
Abstract
Objective:
Hepatitis B virus and hepatitis C virus are the leading causes of global liver-related morbidity and mortality. Waste handlers are one of the high-risk groups for hepatitis B virus and hepatitis C virus acquisition. Thus, the aim of this study was to assess the pooled prevalence of hepatitis B virus and hepatitis C virus among waste handlers in Ethiopia.
Methods:
Articles were extensively searched in bibliographic databases and gray literature using entry terms or phrases. Studies meeting eligibility criteria were extracted in MS Excel and exported to STATA version 14 software for statistical analysis. A random-effects model was used to compute the pooled magnitude of hepatitis B virus and hepatitis C virus. Heterogeneity was quantified by using the I2 value. Publication bias was assessed using a funnel plot and Egger’s test. Sensitivity analysis was performed to assess the impact of a single study on pooled effect size.
Result:
Of the 116 studies identified, 8 studies were selected for meta-analysis. All studies reported hepatitis B virus, while 5 studies reported hepatitis C virus infection among waste handlers. The overall pooled prevalence of hepatitis B virus and hepatitis C virus infection among waste handlers in Ethiopia was 5.07% (2.0–8.15) and 1.46% (0.52–2.4), respectively. Moreover, the pooled prevalence of lifetime hepatitis B virus exposure among Ethiopian waste handlers was 33.98% (95% CI: 21.24–46.72). Hepatitis B virus and hepatitis C virus infection were not statistically associated with the type of waste handlers, that is, there was no difference between medical and nonmedical waste handlers.
PROSPERO registration:
CRD42023398686.
Conclusion:
The pooled prevalence of hepatitis B virus and hepatitis C virus infection among waste handlers in Ethiopia was intermediate and moderate, respectively. This showed that there is a strong need to scale up preventive efforts and strategic policy directions to limit the spread of these viruses. Moreover, we also conclude that handling healthcare and domestic waste is associated with a similar risk of hepatitis B virus and hepatitis C virus infection.
Introduction
Viral hepatitis is a major health problem worldwide and causes acute and/or chronic hepatitis, which affects both developed and developing countries.1,2 The clinical impact of the virus indicated the development of extensive liver scarring called cirrhosis, liver failure, liver cancer, esophageal varices, hepatic steatosis, and death.1,2 In addition, hepatitis B infection may also cause the deposition of immune complexes, especially in the kidney. 3 Chronic infection also results in loss of work-related productivity, premature death, and economic burden on individuals and the healthcare system. 4 For example, economic evaluation of societal costs of hepatitis B is equivalent to 3.2% of national healthcare expenditure.
Hepatitis B virus (HBV) and hepatitis C viruses (HCV) cause chronic viral hepatitis, a major global health problem responsible for 57% of liver cirrhosis 5 and 75% of primary liver cancer 6 cases, respectively. Approximately 2.2 billion people, which is over a third of the world’s population, have shown evidence of past or present infection with viruses. Approximately 500 million of these are chronically infected, more than 10 times those affected by HIV/AIDS. 7 Every year, chronic viral hepatitis results in approximately 1.3 million deaths from chronic liver disease and hepatic cellular carcinoma. 8
Viral hepatitis is the 10th leading cause of death and the leading cause of liver cancer worldwide. 9 The World Health Organization (WHO) showed that approximately 170 million people are infected with HCV, approximately 130 million are carriers, 3–4 million persons are newly infected each year, and more than 350,000 people are estimated to die from HCV-related liver diseases each year worldwide. 10 HBV is endemic in Africa next to Asia, with a seroprevalence rate between 8% and 20%. 11 The world’s highest prevalence is in Egypt (17.5%), followed by Cameroon (13.8%) and Burundi (11.3%). 12
Ethiopia is one of the countries with a high burden in Africa, with a high prevalence of HBsAg (35.8%) and anti-HCV (22.5%) among chronic liver diseases. 13 A hospital-based study also indicated that hepatitis B accounts for 12% of hospital admissions and 31% of deaths in Ethiopian hospitals. 14 In addition, another study indicated that at least one of the hepatitis markers was found in 78% of patients with hepatocellular carcinoma, 86% of chronic hepatitis cases, and 88% of cirrhosis patients, 15 and the mortality rate reported due to hepatocellular carcinoma is among the highest in the world at approximately 93.45 per 100,000 in Ethiopia. 16
The highest rates of occupational injury among all workers who may be exposed to health care waste reported by waste handler personnel in the USA are 180 per 1000 annually. 17 Some studies have shown that in hospital settings, approximately 30 injuries occur per 100 beds per year. 17 The latter findings also showed that 40 incidents of sharps injuries are associated with waste handling. Even though no seroconversion occurred, waste handlers needed prolonged leave of absence with professional counseling for anxiety or stress disorder. 18
Sharps generated from in-home medical use, such as in the treatment of diabetes and discarded sharps collected by domestic waste handlers, can pose significant problems when disposed of in municipal solid waste. Uncontained sharps can pose a health and safety problem to waste handlers in the environment, where bags are inspected for banned wastes or recyclables are removed from the waste stream, which can be inadvertently punctured; consequently, domestic waste handlers could have risk of acquiring HBV and HCV infection after exposure to contaminated sharp instruments that have been improperly discarded.19,20
The availability of safe and effective vaccines against HBV in resource-limited countries such as Ethiopia is scarce 21 and increases the risk of HBV infection. Thus, many waste handlers remain at higher risk of acquiring HBV infection, and these groups are known to be much at risk of occupational blood-borne infectious pathogens, but there are few documented data, and these subjects were deprived of attention. Evidence on the epidemiology of these viruses is of paramount importance to design control strategies for the disease and to implement preventive measures. Thus, this systematic review and meta-analysis was intended to assess the national pooled seroprevalence of HBV and HCV among waste handlers in Ethiopia.
Methods
Design and protocol registration
This systematic review and meta-analysis was designed to estimate the national pooled seroprevalence of HBV and HCV among waste handlers in Ethiopia. The result was reported based on the Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P) 22 (see Supporting Information). The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42023398686.
Data source and search strategy
All articles regarding HBV and HCV infection were retrieved via a scientific search of electronic databases, including PubMed/crucial, Web of Science, Research Gate, and Scopus, from 10 to 30 February 2023. In addition to accounting for the studies’ omission during electronic database searches, a direct Google search was carried out using listed references in the included articles.
The comprehensive and extensive searching strategy has been employed using condition, context, population, and outcome of interest (CoCoPop) formulating questions and searching terms were (‘‘Prevalence”), (“epidemiology”) (“magnitude”), and (“Hepatitis B virus”), (“HBV”), (“Hepatitis C virus”), (“HCV”), and (“waste handlers”), (“janitors”), (“cleaners”), and (“Ethiopia”). The search terms were combined using the Boolean operators “OR” and “AND” to fit the advanced searching of articles.
Study selection and quality assessment for risk of bias
Three independent authors (AG, FBG, SS) identified the articles from databases and other sources. Duplicates were removed, and four independent reviewers (AS, YE, HD, MT) continued to screen the title and abstract of all potentially eligible studies. Then, the full text of potentially eligible studies that reported the prevalence or epidemiology of HBV and HCV among waste handlers was added to the collections for extraction. Disagreements between two independent reviewers (WD and MA) were settled by GM to reach a consensus. The quality of the articles was carefully assessed by three authors (AG, WD, MA). The full texts of the articles were used to determine whether the study met the selection criteria or whether the eligibility of the article was in doubt. The Joanna Brigg Institute (JBI) quality assessment manual was used to assess the methodological validity of each study design. 23 Using the critical appraisal checklists, studies were reviewed, and articles with an average score of 50%–75% were considered good quality, while those with a score greater than 75% were defined as high quality. Thus, articles with both good and high quality were included in this systematic review and meta-analysis. Moreover, study qualities were assessed using the Newcastle‒Ottawa Quality scale for cross-sectional studies. 24
Eligibility criteria
Original articles that reported hepatitis B and C viruses among waste handlers in Ethiopia and studies reported only in English were included. Studies reporting hepatitis B and C viruses in review articles, case reports, and letters to the editor were also excluded.
Outcome variables
The outcome variable for this study is the national pooled seroprevalence of hepatitis B and C viruses among waste handlers in Ethiopia. The prevalence of HBV and HCV were computed from the total number of HBsAg and anti-HCV, respectively were positive by enzyme-linked immunosorbent assay (ELISA) or immunochromatographic tests against total sample size. The other outcome variable was the pooled prevalence of HBV lifetime exposure, which was calculated as the total number of anti-HBc antibodies to the total number of participants or sample size.
Data extraction
Data from the eligible studies were extracted by four reviewers (AG, SS, HD, and FBG) independently in Microsoft Excel sheets. The information extracted from each study included the name of the first author, publication year, region, types of waste handlers, and diagnostic methods used.
Statistical analysis
The data extraction was performed using a Microsoft Excel worksheet, and the meta-analysis was performed using STATA version 14 with metan commands. The point estimate and 95% confidence interval of the seroprevalence of hepatitis B and C viruses among waste handlers in Ethiopia for the studies fulfilling the inclusion criteria were calculated. Due to the high heterogeneity reported, the national pooled seroprevalence of hepatitis B and C viruses among waste handlers in Ethiopia was calculated using a random effect model. The Sidik-Jonkman method was used to estimate the between-study variance. Cochrane’s Q test and I2 statistics, which provide an estimate of the percentage of variability in effect estimates that is due to heterogeneity rather than chance alone, were used to assess heterogeneity. 25 A p-value of <0.005 was used to declare significant heterogeneity. Therefore, a random effect model was used to adjust the observed variability. Publication bias was assessed by visual observation of the symmetry of the funnel plot and Egger’s test statistics.26,27 Sensitivity analysis was performed to assess the impact of a single study on the overall pooled effect size. Subgroup analysis for the primary outcome was performed by publication year, region, types of waste handlers, and diagnostic methods used.
Result
Literature search and eligible studies
During the initial electronic search and manual search of reference lists, a total of 116 articles were retrieved. Approximately 39 articles were excluded because of duplication. After reviewing their title and abstracts, 66 articles were excluded due to unrelated titles, not being studied in Ethiopia, and being review articles. Then, the full texts of 11 studies were evaluated for eligibility. Then, three articles were excluded because they were not related to the objective. Finally, after methodological quality assessment, eight studies were included in this systematic review and meta-analysis (Figure 1).

Flow diagram for the selection process of eligible studies.
Characteristics of the included studies
The studies were conducted from 2011 to 2023 in three national and regional states and one city administration in Ethiopia. Of these, two studies were conducted in the Addis Ababa city administration, and four studies were from the Amhara national regional state. All studies were cross-sectional and published in English. Three studies enrolled in this study were conducted on medical waste handlers and nonmedical waste handlers, and another three studies were conducted on medical waste handlers only. Only one study was used above 384 (i.e., 388). Of the 2127 participants who were included in the study, 1345 and 514 were medical and nonmedical waste handlers, respectively. From a total of 111 HBsAg-positive waste handlers, 103 were medical and 8 were nonmedical waste handlers, while 14 waste handlers were positive for anti-HCV, of which 12 were medical and 2 were nonmedical waste handlers. In addition, from a total of 1052 medical waste handlers reported in four studies, 197 (18.7%) waste handlers had received hepatitis B vaccine. (Table 1). Moreover, two studies reported lifetime exposure to hepatitis in 2011 and 2016. From a total of 486 waste handlers, 174 were positive for anti-HBc (Table 2).
Characteristics of included studies.
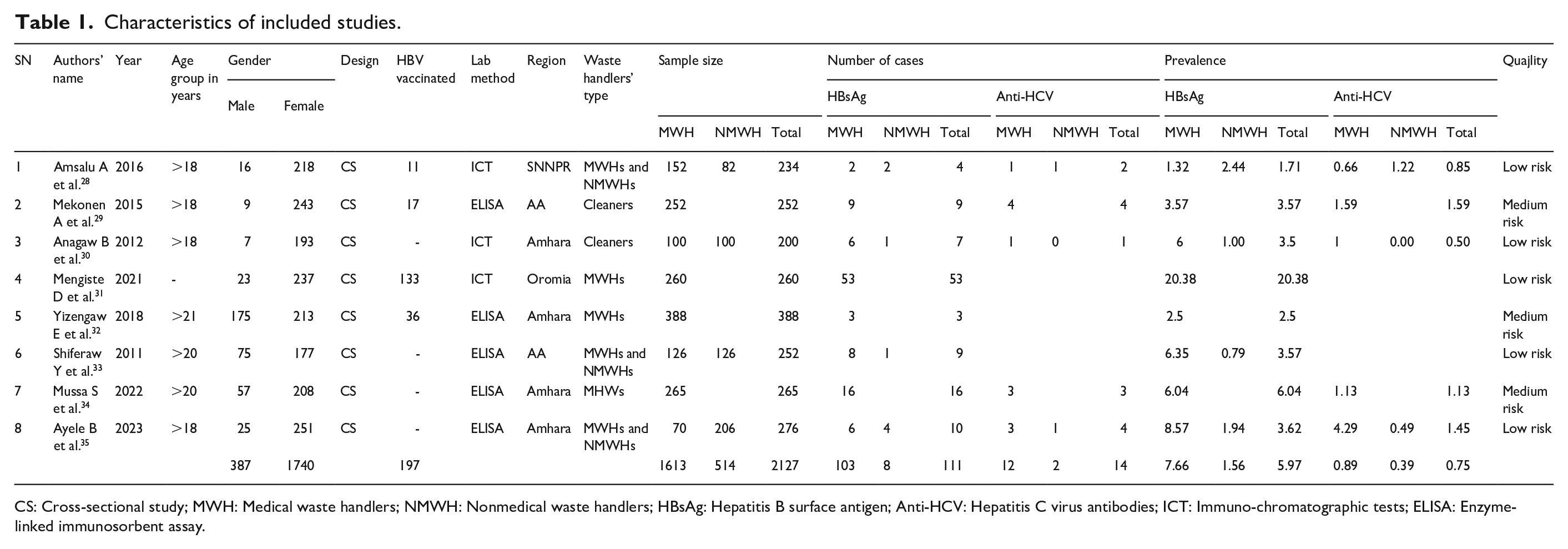
CS: Cross-sectional study; MWH: Medical waste handlers; NMWH: Nonmedical waste handlers; HBsAg: Hepatitis B surface antigen; Anti-HCV: Hepatitis C virus antibodies; ICT: Immuno-chromatographic tests; ELISA: Enzyme-linked immunosorbent assay.
Lifetime exposure status of studies included in the systematic review and meta-analysis.

MWH: Medical waste handlers; NMWH: Nonmedical waste handlers; Anti-HBc: Hepatitis B core Antibody.
Prevalence of HBV infection among waste handlers in Ethiopia
HBV infection was reported from 1.32% to 20.38% in medical waste handlers and from 0.79% to 2.44% in nonmedical waste handlers. The overall pooled magnitude of HBV infection among waste handlers using the random effect Sidik-Jonkman model was 5.07% (95% CI: 2.0–8.15). Significant heterogeneity was observed, with an I2 value of 99.96% and a heterogeneity Chi-squared of 2532.06 (Figure 2).
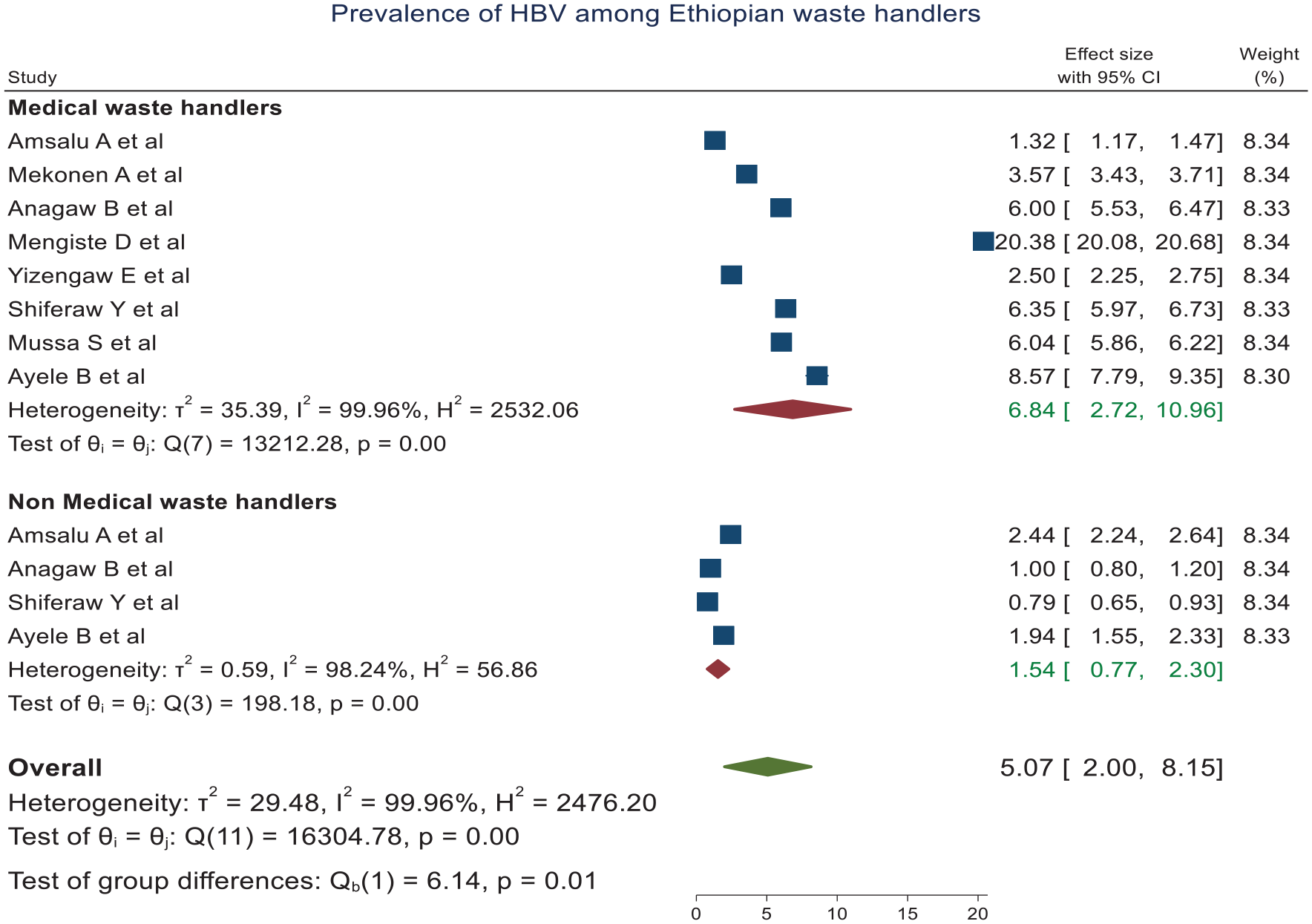
Forest plot showing the magnitude of HBV among waste handlers in Ethiopia.
From the pooled prevalence rate of 5.07%, the prevalence of HBV among MWHs and NMWHs was 6.84% (95% CI: 2.72–10.96) and 1.54% (95% CI: 0.77–2.3), respectively. The difference in the magnitude of HBV infection between the types of waste handlers (i.e., MWHs vs NMWHs) was statistically significant. Being a medical waste handler did not have any additional risk of acquiring HBV infection compared to nonmedical waste handlers (pooled OR = 3.57; 95% CI: 0.96–13.24; p = 0.06) (Figure 3).

Forest plot showing the association between types of waste handlers and HBV infection.
Subgroup analysis
The pooled proportion of HBV among waste handlers was 5.76% in the Amhara region. More than half of the studies used ELISA as a diagnostic tool and reported 5.39% of HBV than 9.23% in immunochromatographic tests (ICT) (Figure 4).

Forest plot showing subgroup analysis by region and laboratory method.
Heterogeneity exploration and publication bias
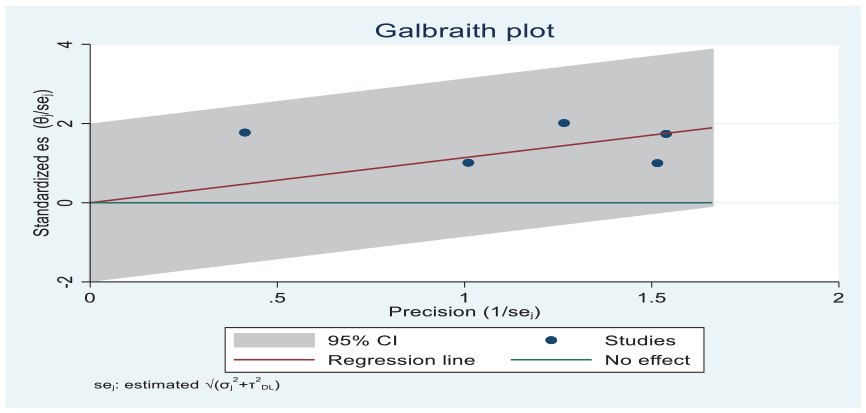
To assess the possible sources of heterogeneity, a Galbraith plot was computed and indicated that one study was found outside of the 95% CI or not found between 2 and −2 (Figure 5). Moreover, sensitivity analysis was also performed to rule out the presence of a single study effect, but none of the studies were omitted, indicating the absence of a single study effect (Figure 6).

Galbraith plot of hepatitis B virus among waste handlers.

Forest plot of sensitivity analysis of HBV among waste handlers.
HBV lifetime exposure among waste handlers
The pooled prevalence of HBV lifetime exposure among Ethiopian waste handlers was 33.98% (95% CI: 21.24–46.72), where the magnitude was significantly varied among medical and nonmedical waste handlers, that is, the pooled prevalence was 43.54% (35.57–51.51) among medical waste handlers and 21.41% (10.04–38.79) among nonmedical waste handlers (Figure 7). The pooled effect of the type of waste handlers showed that being a medical waste handler increased the odds of lifetime exposure by 2.39 times compared to being nonmedical waste handlers, and it was statistically significant (Figure 8).

Forest plot showing lifetime exposure to HBV among waste handlers.

Forest plot showing the association between types of waste handlers and HBV lifetime exposure.
Prevalence of HCV among waste handlers
The pooled prevalence of anti-HCV among waste handlers in Ethiopia was 1.52% (95% CI: 0.60–2.43), whereas the prevalence of anti-HCV among medical and nonmedical waste handlers was 1.71% and 1.04%, respectively (Figure 9).

Forest plot showing HCV infection among waste handlers.
The prevalence of HCV infection among waste handlers was not significantly different between medical and nonmedical waste handlers. Moreover, there was a substantially higher level of heterogeneity between studies (I2 = 99.82%). To explore the sources of this highest heterogeneity, a Galbraith plot and sensitivity analysis were carried out despite the between-studies variability not being ruled out by these methods, that is, none of the studies were omitted by sensitivity analysis, and the estimates of all studies were found to be between 2 and −2 in the Galbraith plot (Figures 10 and 11).

Forest plot of sensitivity analysis of HBV among waste handlers.
Galbraith plot of hepatitis B virus among waste handlers.
Publication bias
The funnel plot was used to assess the impact of the small-studies effect or publication bias on estimated pooled prevalence. The graph of the funnel plot becomes asymmetrical, indicating the presence of publication bias. Furthermore, Egger’s test statistics confirmed the presence of marginally significant publication bias at a p-value < 0.001. Hence, nonparametric trim and fill analysis was performed.
Trim and fill analysis
When trimming and filling, analysis was conducted using a random model, two studies were imputed, and the total number of studies remained at seven. The pooled proportion of anti-HCV was 1.10 (0.52–1.75) at a p-value < 0.001.
Discussion
To the best of our knowledge, this study is the first systematic review and meta-analysis to comprehensively address the burden of HBV and HCV among waste handlers in Ethiopia. The current evidence on HBV and HCV prevalence in Ethiopian waste handlers is reinforced by the scarcity of studies. Thus, the output of this meta-analysis will be used as a means to provide a better understanding of the current prevalence of HBV and HCV infections among the target groups who are at risk of HBV and HCV infections due to their social and economic vulnerability, presenting high prevalence values of the disease when compared to the general population. Moreover, determining the prevalence estimates of these viruses is crucial for establishing appropriate country-specific prevention, diagnosis, and containment strategies. A total of eight studies targeting the two hepatitis viruses were selected using a comprehensive search strategy in validated databases and were quantitatively analyzed for the first time to better determine the burden of these infections in the country. In this meta-analysis, approximately 50% of studies (4 out of 8) compared waste handlers who were exposed to medical waste (i.e., medical waste handlers) with those who were not (i.e., nonmedical waste handlers).
The pooled prevalence of HBV infection among waste handlers was 5.07%, with great heterogeneity between its regional states in Ethiopia. The finding of this meta-analysis was lower than the previous findings reported from studies conducted in Nigeria, 36 Brazil, 37 Pakistan, 38 and Central Greece, 39 which showed HBV prevalence rates in waste handlers of 14%, 17.4%, 18.8%, and 23.0%, respectively. The lower prevalence rate of HBV in this study might be explained by differences in the behavioral characteristics of waste handlers recruited in the primary studies. For example, the higher proportion of intravenous drug users and male homosexuals in other countries might contribute greatly to an increased rate of HBV, but in the Ethiopian context, these types of behaviors are not greatly noticed. However, these variables are not common in Ethiopia, and the unavailability of health education material, no use of personal protective equipment, handling waste with bare hands and feet, inadequate and precarious waste disposal systems, handling of piercing-cutting instruments (biomedical waste), and poor vaccination status might contribute to the infection rate in our context.
Although the pooled prevalence of HBV among medical waste handlers (6.84%) was higher than that among nonmedical waste handlers (1.54%), the difference was not statistically significant (p = 0.06). The nature of the work, frequent exposure status with body fluids, handling of piercing-cutting instruments (biomedical waste), workload, and presence of noise might contribute to the slight increase in HBV in medical waste handlers.
The pooled prevalence of HBV lifetime exposure among waste handlers was 33.98%, which implies that one in every three waste handlers had developed lifetime exposure for HBV. The magnitude of HBV lifetime exposure varied significantly among medical (43.54%) and nonmedical waste handlers (21.41%). The pooled odds of lifetime exposure among medical waste handlers were 2.39 times higher than those of nonmedical waste handlers for developing HBV lifetime exposure.
The pooled prevalence of anti-HCV among waste handlers in Ethiopia was 1.52%, which is graded as moderate. This finding was lower than 3.2% of anti-HCV evidence of the national strategic plan of Ethiopia working toward combating viral hepatitis by 203040 to use as a means of performance evaluation and the way forwards. The finding of this study is also lower than previous findings reported from TB patients (7%) in Ethiopia, 41 although the populations are different. Moreover, the pooled prevalence of anti-HCV among medical and nonmedical waste handlers was 1.71% and 1.04%, respectively, but the difference was not statistically significant. Therefore, the magnitude of anti-HCV among medical waste handlers might be due to informal cleaning practices, accidental needlestick injuries, handling infected sharps before, during, and after disposal, unsafe sharps waste management, which includes incomplete incineration, disposal in open pits or dumping sites, leaving used injection equipment in hospital laundry, and other practices that fail to secure infected sharps waste. 42
The practical implication of this study was that the burden of HBV and HCV infections among medical waste handlers is higher than that among nonmedical waste handlers, indicating the need to assess working conditions and design and implement appropriate prevention strategies because the working conditions of medical waste handlers increase the risk of acquiring HBV and HCV in relation to accidents involving sharps, segregation of sharps and cuts occurring during the disposal of healthcare waste. The high rates of injuries involving sharps represent a health risk for workers collecting healthcare waste. Therefore, there is a need for safe sharps waste management practices in health care facilities together with attitudinal efforts to be made on health care workers and waste handlers for coordinated prevention of viral hepatitis as a national strategic plan of Ethiopia.
Substantial heterogeneity was found in the current study. The significant heterogeneity observed in this study is unlikely to be solely attributed to publication bias. It is plausible that the variations can be attributed to differences in methodological issues such as differences in the sample size, the method of detection, periodic variation of studies, and underlying conditions of patients. The other difference might be attributable to the target groups where samples were taken. For example, medical waste handlers are at higher risk of acquiring viral hepatitis infection than nonmedical waste handlers. Moreover, it can vary in association with the infection prevention and control practices of health facilities as well as waste management practices.
Sensitivity analysis and subgroup analysis were carried out to rule out the most possible causes of heterogeneity. The results of the sensitivity analysis proved that there was no single study that impacted the pooled effect size. The pooled prevalence of HBV and HCV infections in Ethiopia was calculated by omitting each study sequentially, and the computed pooled prevalence was within the 95% CI of the overall pooled prevalence. In addition, publication bias was assessed using funnel plots and Egger’s test statistics, which confirms the absence of publication bias for HBV, while there was publication bias in cases of HCV. Hence, trim and fill analysis was computed. The presence of substantial heterogeneity and the number of studies included in this meta-analysis might be the limitations of this study. Thus, to limit the influence of the study heterogeneity, the random effect Sidik-Jonkman model was implemented in the meta-analyses, and subgroup analyses and sensitivity analyses were performed. Furthermore, molecular data such as HBV and HCV viral load and genotyping were not obtained, which might be another significant limitation despite the present study will provide the general burden of viral hepatitis infections among the target groups. In addition, HBV-HDV coinfection, chronic infection, hepatocellular carcinoma, and cirrhosis were not reported.
Conclusions
The findings of this review showed that the pooled prevalence of HBV and HCV infection among waste handlers in Ethiopia was intermediate and moderate, respectively. This showed that there is a strong need to scale up preventive efforts and strategic policy directions to limit the spread of these viruses. Moreover, we also conclude that handling healthcare and domestic waste is associated with a similar risk of HBV and HCV infection. However, the effect of exposure to waste on workers’ health in both domestic and healthcare settings is increasingly supported by scientific evidence; further studies, such as synopsis of synthesis or guidelines, should prove the association between the risk of handling healthcare and domestic wastes. Furthermore, immunization against HBV as a primary preventive measure should be highly advocated for high-risk individuals such as medical waste handlers. Moreover, vaccination against HBV among waste handlers could be considered and effectively implemented as a preventive measure against HBV.
Footnotes
Acknowledgements
Not applicable.
Author contribution
AG conceived and designed the study. AG, FBG, and SS, participated in article search and AS, YE, HD, and MT participated in duplicate checks and removal. Data extraction was done by AG, SS, HD, and FBG. AG, WD, and MA conducted a quality assessment of the included studies and performed the statistical analysis and interpretation of the data. AG, MA, YK, GMB and EA. drafted manuscript. AG, MA, YK, GMB, SSK, YM, MT, and EA check the validity and monitor the overall process. MT, YM, MA, GMB, WD and AS critically reviewed the manuscript. All the authors read and approved the final manuscript before it was submitted for publication.
Availability of data and materials
All data needed for this research are available within the manuscript and its supporting files.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Informed consent
Not applicable.
Trial registration
The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42023398686.