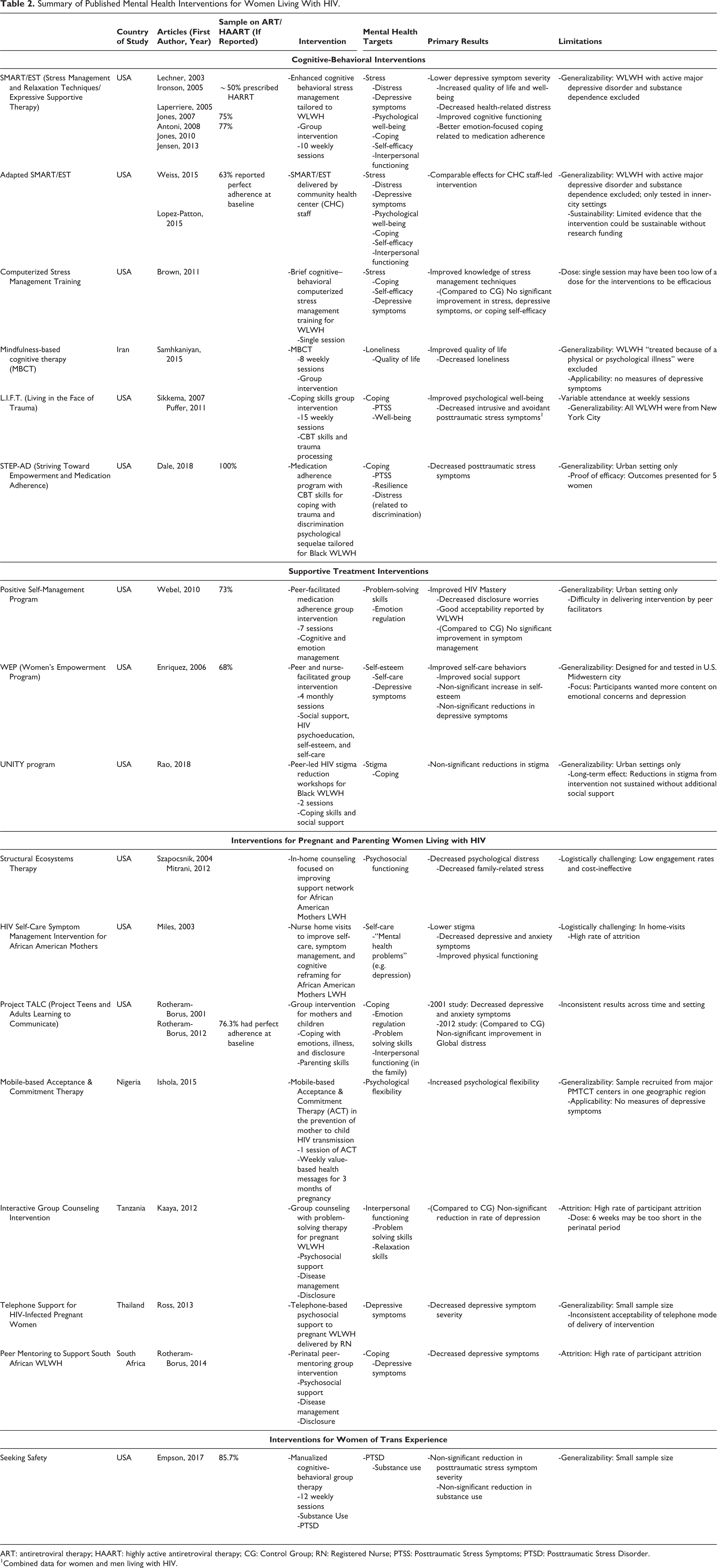
ART: antiretroviral therapy; HAART: highly active antiretroviral therapy; CG: Control Group; RN: Registered Nurse; PTSS: Posttraumatic Stress Symptoms; PTSD: Posttraumatic Stress Disorder.
1 Combined data for women and men living with HIV.
Cognitive-behavioral interventions
Cognitive-behavioral interventions for WLWH are the most frequently studied. One of the most widely disseminated is the Stress Management and Relaxation Techniques/Expressive Supportive Therapy (SMART/EST) study. 113 The SMART/EST study was a 3 stage, multi-site randomized trial designed to test the feasibility and effectiveness of enhanced cognitive behavioral stress management. The study was conducted in several U.S. regionally-diverse community health centers with participants who were ethnically representative of WLWH, including a majority African American, Latina, and Caribbean women. 114 Cognitive behavioral stress management includes cognitive-behavioral and interpersonal skills training plus relaxation tailored to the psychosocial needs of WLWH. 115 In the SMART/EST study, cognitive behavioral stress management was augmented with an expressive and supportive component in a 10-week group intervention. The intervention led to improved quality of life, including improved cognitive functioning, decreased health-related distress, 116 increased positive well-being, 117 and increased emotion-focused coping related to medication adherence. 118 Participants in the enhanced cognitive behavioral stress management intervention were found to have lower depressive symptom severity at the end of treatment and at the 1-year follow-up assessment. 119 Secondary analyses examining specific components of the SMART/EST psychosocial intervention found that women in the group intervention practicing guided imagery had lower cortisol levels at post-tests compared to pre-intervention levels. 120 Increases in CBT skills and self-efficacy were inversely correlated with viral load and depressive and anxious symptoms, 113 even 1 year after the intervention ended. 121
The effectiveness of the SMART/EST intervention was examined when led by community health center staff (versus doctoral level psychologists and post-doctoral fellows). 122 While the authors acknowledge challenges to translating their research to real-world health settings, 123 they found comparable effects between staff-led interventions and those led by the mental health professionals, 122 opening the door to non-traditional modes of this intervention. Despite its demonstrated efficacy, the SMART/EST study has limited generalizability as an intervention targeting mental health. The study excluded WLWH with active major depressive disorder. 116,118 Although women were allowed to participate in the study after receiving treatment, their initial exclusion limits the ability to draw conclusions about the SMART/EST intervention’s effectiveness as a treatment for depression. In addition, the SMART/EST intervention was only tested in inner-city community health clinics and 60% of these sites had discontinued the program 2 years post-study termination. 123 Thus, it is unclear if the program could be sustainable without research funding or in non-urban settings.
Several other studies have examined cognitive-behavior based psychosocial interventions for WLWH. Brown and colleagues conducted a randomized controlled trial in the U.S. testing a single session computerized stress management training against a waitlist control condition. 124 The intervention provided psychoeducation on stress, information on cognitive reappraisal of stressors, coping strategies, relaxation training, and motivational interviewing. Participants were also given a workbook of activities and a relaxation CD to practice at home. 124 The women in the intervention had significantly greater knowledge of stress management techniques but no changes in their perceived stress, depressive symptoms, or coping self-efficacy as compared to the waitlist condition. 124 The authors attribute this lack of significant changes to the single session intervention being too low of a dose or the follow-up period being too short. They hypothesized that it may take longer than 1 month for changes in coping to be detectable. 124 Another intervention for WLWH with cognitive behavioral techniques is mindfulness-based cognitive therapy (MBCT). It is an 8-week group intervention that incorporates formal and informal mindfulness practices with cognitive therapy techniques. 125,126 MBCT was originally designed as an intervention to prevent depression relapse. 126 One research group in Iran tested this among WLWH and found that it improved participants’ quality of life and decreased their sense of loneliness compared to a control group of WLWH who did not receive the intervention. 127 However, this study did not measure the intervention’s effect on mental illness symptomatology, including depressive symptoms. Further, the authors excluded women receiving treatment for “psychological illness” (pp. 108). Thus, as with the SMART/EST study, it is not possible to generalize the findings of this study to interventions for WLWH with active mental illness.
Due to the high prevalence of trauma among WLWH, some cognitive-behavioral interventions have attempted to address the unique needs of WLWH with posttraumatic stress symptoms. The group intervention, Living in the Face of Trauma (L. I. F. T.) was designed for individuals living with HIV with childhood sexual trauma histories to improve coping and reduce posttraumatic stress symptoms. 128 Intervention groups were either all-male or all-female and took place at community health care clinics in New York City. Women in the intervention were invited to 15 sessions of a weekly coping skills group that provided psychoeducation, adaptive problem-focused and emotion-focused coping skills application, and group processing. The skills taught included cognitive-behavioral techniques such as cognitive restructuring, communication, and decision-making improvement, as well as trauma-focused techniques like sharing trauma narratives and addressing the thoughts and behaviors common to WLWH with sexual abuse histories. 129 The authors reported that there was variable attendance at the intervention sessions with approximately 30% of intervention participants attending fewer than two-thirds of sessions. 128 Nevertheless, for both men and women in the L.I.F.T. intervention, it was effective in reducing intrusive and avoidant symptoms of posttraumatic stress 128 and for the WLWH, it improved psychological well-being. 129
Another cognitive-behavioral intervention for WLWH that included a focus on trauma symptomatology was the Striving Toward Empowerment and Medication Adherence (STEP-AD) study. 130 Although the primary aim of the study was to improve medication adherence, it employed cognitive behavioral problem-solving techniques and coping skills for dealing with trauma symptomatology and racial and HIV-related discrimination, along with skills to improve medication adherence. The authors reported that women’s self-reported posttraumatic stress disorder symptoms decreased over the course of the study and, as such, concluded that STEP-AD was an acceptable treatment for addressing trauma symptomatology. 130 However, these findings were derived from a sample size of 5 U.S. women, so there is a need for more rigorous studies of this intervention in the future.
Supportive treatments
Supportive, peer-facilitated programs have also been utilized in addressing the psychosocial and mental health issues faced by WLWH. In these programs, having WLWH as the program facilitators engendered credibility and engagement in the intervention and decreased feelings of isolation among the WLWH participants. 131,132 The credibility piece has been particularly salient for interventions promoting self-care and self-management of disease. 131
Webel and colleagues conducted a randomized controlled trial of a 7-session group self-management intervention led by trained peer leaders following the Positive Self-Management Program in a U.S. urban setting. 132 The majority of sessions focused on medication adherence and other health behaviors but some dealt with cognitive symptom management, emotion regulation, problem-solving, relaxation, and techniques to manage depression. 132 Those in the intervention group demonstrated better quality of life scores in the domains of HIV mastery and disclosure worries but not in symptom management. 132 When discussing the lack of significance in their primary outcome, self-management, the authors noted that the peer-facilitators in the study sometimes struggled with delivering the intervention, specifically with the wording of the scripts. This highlights the importance of tailoring psychosocial interventions to both facilitators and recipients. Despite this limitation, the participants in the study felt the content was helpful and the intervention fostered a sense of community. 132
The Women’s Empowerment Program (WEP) utilized a dual-facilitator design to provide participants with expertise in 2 areas of HIV-related self-care: 1) a nurse with extensive knowledge in women’s health and HIV care and 2) a WLWH peer facilitator with knowledge on self-management regarding living with HIV. 131 The study aimed to assess if the self-care management program would lead to decreases in depressive symptoms. WEP consisted of 4-hour sessions held once a month for 4 months. The sessions included a communal meal, small-group breakout sessions, role-playing, and didactic portions covering social support, HIV-related information, self-esteem, and self-care specifically designed for WLWH in the U.S. Midwest. 131 On average, participants experienced improvement in feelings of social support and self-esteem, use of self-care behaviors, and depressive symptoms, although the changes in self-esteem and depression were not statistically-significant. The authors attributed their non-significant findings to the study’s small sample size (N = 34). Although the results of this study were promising, WLWH participants provided feedback that they would have liked more program content surrounding emotional problems and depression. 131
The UNITY program is another supportive intervention that utilized workshops led by peer facilitators in an attempt to reduce HIV-related stigma for African-AmericanWLWH. 133 This 2-session program included group discussions and multimedia on coping skills and social support exercises to deal with stigma. This intervention’s efficacy was tested in a U.S.-based randomized controlled trial. Although women in the intervention demonstrated a decrease in illness-related stigma, the reduction was not significant when compared to the study’s control group that also exhibited reduction in stigma. 133 The authors hypothesized that peer support, which was present in both the intervention and control condition, was more important in combatting stigma than the HIV-specific education delivered in the intervention. 133
Mental Health Treatment Among Pregnant and Parenting Women Living With HIV
A series of interventions addressed improving the mental and physical health of pregnant and parenting WLWH through their support networks and families. One such intervention is structural ecosystems therapy which consists of a counselor meeting with a woman living with HIV in her home and working with her on improving support networks to better serve her needs. 134,135 Studies of structural ecosystems therapy conducted in the U.S. have shown it to be efficacious in reducing psychological distress and family-related hassles. 134,135 Authors of some studies, however, note the logistical difficulty in conducting in-home sessions with WLWH and their families and lower than expected engagement rates of WLWH. 134,135
Another home-visit intervention involved nurses conducting sessions on self-care symptom management with African-American mothers living with HIV in the U.S. 136 The sessions covered stress and concerns of the mother, cognitive reframing, self-care, and HIV symptom management. 136 A randomized controlled trial of this intervention found that compared to a usual care condition, women receiving the sessions reported less stigma and improved physical functioning. 136 Although the women in the intervention did not demonstrate significant reductions in overall depressive symptom severity, there were significant reductions in their symptoms of depressed/dejected mood and tense/anxious mood. 136 The authors of the study reported high participant attrition (approximately 40%) but it is unclear if WLWH dropped out during the intervention or research follow-up period.
In another intervention for mothers living with HIV, women and their adolescent children attended group sessions separately for half of the intervention and together for the other half. The mothers’ group aimed to improve parenting and health behaviors and decrease mental health issues through coping with illness, emotions, and disclosure. 137,138 When the intervention was tested in New York City in the 1990s, they found significantly lower depressive and anxious symptoms at both 15 months and 2 years after the end of the intervention 138 but these results were not replicated in another study of the same intervention in Los Angeles 10 years later. 137 When accounting for the inconsistency in outcomes, the authors of these studies underscore the changing demographics of women living with HIV and HIV-related services and treatment available at the time of the 2 studies. 137
Mental health treatments for pregnant and postpartum mothers living with HIV have primarily been provided as part of prevention of mother-to-child transmission interventions or as an adjunctive piece to usual HIV care. 139 -141 The majority of psychosocial interventions for pregnant WLWH targeted depressive symptoms, although one mobile-based intervention in Nigeria used Acceptance and Commitment Therapy techniques in an attempt to improve psychological flexibility. 141 Other perinatal programs in Tanzania, South Africa, and Thailand used psychosocial support as their main form of treatment, 139,140,142 often complementing psychoeducation on disease management, skill building, and if and how to disclose their HIV-positive status to their support networks. 139,140 Despite the reported improvements in psychosocial outcomes, several perinatal studies noted participant attrition in their discussion of study limitations. 139,140 The authors attributed this in part to systemic barriers such as women not being able to attend treatments due to lack of flexibility in their schedules from work and other commitments and from fear of unintended disclosure by attending the intervention at the health clinic. 139,140
Mental Health Treatment Among Women of Trans Experience
Women of trans experience have an estimated 14% prevalence of HIV and high rates of depression symptomatology (44%) and trauma experiences (56%). 143 They tend to have worse self-reported mental health than cisgender women 144 and cisgender men living with HIV. 145 Although there are instances of psychosocial interventions recruiting trans men and women, 128 there is limited research on interventions for women of trans experience or what the outcomes are for this specific group of women. One exception is a pilot study in the U.S. which evaluated the Seeking Safety group therapy intervention on substance use and posttraumatic stress symptoms. 146 Through 12 weekly group sessions focusing on cognitive, behavioral, and interpersonal concerns associated with trauma and substance use, enrolled women saw reductions in posttraumatic stress, alcohol abuse, and drug abuse symptom severity. Although it is difficult to draw sweeping conclusions about this intervention due to the pilot study’s small sample size (N = 7), the combination of social support and therapeutic skills appeared to be beneficial. 146
Psychopharmacologic Treatment of Mental Illness Among Women Living With HIV
In addition to psychosocial and psychotherapeutic treatments, psychopharmacologic treatments for psychiatric disorders can be helpful, ideally in combination, or alone for WLWH. When the psychiatric disorder is more severe, the role of psychopharmacology can be an important addition to psychotherapeutic interventions. For major depressive disorder in particular, the combination of therapy and antidepressant medication is associated with better ART adherence as demonstrated in an international meta-analysis of 12,000 adults with HIV 147 and a U.S. multi-center study of 2,628 WLWH. 148 In another U.S.-based study looking at psychopharmacologic treatment for depressive symptoms in people living with HIV/AIDS, greater adherence to psychopharmacologic treatments regardless of medication class was positively associated with higher ART adherence and mediated the association between depressive symptoms and ART adherence. 149
For pregnant WLWH, untreated symptomatic psychiatric disorders can have a deleterious effect on the pregnancy and mother. Thus, effective treatment is imperative. For major depressive disorder, a class of antidepressant medications, the selective serotonin reuptake inhibitors (SSRIs) are often used due to their tolerability and safety profiles. These medications have a reassuring safety profile in pregnancy, 150 breastfeeding, 151 and in combination with ART. 152 There is a randomized controlled trial in progress in Uganda comparing the effects of an evidence based depression care model versus usual care on adherence called M-DEPTH. This study will incorporate a stepped up care continuum with psychotherapeutic and psychopharmacologic interventions including SSRIs. 153
There are few published studies on psychopharmacologic treatments and their effect on mental illness that are specific to individuals living with HIV. 154 Instead, many studies from the general population have been extrapolated to inform clinical practice. For WLWH, there are specific gaps in evidence pertaining to pharmacotherapy. The first is potential drug-drug interactions between antiretroviral medications and antidepressants, anxiolytics, antipsychotics, mood stabilizers, or other medications for psychiatric illness. 155 It is always important to review drug-drug interactions whenever prescribing any medication to understand the treatment implications while balancing the risks. Every medication will have a different profile and potential effect on the cytochrome P450 isoenzymes. 156 Another consideration is the mental health treatment preference of each individual woman living with HIV while providing the most informed treatment recommendations for their condition. In the U.S., for example, African Americans and Latinas are less likely than their white counterparts to find antidepressant medications acceptable. 157,158 Although antidepressant use in the U.S. increased for African-American and Hispanic individuals over a decade from the 1990s to 2000s, they were still far less likely to take such medication compared to their white counterparts. 159 Given the extant racial and ethnic disparity in HIV prevalence, 2 psychopharmacologic treatment for WLWH requires attention to these patient preferences to optimize adherence and self-efficacy.
Discussion
WLWH experience a greater burden of mental health conditions and symptomatology compared to the general population, women without HIV, and men living with HIV. Mental health issues in WLWH, particularly depression, posttraumatic stress, and anxiety are associated with a decreased quality of life and worse HIV-related health outcomes. Due to the connection between mood and anxiety symptoms and negative HIV-related health outcomes, several health interventions have incorporated psychosocial aspects such as cognitive reappraisal and stress management into routine HIV care. However, there have been few researched interventions with the primary aim of addressing mental illness in WLWH.
There is a large research base showing that depression is commonplace among WLWH, with harmful consequences for social, occupational, and familial functioning. It has also been linked to poor HIV management including ART adherence and worse disease progression. Yet few psychosocial interventions have specifically addressed treatment of active depression in WLWH and even fewer have been shown to be effective in reducing depressive symptoms. Some notable studies that addressed depressive symptomatology did not include WLWH with major depressive disorder in their samples so results cannot be extrapolated to women with depression. 116,118 Given the high rate of major depressive disorder, this constitutes a critical gap in the knowledge-base of mental health interventions for WLWH.
While access to mental health treatment specific to the needs of WLWH in general is inadequate, there is also a lack of research on mental health treatment for specific groups of WLWH. The periods of pregnancy and the postpartum see an increase in stress, depression, and anxiety for women and engender additional stressors regarding disclosure, prevention of transmission to baby, and stigma for WLWH. Research on perinatal mental health conditions for WLWH has been done primarily in Africa. The majority of research has been done as part of transmission prevention programs, rather than as direct mental health interventions. Another group with a dearth of research is women of trans experience. Although the research on HIV among transgender women has grown exponentially in recent years, studies on mental health treatment for transgender women have not. Little is known on how psychosocial interventions could benefit transgender WLWH with mental health issues.
Existing research demonstrates that psychosocial interventions can be beneficial for WLWH. Interventions that target the unique needs of WLWH such as decisions regarding disclosure of HIV serostatus, intersectional stigma, and coping with medical symptom management have demonstrated improved quality of life. Group interventions that offer a peer-support component have been shown to be acceptable to WLWH. Indeed, improving the support networks, whether it be family or other WLWH, can help to improve mental health in this population.
Despite the existing research on mental health and mental health interventions for WLWH, more work is necessary to adequately address the needs of this population. Future research should examine how the mental health of WLWH compares to women living with other chronic medical conditions as this may illuminate the role of HIV sequelae in mental illness and targets for mental health interventions. In regard to mental health interventions for WLWH, several questions remain. First among these is what types of mental health interventions are effective for WLWH who present with clinically significant mental health issues. Limited research has focused on mental health-specific interventions that are feasible, acceptable, and accessible for WLWH. Second, as demonstrated in this review, several interventions with psychosocial components for the health of WLWH have been shown to be efficacious in controlled research settings. However, much less research has focused on implementation: whether these studies of efficacy translate to effectiveness when implemented in real-world settings. Prior research has illustrated the harmful effect of HIV-related stigma on mental health and how some interventions have tried to address this construct; Very little mental health intervention research has examined how to overcome the additional stigma of mental illness and mental health treatment among WLWH. For instance, wellness and exercise-based interventions may carry less stigma than traditional mental health interventions and have been shown to improve depression and quality of life in people living with HIV, but there is a lack of this research among WLWH. 160,161
We know that the burden of mental health issues is great among WLWH and that supportive and cognitive-based components of health interventions have shown promise for addressing these issues. We also know that pharmacotherapy may be an effective approach in some cases, but studies on acceptability and health systems approaches to increasing access to psychopharmacology within the existing HIV care delivery system are lacking. In summary, research targeting mental health, particularly through the lens of dissemination and implementation is warranted to fill the extant gaps in services for WLWH.
Footnotes
Authors’ Notes
The findings and conclusions are those of the authors and do not represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Third Coast Center for AIDS Research: Third Coast CFAR SP0029591.