
Abstract
Background
The incidence of sexually transmitted infections (STIs) remains high among men who have sex with men (MSM) living with human immunodeficiency virus (HIV) (PWH). This study determined the prevalence of asymptomatic STIs in MSM PWH attending an HIV clinic in Mexico City.
Methods
This cross-sectional study (May 2022-November 2023) included self-questionnaires on STI-related behaviors and symptoms, urethral samples for multiplex polymerase chain reaction (PCR), and serological tests for syphilis, HBV, and HCV.
Results
Among 261 patients, 56.7% were receiving antiretroviral therapy, 41.8% had suppressed HIV-1 viral load, and 26.1% tested positive for at least one STI in urethral PCR. The most prevalent microorganisms were Ureaplasma urealyticum (14.9%), Mycoplasma hominis (6.9%), Mycoplasma genitalium (4.2%), and Chlamydia trachomatis (3.1%). Multiple infections were identified in 5.3% of cases. Seroprevalence rates for syphilis, HBV, and HCV were 17.6%, 6.5%, and 3.1%, respectively. Current smoking and insertive anal sex were the only statistically significant associated factors.
Conclusions
This study underscores the high frequency of asymptomatic STIs and the importance of regular screening.
Plain Language Summary
Sexually transmitted infections (STIs) are common among men who have sex with men (MSM) living with human immunodeficiency virus (HIV) (PWH). This study looked at how often these infections occur without symptoms in MSM attending an HIV clinic in Mexico City. From May 2022 to November 2023, researchers collected information from patients using questionnaires about their sexual behaviors and symptoms, took urethral samples to test for STIs, and performed blood tests for syphilis, hepatitis B, and hepatitis C. The study included 261 participants. Over half (56.7%) were on antiretroviral therapy, and 41.8% had undetectable HIV levels. Testing showed that 26.1% had at least one STI in the urethra, even though they had no symptoms. The most common infections were Ureaplasma urealyticum (14.9%), Mycoplasma hominis (6.9%), Mycoplasma genitalium (4.2%), and Chlamydia trachomatis (3.1%). Some participants (5.3%) had more than one infection. Additionally, 17.6% tested positive for syphilis, 6.5% for hepatitis B, and 3.1% for hepatitis C. Smoking and insertive anal sex were the only behaviors linked to a higher chance of infection. This study highlights the high rate of hidden STIs in this population and emphasizes the need for regular STI testing to ensure early detection and treatment.
Keywords
Introduction
Sexual contact can transmit over 30 types of bacteria, viruses, and parasites, including oral, anal, or vaginal sex. 1 Sexually transmitted infections (STIs) are widespread infectious diseases reported globally and represent a significant public health challenge. 2 Among the most prevalent STIs, several are curable, including syphilis, gonorrhea, chlamydia, and trichomoniasis. In contrast, others are incurable but treatable (hepatitis B virus, herpes simplex virus [HSV], human immunodeficiency virus [HIV], and human papillomavirus [HPV]). This has created more significant challenges in providing adequate services for preventing and controlling STIs.1,3
Approximately 85% of new STI cases occur in developing countries. 4 However, rates of gonorrhea, syphilis, and chlamydia infections have substantially increased in high-income countries, particularly among men who have sex with men (MSM).5,6 International guidelines recommend that sexually active MSM people living with HIV (PWH) undergo testing for syphilis, gonorrhea, and chlamydia at least annually. 6 Up to 90% of STIs may not present any symptoms, depending on both the infection and the causative agent. 7 There is a reported prevalence of asymptomatic STIs among MSM PWH of 11% to 19%.6,8–11 In some studies, syphilis has been the most common asymptomatic STI, followed by chlamydia and gonorrhea.6,12,13 When screening for HCV has been included, irrespective of HIV serostatus, the reported prevalence varies from 2% to 13%.14–16
Risk factors for asymptomatic STIs among MSM PWH include chemsex, a recent HIV diagnosis (<7 years), unprotected sexual activity with more than 20 partners in the last 6 months, age under 40 years, high CD4 counts (>450 cells/mm3), and marijuana use.6,11,14
This study examined the prevalence and associated factors of asymptomatic STIs using a multiplex polymerase chain reaction (PCR) urethral swab test, serological tests for syphilis, HBV, HCV, and a questionnaire on high-risk sexual behaviors in MSM PWH at a tertiary hospital in Mexico City.
Methods
This cross-sectional study was conducted from May 2022 to November 2023 at the HIV clinic of the Infectious Diseases Hospital, National Medical Center “La Raza,” Mexico City. The HIV clinic is a tertiary-level reference center for people with social security coverage. After eligibility was verified for interested participants, written informed consent was obtained to collect urethral samples. This study was approved by the Local Committee for Health Research No. 3502 (Approval no. R-2024-3502-254) and the Local Ethics Committee No. 35028 at the Infectious Diseases Hospital, National Medical Center “La Raza.”
For the sample size calculation, a formula for prevalence studies was used with a 95% confidence interval and a 5% margin of error. Given an unlimited population size and based on the prevalence reported in the Willekens et al study (19.9%), 6 20% was assumed because no similar prevalence studies are available for our country.
Men who have sex with men PWH aged ≥18 years were eligible for inclusion in the study if they were sexually active and asymptomatic for STI. People who used antibiotics in the last 30 days, current antibiotic treatment for an STI, patients with signs or symptoms of an STI at the time of evaluation, errors in laboratory report results, and patients who discontinued follow-up or lacked social security were excluded. After this, participants underwent a medical interview, complete physical examination, and responded to a self-administered questionnaire on behaviors and symptoms related to STIs (Braun STI screening ZPHI study). 15 The information obtained from the medical interview and the self-administered questionnaire STI screening ZPHI covered sexual behavior, use of illicit or recreational drugs, chemsex, previous diagnosis of STIs, time since HIV diagnosis, treatment with antiretroviral therapy (ART), and demographic data.
Sexually transmitted infection screening was performed using urethral swabs obtained by multiplex PCR (STD Direct Flow Chip kit®; Vitro S.A.) to detect 11 microorganisms (Chlamydia trachomatis, Neisseria gonorrhoeae, Hemophilus ducreyi, Mycoplasma genitalium, Mycoplasma hominis, Treponema pallidum, Ureaplasma urealyticum, Ureaplasma parvum, Trichomonas vaginalis, HSV 1, and HSV 2). In addition, venous blood specimens were collected for HBV and HCV serology, Venereal Disease Research Laboratory (VDRL), and anti-T. pallidum antibodies, HIV viral load, and CD4 count. For this study, we defined suppressed HIV viral load as a viral load of <40 copies/mL and detectable viral load as ≥40 copies/mL. The patients who tested positive for syphilis, chlamydia, or gonorrhea received appropriate treatment according to national and international clinical practice guidelines. The reporting of this study conforms to the STROBE statement: guidelines for reporting observational studies (Supplemental File). 17
Statistical Analysis
According to their distribution using the Kolmogorov-Smirnov test, quantitative variables were summarized with medians and interquartile ranges (IQRs). Qualitative variables were presented as frequencies and percentages. Categorical variables were recoded into dichotomous ones using the relevant results from other studies.6,11,14 Bivariate analysis was performed to evaluate possible factors associated with asymptomatic STIs and to obtain the odds ratio (OR) using the chi-square and Fisher exact tests. Independent risk factors for asymptomatic STIs were identified through logistic regression analysis, which included variables with P < .05 from the bivariate analysis and calculated with 95% confidence intervals. All analyses were conducted using the SPSS software (version 27; IBM SPSS Corp.).
Results
A total of 261 patients were included in the study, with a median age of 27 years (IQR 23-31). At the time of the study, 56.7% of the participants were on ART, with a median duration of 2 months (IQR 1-11) since HIV diagnosis. Over half of the patients (58.2%) had detectable HIV-1 RNA, and the median HIV viral load was 2667 copies/mL (IQR 40-41 374). The median CD4 count was 398 cells/μL (IQR 228-637). During medical interviews, 242 patients (92.7%) reported being single, 198 (75.9%) reported alcohol consumption, and 106 (40.6%) identified as current smokers. Additionally, 43 patients (16.5%) reported illicit drug use, while 29 (11.1%) disclosed engaging in chemsex practices.
Regarding sexual health and behavior, 99 individuals (37.9%) reported a history of previous STIs. Within the past three months, 92 participants (38%) admitted to engaging in high-risk sexual behaviors, and 112 patients (46.3%) reported not having a stable partner. Notably, 121 patients (50%) indicated involvement in condomless casual sexual encounters. Data on sexual behavior were unavailable for 19 participants (Table 1).
Demographic Characteristics of MSM PWH Who Underwent Multiplex PCR Testing of the Urethra to Detect Asymptomatic STIs.

Abbreviations: ART, antiretroviral therapy; HIV, human immunodeficiency virus; IQR, interquartile range; MSM, men who have sex with men; No, number; PCR, polymerase chain reaction; PWH, people living with HIV; STIs, sexually transmitted infections; RNA, ribonucleic acid.
aPatient data for 19 individuals was lost, including information on the number of sexual partners, risky sexual behaviors, and condom use with steady sexual partners and with casual sexual partners.
bPatient data for 19 individuals was lost, 13 did not answer, and 19 reported having only oral sex.
cThe World Health Organization defines risky sexual behaviors as frequently changing sexual partners, having more than one sexual partner, having sexual contact with casual sexual partners, having sexual contact with sexual workers or their clients, having sexual contact without the use of preservatives, history of a sexually transmitted disease the last year, using alcohol or drugs previously or during the sexual contact.
A total of 68 urethral samples (26.1%) tested positive for at least one of the screened STIs. In 14 patients (5.3%), more than one was detected. U. urealyticum (14.9%), M. hominis (6.9%), M. genitalium (4.2%), and C. trachomatis (3.1%) were the most prevalent (Table 2).
Results of Urethral Multiplex PCR Screen for Asymptomatic STIs in MSM PWH.
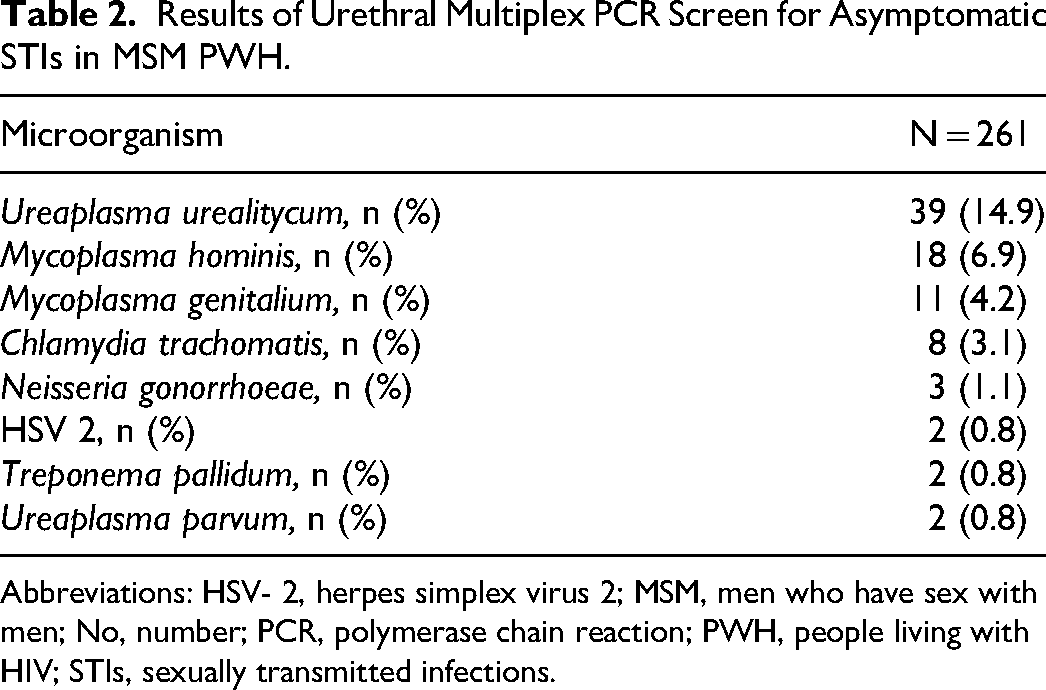
Abbreviations: HSV- 2, herpes simplex virus 2; MSM, men who have sex with men; No, number; PCR, polymerase chain reaction; PWH, people living with HIV; STIs, sexually transmitted infections.
Serology for HBV detected 169 patients (64.8%) with negative anti-HBs antibodies, indicating lack of vaccination, and 17 (6.5%) with positive anti-HBc antibodies, indicating prior infection. Only 75 (28.7%) patients were positive anti-HBs antibodies, indicating previous vaccination. None of the patients in this study was diagnosed with acute or chronic HBV infection.
One patient (0.4%) was diagnosed with chronic HCV infection, and resolved infection was documented in 7 patients (2.7%). Confirmation was performed using HCV viral load in both scenarios.
Syphilis diagnosis (early latent, late latent, and latent of indeterminate duration) was made in 46 patients (17.6%), while 29 patients (11.1%) had a history of treated syphilis.
In the bivariate analysis, current smoking (OR 1.82; CI 95% 1.04-3.18; P = .03) and insertive anal sex (OR 2.44; CI 95% 1.33-4.47; P = .003) were identified as associated risk factors (Table 3). However, in the multivariate analysis using a logistic regression model, only insertive anal sex remained a statistically significant associated factor (OR 2.44; CI 95% 1.33-4.47; P = .004).
Bivariate and Multivariate Analysis of Associated Factors Studied in MSM PWH Who Underwent Multiplex PCR Testing of the Urethra to Detect Asymptomatic STIs.

Abbreviations: ART, antiretroviral therapy; HIV, human immunodeficiency virus; MSM, man who have sex with man; OR, odds ratio; PCR, polymerase chain reaction; PWH, people living with HIV; RNA, ribonucleic acid; STIs, sexually transmitted infections; 95% CI, confidence interval.
aChi-square and Fisher exact tests.
bLogistic regression.
Also, a bivariate analysis was conducted to assess factors associated with syphilis (early latent, late latent, and indeterminate duration). A previous history of STIs was the only statistically significant associated factor (OR 2.82; 95% CI 1.47-5.41: P = .001).
Discussion
This study reveals a notably high prevalence of asymptomatic urethral STIs among MSM PWH, as identified through multiplex PCR testing. U. urealyticum and M. hominis were the most frequently detected microorganisms in urethral samples, while syphilis, diagnosed through serological tests, showed a significant prevalence in this population. Importantly, insertive anal sex was the only statistically significant associated factor for asymptomatic urethral STIs in the multivariate analysis, highlighting its role in STI transmission. Although smoking was associated with asymptomatic STIs in the bivariate analysis, this association did not persist in the multivariate model.
The present study accentuates the association between a prior history of STIs and syphilis in MSM PWH. Several studies consistently highlight this correlation.18–20 A study conducted in Barcelona identified previous syphilis and N. gonorrhoeae infections as risk factors for syphilis among MSM PWH. 18 Similarly, studies in Tokyo and Trinidad found that a history of syphilis infection was strongly predictive of subsequent syphilis diagnoses in this population.19,20 These results reinforce the critical importance of regular STI screening and targeted interventions for syphilis prevention among MSM PWH, particularly given its resurgence despite the availability of screening and effective treatment strategies. 21 Early detection of syphilis is vital to prevent complications such as neurosyphilis, which can cause significant morbidity and disability. Also, the immunopathological interaction between syphilis and HIV transmission highlights the urgency of diagnosis and treatment of this STI. 22
Insertive anal sex emerged as a significant risk factor for asymptomatic STIs in MSM PWH, this being an association supported by previous studies.15,23,24 Braun et al found that engaging in insertive anal intercourse was significantly associated with a higher likelihood of testing positive for STIs in a cohort of MSM PWH, with an OR of 6.48 15 also emphasized the high prevalence of asymptomatic STIs in MSM PWH and the need for regular STI screening, particularly in those engaging in anal intercourse. 23 Similarly, Raccagni et al demonstrated that high-risk sexual behaviors, including insertive anal sex, were strongly associated with C. trachomatis and N. gonorrhoeae infections among MSM PWH. 24 Overall, the evidence suggests that insertive anal sex is a significant risk factor for asymptomatic STIs in MSM PWH.
Studies have shown that smoking may be associated with an increased risk of substance abuse and possibly an increased risk for HIV/STIs.25–27 In the bivariate analysis, we found an association between smoking and asymptomatic STIs. However, it is essential to note that this association has not previously been described in studies involving similar populations. Further research is needed to clarify this relationship in MSM PWH.
Gonorrhea and chlamydia are the most common bacterial STIs in high-income countries. The prevalence of these pathogens is higher in rectal or oropharyngeal samples than in urethral samples. 28 While this study found a relatively low prevalence of N. gonorrhoeae and C. trachomatis in urethral samples, this is consistent with previous reports demonstrating higher detection rates in rectal or pharyngeal samples.6,8,9,11,14 Without treatment, gonorrhea or chlamydia can lead to multiple chronic and irreversible complications, including chronic pelvic pain and infertility, in both men and women.29,30 However, there is debate about the risks and benefits of frequent screening in asymptomatic patients, as this could increase antibiotic resistance to other infections. 31 Also, STIs in PWH have been associated with an increased HIV viral load in the genital tract, which can increase the risk of transmission of HIV. 32 Unfortunately, no rectal or oropharyngeal samples were collected due to limited resources.
Few studies evaluated the prevalence of mollicutes in asymptomatic MSM PWH. The high prevalence of mollicutes found in our patients differed from Kato et al, who reported a prevalence of 8.2% for urine samples, while in our patients, it was 26.8%; however, they did not find N. gonorrhoeae or C. trachomatis in urine samples. 33 Cordova and Cunah reported a prevalence of U. urealyticum and M. hominis in urine and urethral samples, with findings similar to those of this study (18.9% and 7.5%, respectively). 34 Furthermore, de Jesus Salgado et al reported a high prevalence (14.1%) of mollicutes in urethral samples in an MSM population without HIV infection. 35 The high prevalence of mollicutes observed in this study aligns with their role in the genital microbiota of individuals with multiple sexual partners. Complications associated with these pathogens are infertility, nongonococcal urethritis, prostate cancer, and an increased risk of HIV transmission. 36 For the case of M. hominis and U. parvum, the association with nongonococcal urethritis and other complications has been almost null in different studies, and they have been cataloged as colonizing microorganisms.34,35 Current guidelines do not recommend routine screening for mollicutes, and treatment is reserved for symptomatic patients, nongonococcal urethritis where no other causal agent has been identified, and patients with high bacterial loads.
Despite the strengths of this study, several limitations must be acknowledged. Pharyngeal and rectal samples were not analyzed. This is a critical limitation, given that these anatomical sites have reported higher prevalence rates of N. gonorrhoeae, C. trachomatis, and mollicutes. Additionally, this was a single-center, cross-sectional study conducted among insured workers, limiting its generalizability to other populations, such as those accessing different public health systems.
To our knowledge, this is the first study in Mexico to use multiplex PCR to detect 11 microorganisms in asymptomatic MSM PWH. The findings highlight a significant knowledge gap regarding STI prevalence in this population and the urgent need for expanded research and targeted public health initiatives to address asymptomatic STIs in MSM PWH effectively.
Conclusion
The findings of this study highlight the urgent need to implement and reinforce the established recommendations for STI screening as outlined in national and international clinical practice guidelines. The high prevalence of asymptomatic STIs in this population emphasizes the critical importance of prevention strategies, enhancing sexual education programs, and ensuring access to comprehensive and routine STI screening. These measures are essential to reduce the burden of asymptomatic infections and their associated complications, thereby improving overall health outcomes in MSM PWH.
Key Messages
A total of 26.1% of MSM PWH tested positive for at least one asymptomatic urethral STI, with U. urealyticum and M. hominis being the most common pathogens. Additionally, latent syphilis was diagnosed in 17.6% of participants, highlighting the significant burden of this infection.
Insertive anal sex was the only statistically significant associated factor for asymptomatic urethral STIs in the multivariate analysis. A previous history of STIs was significantly associated with syphilis.
These findings highlight the importance of regular STI screening every 3 to 6 months for MSM engaging in high-risk sexual behaviors and every 12 months for others. These efforts aim to reduce the burden of asymptomatic infections and their complications.
The lack of rectal and pharyngeal samples represents a limitation, given their higher reported prevalence for STIs. Further studies are needed to provide a more comprehensive understanding of STI prevalence in MSM PWH.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251321039 - Supplemental material for High Prevalence of Asymptomatic STIs in MSM PWH in a Male HIV Clinic in Mexico City
Supplemental material, sj-docx-1-jia-10.1177_23259582251321039 for High Prevalence of Asymptomatic STIs in MSM PWH in a Male HIV Clinic in Mexico City by Juan Pablo Sánchez Navarro, Gustavo Barriga Angulo, José Antonio Mata Marín, Mara Rodríguez Evaristo, Paola Edith Padilla Noguera and Jesús Enrique Gaytán Martínez in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Authors’ Note
Patient Consent Statement: After eligibility was verified for interested participants, written informed consent was obtained to collect urethral samples. This study was approved by the Local Committee for Health Research No. 3502 (Approval no. R-2024-3502-254) and the Local Ethics Committee No. 35028 at the Infectious Diseases Hospital, National Medical Center “La Raza.” Availability of Data: The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Authors Contribution
Juan Pablo Sánchez Navarro: study design, investigation, formal analysis, writing—original draft, writing—review and editing; Gustavo Barriga Angulo: laboratory support; José Antonio Mata Marín: study design, formal analysis, writing—review and editing; Mara Rodríguez Evaristo: review; Paola Edith Padilla Noguera: review; Jesús Enrique Gaytán Martínez: review, editing, and supervised the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.