
Abstract
Introduction
To sustain progress toward epidemic control, it remains essential to enhance and refine Appointment Spacing Model (ASM) implementation while reinforcing coordination between health facilities and community services. Nonetheless, even with the rollout of the six-month multi-month scripting (MMS)/ASM, there is still limited evidence on its nationwide adoption and the factors that affect its utilization.
Methods
This systematic review and meta-analysis followed a protocol registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the reference number CRD42024597279. Articles were retrieved from multiple electronic databases, including PubMed/MEDLINE, Wiley Online Library, Cochrane Library, and African Journal Online, with additional gray literature searched via Google Scholar. Data were initially extracted in Microsoft Excel and subsequently imported into STATA version 11 for analysis. Study heterogeneity was assessed using Cochran's Q test and the I² statistic.
Results
The initial search yielded 1026 primary articles, which were managed using EndNote X7. Of these, 54 were from PubMed, 14 from Wiley Online Library, 6 from the Cochrane Library, 17 from African Journal Online, and 935 from Google Scholar. Ultimately, 8 studies with a combined sample size of 3328 were included in the review. In this study, the pooled prevalence of ASM uptake among people on antiretroviral therapy (ART) in Ethiopia was estimated at 48.22% (95% CI: 31.01-65.44, I² = 92.9%, P = .000). Strong social support (Pooled Odds Ratio [POR]: 1.92, 95% CI: 1.46, 2.54), baseline regimen change (POR: 2.26, 95% CI: 1.74, 2.93), and duration of ART more than five years (POR: 2.15, 95% CI: 1.57-2.97) were factors associated with ASM.
Conclusions
The uptake of the ASM for ART care was relatively low at 48.22%, falling short of the 70% target. Key factors influencing uptake included strong social support, changes to the baseline treatment regimen, and duration on ART. To enhance the adoption of the six-month MMS/ASM care model, public health hospitals and both governmental and nongovernmental organizations should implement targeted interventions addressing these determinants.
Plain Language Summary
Many adults living with Human Immunodeficiency Virus (HIV) in Ethiopia can use the ASM to reduce clinic visits. Our review shows uptake varies, influenced by distance, health status, stigma, and patient confidence. Understanding these factors helps programs support safe, convenient HIV care, saving time and improving patient satisfaction.
Introduction
Human Immunodeficiency Virus (HIV) remains a leading cause of illness and death, especially in Africa. By 2018, an estimated 37.9 million people worldwide were living with the virus, with about 20.6 million residing in Eastern and Southern Africa. 1 The Joint United Nations Programme on HIV/acquired immunodeficiency syndrome (AIDS) (UNAIDS) introduced the 95-95-95 targets, which seek to ensure that by 2030, 95% of people living with HIV know their status, 95% of those diagnosed are on antiretroviral therapy (ART), and 95% of those receiving treatment achieve viral suppression. 2 In Ethiopia, roughly 84% of people living with HIV know their status. Of these, 83% are on ART, and 96% of adults receiving ART have successfully achieved viral suppression. 3
Based on the 2016 WHO recommendations, a new care delivery approach was introduced to better manage the growing number of stable patients on ART and to enhance retention and health outcomes. Ethiopia adopted this strategy, known as the Appointment Spacing Model (ASM), and began implementing it in April 2017. 3 The ASM was developed for clinically stable adults on ART to lessen the number of clinic visits, reduce pressure on health facilities, and enhance both adherence and quality of care. Its objectives are to meet patient needs, lower travel expenses, decrease waiting times, and ultimately support improved self-management and long-term retention in care.4–6 This strategy sought to cover 70% of stable adult HIV clients by providing clinical visits every six months for medication refills. It serves two main purposes: improving patient health outcomes in alignment with the UNAIDS 95-95-95 targets and allowing healthcare facilities to broaden access to HIV services. 6
The ASM is an approach designed to optimize HIV care services by decreasing the number of clinic visits and medication pickups, thereby saving healthcare resources and enhancing the efficiency of patient management. In 2017, Ethiopia became the first country in sub-Saharan Africa to widely implement multi-month scripting (MMS)/ASM for HIV care. The program was developed with attention to sociocultural factors, awareness levels, stigma and discrimination, resource requirements, and long-term sustainability. Through ASM, stable clients attend clinical appointments and receive medication refills every six months. 7
The ASM is linked to a reduced risk of death, as patients participating in the program have a lower likelihood of dying compared to those who are not enrolled. 8 Findings from multiple studies show that the ASM is associated with improved retention rates (97%), a reduction in loss to follow-up (with missed appointments decreasing from 24.4% to 20.3%), lower service costs compared to traditional methods, and better treatment adherence. Furthermore, it improves median waiting times and boosts provider satisfaction.5,6,9 Ethiopia has achieved notable success with the ASM, maintaining high viral suppression rates among clients despite fewer clinic visits. To sustain progress toward epidemic control, it remains essential to enhance and refine ASM implementation while reinforcing coordination between health facilities and community services. Nonetheless, even with the rollout of the six-month MMS/ASM, there is still limited evidence on its nationwide adoption and the factors that affect its utilization. 10
The purpose of this study was to assess the uptake of the six-month multi-month scripting/appointment spacing differentiated service delivery model among stable clients on ART and to identify factors influencing its use. The results are expected to be vital for enhancing service quality and ensuring the sustainability of HIV treatment programs, especially in resource-constrained settings like Ethiopia. Furthermore, the study can guide program planners in designing evidence-based interventions to address barriers to ASM uptake and support progress toward the global 95-95-95 targets.
Methods
Study Design and Protocol Registration
This systematic review and meta-analysis followed a protocol registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the reference number CRD42024597279. The findings are presented in line with the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA) 2020 guidelines for systematic reviews and meta-analyses 11 (Supplemental file 1).
Searching Techniques
Articles were retrieved from multiple electronic databases, including PubMed/MEDLINE, Wiley Online Library, Cochrane Library, and African Journal Online, with additional gray literature searched via Google Scholar. The study was conducted from September 10 2024 to March 10 2024. EndNote X7 was used to collect and remove duplicate records. The search employed both Medical Subject Headings (MeSH) and free-text terms, using keywords such as “appointment spacing model,” “six-month appointment spacing,” “six multi-month scripting,” “on-time appointment keeping,” “community-based differentiated service delivery models,” “HIV/AIDS care models,” “appointment system,” “multi-month prescriptions,” “human immunodeficiency virus,” “people living with HIV/AIDS,” “HIV/AIDS,” “determinants,” “associated factors,” and “predictors,” with search strings adapted for each database. Two authors (WCT and AMZ) screened the articles by reviewing titles, abstracts, and/or full texts, applying Boolean operators “AND” and “OR” to combine search terms. Additionally, the snowballing technique was applied to the references of selected articles to identify further relevant studies. Any disagreements between the authors were resolved through group discussion (Supplemental file 2).
Source Population
The source populations for this study were adults living with HIV.
Study Selection and Eligibility Criteria
The articles retrieved from the search were imported into EndNote X7 (Thomson Reuters, New York, NY), and duplicates were removed. Two authors (AMZ and YAF) then screened the titles of the remaining articles, excluding those that did not meet the eligibility criteria. Prior to data extraction, the full texts of the selected articles were assessed by the same authors to ensure they satisfied the inclusion criteria. This systematic review and meta-analysis included studies that met the following criteria: (1) Observational studies—cross-sectional, cohort, or case-control—reporting on the uptake and associated factors of the ASM among on ART; (2) studies conducted in Ethiopia; (3) articles published in English up to August 15, 2024; and (4) studies carried out in community or healthcare settings. Excluded were articles without full text, unpublished studies, low-quality studies, case reports, qualitative studies, conference papers, and previous systematic reviews or meta-analyses.
Data Extraction
Once the articles for inclusion were finalized, two independent authors (MTA and WCT) carried out data extraction using a standardized Microsoft Excel template. The process followed the Joanna Briggs Institute (JBI) tool to systematically gather key information from the primary studies. Extracted data encompassed the first author's name, publication year, study region, study design, response rate, sample size, sampling method, prevalence of ASM uptake, and other relevant effect measures. For studies reporting factors associated with ASM uptake among adults living with HIV, odds ratios were analyzed using a two-by-two table.
Quality Assessment
The quality of the included studies was evaluated using the JBI critical appraisal checklist, which is publicly accessible at https://jbi.global/critical-appraisal-tools. 12 The checklist includes nine items, and the overall methodological quality of each study is scored from 0 to 9, categorized as low (0-4), medium (5-6), or high (7-9) quality. In line with the study protocol, two authors (YAF and GWA) conducted a blinded review to assess the quality of the primary studies. Only studies scoring 5 or above on the JBI checklist were included in the review, and any disagreements in the assessment were resolved with the involvement of a third author (WCT) (Supplemental file 3).
Outcome of Interest
The main objective of this review was to estimate the pooled uptake of the ASM among adults living with HIV in Ethiopia. ASM uptake was defined for ART clients who met the WHO criteria for stable adults and agreed to follow the six-month schedule for clinical visits and medication refills. Participants who accepted the ASM were categorized as “uptake” and coded as “1”, whereas those who declined were classified as “non-uptake” and coded as “0”. 13
Statistical Analysis
Data were initially extracted in Microsoft Excel and subsequently imported into STATA version 11 (STATA Corp., LLC) for analysis. Study heterogeneity was assessed using Cochran's Q test and the I² statistic, with a p-value below 0.05 considered indicative of statistically significant heterogeneity. 8 Heterogeneity levels were categorized as none (I² = 0.0%), low (I² < 25%), moderate (25% ≤ I² ≤ 75%), or high (I² > 75%). Given the presence of heterogeneity among the studies, a random-effects model was utilized to estimate the pooled uptake of ASM. 14 In particular, the DerSimonian–Laird random-effects model was used to determine the pooled estimate. 14
Subgroup and Sensitivity Analysis
Subgroup analyses were conducted by region, study design, and sample size to explore the sources of heterogeneity among the included studies. Furthermore, a meta-regression analysis was performed using sample size, response rate, and publication year as covariates. A sensitivity analysis was performed to evaluate how each individual study influenced the overall estimate.
Publication Bias
Publication bias was evaluated using both visual inspection of the funnel plot and Egger's test.15,16 A p-value below 0.05 in Egger's test was considered indicative of significant publication bias, implying that studies showing larger effect. 17 A trim-and-fill analysis was performed to adjust for the detected publication bias. 18
Results
Results of the Literature Search
The initial search yielded 1026 primary articles, which were managed using EndNote X7. Of these, 54 were from PubMed, 14 from Wiley Online Library, 6 from the Cochrane Library, 17 from African Journal Online, and 935 from Google Scholar. After removing 848 duplicates, 110 articles were excluded for not being relevant to the study population. The full texts of the remaining 68 articles were assessed against the eligibility criteria, and some were further excluded for not reporting the outcome of interest or ASM uptake. Ultimately, 8 studies with a combined sample size of 3328 were included in the review (Figure 1).

PRISMA Flow Diagram of the Study on Uptake of Appointment Spacing Model and Determinants Among Patients on ART in Ethiopia (n=8). PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols, ART, Antiretroviral Therapy.
Characteristics of Included Studies
This study incorporated eight primary studies published up to 2024, encompassing a sample size of 3328 individuals. Four studies were sourced from the Amhara region,10,19–21 two from Oromia,13,22 and the rest from the Southern region.23,24 All included studies were published in peer-reviewed journals. Regarding study design, seven were facility-based cross-sectional studies, and one was a community-based cross-sectional study. Reported ASM uptake ranged from 19.16% to 85.33% (Table 1).
Overview of Included Studies in the Study on the Uptake of ASM and Determinants Among Patients on ART in Ethiopia (n = 8).

ASM, appointment spacing model; ART, antiretroviral therapy.
Uptake of ASM
In this study, the pooled prevalence of ASM uptake among people on ART in Ethiopia was estimated at 48.22% (95% CI: 31.01-65.44, I² = 92.9%, P = .000). The I² value of 92.9% indicates substantial heterogeneity among the included studies, and therefore, a random-effects model was used to determine the pooled prevalence (Figure 2).

Forest Plot for the Pooled Uptake of ASM Uptake Among Patients on ART in Ethiopia (n=8). ASM, Appointment Spacing Model; ART, Antiretroviral Therapy.
Subgroup Analysis
Subgroup analysis indicated that studies using simple random sampling reported the highest pooled uptake of the ASM among people on ART(85.33% (95% CI: 77.82-92.84) (Figure 3).

A Subgroup Analysis of the Forest Plot Showing the Pooled Uptake of ASM Uptake Among Patients on ART in Ethiopia Based on Sampling Technique (n=8). ASM, Appointment Spacing Model; ART, Antiretroviral Therapy.
Subgroup analysis by region showed that the highest pooled prevalence of ASM uptake among people on ART was reported in the Amhara region at 59.99% (95% CI: 38.52-81.46, I² = 92.6%, P = .000), whereas the lowest prevalence was observed in the Oromia region (Figure 4).
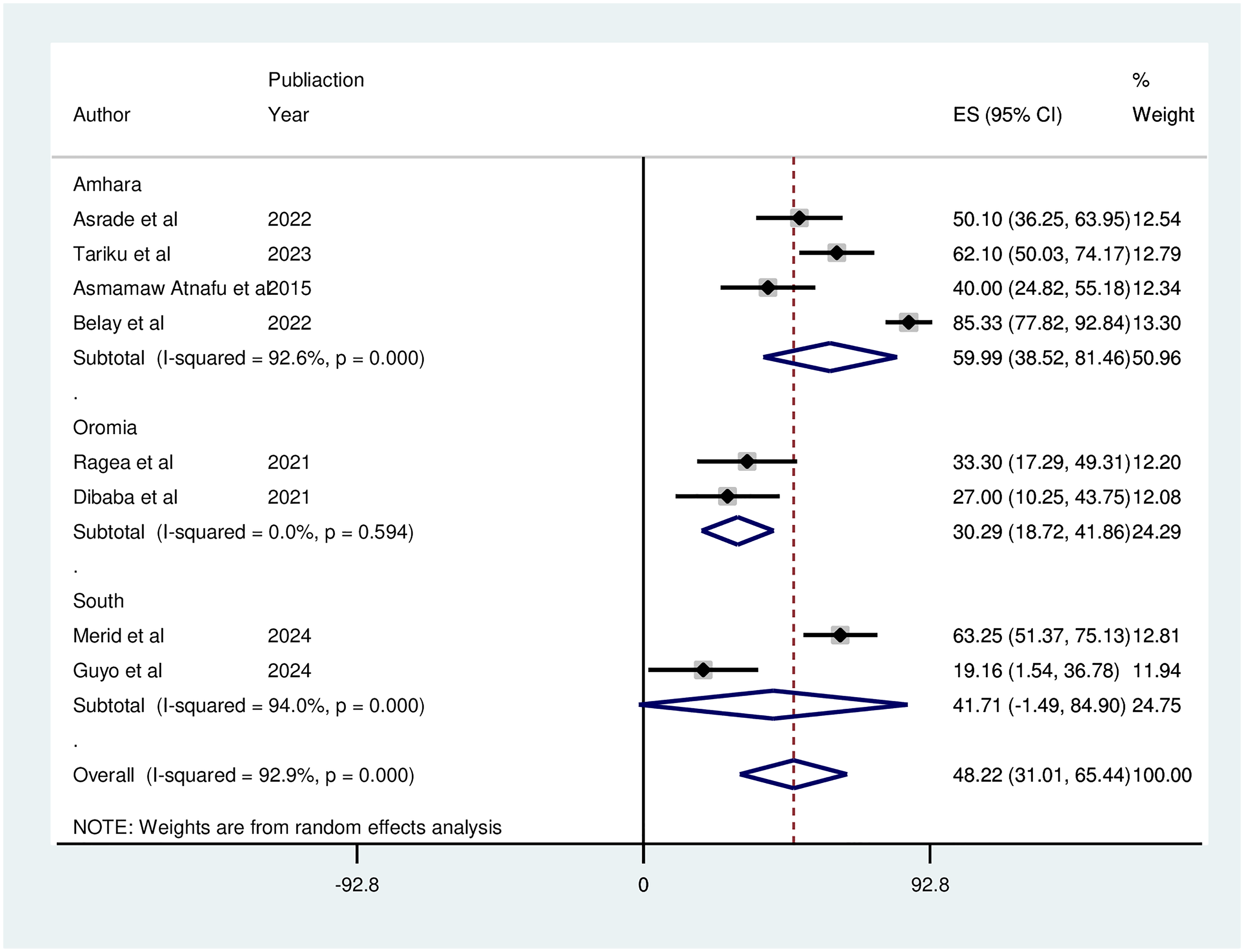
A Subgroup Analysis of the Forest Plot Showing the Pooled Uptake of ASM Uptake Among Patients on ART in Ethiopia Based on Region (n=8). ASM, Appointment Spacing Model; ART, Antiretroviral Therapy.
Publication Bias
The funnel plot displayed an asymmetrical distribution of studies, suggesting potential publication bias. This was confirmed by Egger's test, which yielded a statistically significant p-value of 0.000 at the 5% significance level, indicating the presence of notable publication bias (Figure 5).

Funnel Plot Showing Publication Bias.
Meta-Regression
To explore the sources of heterogeneity, a meta-regression using a random-effects model was conducted on study-level variables. The univariable meta-regression analysis showed that the number of participants, sample size, and publication year were not significant, suggesting that the observed heterogeneity was not attributable to these factors.
Sensitivity Analysis
The analysis revealed substantial heterogeneity among the included studies. A sensitivity analysis was conducted to evaluate the influence of each study on the overall estimate, and the results showed that no single study significantly affected the pooled uptake of the ASM.
Factors Associated with Uptake of the ASM
The meta-analysis identified that uptake of the ASM was significantly associated with strong social support, changes to the baseline ART regimen, and longer duration on ART. Specifically, patients with strong social support were 1.92 times more likely to adopt ASM than those with poor support (Pooled Odds Ratio [POR]: 1.92, 95% CI: 1.46-2.54). HIV patients who had a change in their baseline regimen were 2.26 times more likely to use ASM compared to those without regimen changes (POR: 2.26, 95% CI: 1.74-2.93). Additionally, patients on ART for more than five years were approximately 2.15 times more likely to engage with the ASM model than those on ART for five years or less (POR: 2.15, 95% CI: 1.57-2.97) (Figure 6).

Factors Associated with Uptake of the ASM Among Patients on ART in Ethiopia. ASM, Appointment Spacing Model; ART, Antiretroviral Therapy.
Discussion
This study determined the pooled adoption of the ASM model and its associated factors among stable clients receiving ART in Ethiopia. In this study, the estimated pooled prevalence of ASM uptake among patients on ART in Ethiopia is 48.22% (95% CI: 31.01−65.44, I²=92.9%, P-value = .000). This uptake is higher than what was reported in similar studies, which found rates of 7.2% in Uganda, 25 and 10.3% in Zambia. 26 However, it is lower than earlier findings from Guinea (59.6%) 5 and Malawi (69%). 6 These differences may be due to variations in ASM eligibility criteria between countries. For example, in Malawi, HIV-positive individuals—including children over two years, adolescents, and adults—can access ASM care if they are stable, have been on treatment for at least three months, and have achieved viral suppression. In contrast, countries like Ethiopia, which face challenges such as limited viral load testing and supply chain constraints, have simpler national guidelines that offer combined clinical and medication refill visits every six months, but only for adults. Other factors, such as differences in facility types, key clinical indicators, baseline CD4 counts and viral load levels, as well as the characteristics of study settings, may also contribute to the observed variations.
Patients receiving ART who had strong social support were more likely to adopt the ASM model than those with limited support. This finding is consistent with studies conducted in South Africa, the USA, and other parts of Sub-Saharan Africa.27–29 Strong social connections serve as an important protective factor against illness and overall mortality. The ASM supplemental guide for HIV service delivery emphasizes that clients with robust social support require additional assistance. This support can be strengthened through counseling that encourages patients to disclose their HIV status to family members and treatment supporters. Such care and encouragement from family and the community can enhance self-esteem, which, in turn, fosters positive coping strategies.
Moreover, HIV patients who underwent a change in their baseline ART regimen were more likely to adopt the ASM model than those who did not. This observation aligns with findings from studies conducted in Guinea and Malawi.5,30 One possible reason for this could be the increase in pretreatment resistance to Nevirapine, resulting in poor treatment outcomes. Currently, the WHO recommends alternative first-line regimens based on Dolutegravir (DTG). Consequently, many stable adult clients who transitioned from their initial regimen may experience improved health outcomes due to better adherence, as DTG generally requires less frequent dosing. Since most participants in this study switched to a DTG -based regimen, they are likely to be more inclined to adopt the ASM model.
Furthermore, patients on ART for more than five years were more likely to utilize the ASM model than those on ART for five years or less. This indicates that the longer clients receive care, the more they appreciate the advantages of participating in evolving HIV/AIDS care programs based on their experiences. Another possible explanation is that long-term ART clients develop a deeper understanding of, and gain greater benefits from, the ART service delivery approach.
Strength and Limitations
A key strength of this review is that the authors searched several major databases to identify original articles. However, the study design used does not permit the determination of causal relationships between the outcome and independent variables. Additionally, the prevalence of ASM uptake in certain regions of Ethiopia could not be assessed due to a lack of sufficient studies, which limits the generalizability of the findings to the whole country.
Conclusion and Recommendations
The uptake of the ASM for ART care was relatively low at 48.22%, falling short of the 70% target. Key factors influencing uptake included strong social support, changes to the baseline treatment regimen, and duration on ART. To enhance the adoption of the six-month MMS/ASM care model, public health hospitals and both governmental and non-governmental organizations should implement targeted interventions addressing these determinants. Such efforts would help expand access to ART and support the achievement of HIV treatment goals. Health professionals providing ART services should emphasize counseling clients on the benefits of the six-month MMS/ASM, particularly for those undergoing regimen changes or lacking adequate social support. Additionally, a prospective cohort study is recommended to evaluate the effect of the six-month MMS/ASM on client retention in ART services.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251398934 - Supplemental material for Uptake of Appointment Spacing Model of Care and Determinants Among Adult Clients on Antiretroviral Treatment in Ethiopia
Supplemental material, sj-docx-1-jia-10.1177_23259582251398934 for Uptake of Appointment Spacing Model of Care and Determinants Among Adult Clients on Antiretroviral Treatment in Ethiopia by Worku C. Tassew, Agerie M. Zeleke, Yeshiwas A. Ferede, Moges T. Abebe and Getaw W. Assefa in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251398934 - Supplemental material for Uptake of Appointment Spacing Model of Care and Determinants Among Adult Clients on Antiretroviral Treatment in Ethiopia
Supplemental material, sj-docx-2-jia-10.1177_23259582251398934 for Uptake of Appointment Spacing Model of Care and Determinants Among Adult Clients on Antiretroviral Treatment in Ethiopia by Worku C. Tassew, Agerie M. Zeleke, Yeshiwas A. Ferede, Moges T. Abebe and Getaw W. Assefa in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582251398934 - Supplemental material for Uptake of Appointment Spacing Model of Care and Determinants Among Adult Clients on Antiretroviral Treatment in Ethiopia
Supplemental material, sj-docx-3-jia-10.1177_23259582251398934 for Uptake of Appointment Spacing Model of Care and Determinants Among Adult Clients on Antiretroviral Treatment in Ethiopia by Worku C. Tassew, Agerie M. Zeleke, Yeshiwas A. Ferede, Moges T. Abebe and Getaw W. Assefa in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The author would like to thank the authors of the included primary studies, which were used as sources of information to conduct this systematic review and meta-analysis.
Author Contributions
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.