
Abstract
A chart review study of the sexually transmitted infection (STI) prevalence among persons living with HIV (PLHIV) was conducted among STI clinic attendees in Trinidad between January 2012 and December 2012. Data were abstracted from client records to obtain the clinical and the laboratory diagnoses of STIs. Descriptive and bivariate analyses were conducted, and factors significantly associated with the presence of a STI were assessed using multiple logistic regression. During this period, 385 PLHIV were seen; 104 (27.0%) were newly HIV diagnosed and 281 (73.0%) had a known history of HIV infection; 135 (35.1%) were diagnosed with a STI. Patients with known HIV infection were more likely to be diagnosed with a STI than those who were newly diagnosed (odds ratios: 6.99; 95% confidence interval: 3.79-12.89). The STI prevalence was high among PLHIV in Trinidad, identifying them as a critical target group for public health interventions to prevent the spread of HIV and STIs.
Keywords
What Do We Already Know about This Topic?
There is evidence of an epidemiological synergy2 between HIV and various STIs which may result in increased HIV acquisition and transmission.
How Does Your Research Contribute to the Field?
This is the one of the few studies in the Caribbean to demonstrate the STI patterns in HIV infected persons.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
The STI prevalence was high among PLHIV in Trinidad, hence targeted and sustained interventions among these patients to reduce STI/HIV transmission are urgently needed.
Introduction
Several studies have established a convincing link between sexually transmitted infections (STIs) and the risk of sexual transmission of HIV infection 1 -4 as there is evidence of an epidemiological synergy 2 between HIV and various STIs which may result in increased HIV acquisition 2,3,5 and transmission. 2,3,6,7 Inflammation or ulceration of the mucosa of the genital tract due to STIs may enhance HIV transmission by increasing the infectiousness of HIV-infected persons and increasing the susceptibility of HIV seronegative individuals to HIV. 2
Sexually transmitted infections in persons with HIV infection may serve as a surrogate for risky sexual behavior and unprotected sexual activity and it is known that untreated STIs increase the risk of sexual transmission of HIV several-fold and increase HIV shedding and susceptibility of the genital mucosa to HIV infection. 2,8
There is biological evidence that HIV shedding is increased in the presence of a STI and that treatment of the STI decreases the shedding of HIV in the genital tract, 9 thus suggesting the potential to reduce HIV transmission. This also indicates that the control of STIs through improved STI prevention, diagnosis, and treatment may have a significant role in HIV prevention efforts. 9 Hence targeted interventions for the prevention, screening, treatment, and control of STIs may disrupt their adverse synergism and substantially reduce HIV transmission. 2
Patients and Methods
The Queen’s Park Counselling Centre and Clinic (QPCC&C) is the main STI clinic in Trinidad with main branches in the north and south of the island where daily walk-in STI clinics are held. As part of the routine standard of care, all patients attending the STI clinic were offered a screening test for syphilis and testing for HIV antibodies.
A chart review study of STI prevalence among persons living with HIV (PLHIV) was conducted among patients who attended the STI clinic in Trinidad between January 2012 to December 2012. Patients who tested HIV seropositive for the first time were considered to be newly diagnosed with HIV infection. Patients who had a previous diagnosis of HIV infection (those referred from the HIV clinic or those who admitted to being HIV infected) were considered as known to be HIV infected.
Inclusion Criteria
All persons attending the STI clinic during the study period who were diagnosed HIV positive (both newly HIV diagnosed and known HIV-positive patients) were included.
Exclusion Criteria
HIV seronegative individuals were excluded. As part of the routine standard of care at the STI clinic, all patients underwent an ano-genital examination by a physician to determine the presence of ano-genital abnormalities, for example, genital discharge, genital ulcers, genital warts, or skin lesions and these were documented. Specimens were collected from the urethra of males and the urethra, cervix, and posterior fornix of females and sent to the onsite laboratory for smear (wet prep for Trichomonas vaginalis and bacterial vaginosis, gram-stained smear for gonorrhea in men, and Tzanck smear for herpes simplex), culture (on Thayer Martin media for gonorrhea), and dark field microscopy (Treponema pallidum).
In patients with genital ulcers, the base of the lesion was scraped, material was obtained for the Tzanck test and serous exudate was obtained for dark field microscopy. In the Tzanck smear, the specimen was examined for the presence of the characteristic multinucleated giant cells typical of herpes viruses. Darkfield microscopy was used to detect T pallidum directly from lesion exudate as a delicate, tightly spiraled, corkscrew-shaped organism with its typical motility. In men, gonorrhea was diagnosed when gram-negative intracellular diplococci were seen on gram-stained smears of urethral exudates; and in men and women by culture on Thayer Martin media and the isolation of an oxidase positive, gram-negative diplococcus. Nongonococcal urethritis/cervicitis was diagnosed if there were ≥ 10 polymorphonuclear leukocytes per high-power field in the absence of gonorrhea. The results of the smears, dark field microscopy and Tzanck smears were obtained within 30 minutes so that the patient would have appropriate same day treatment.
The QPCC&C Laboratory is the reference laboratory for STI testing in Trinidad. Standardization and external quality proficiency assessment is performed quarterly through Oneworld Accuracy Canada to assess, monitor, and improve the reliability and accuracy of the diagnostic tests. 10 Testing for syphilis was carried out by screening sera with a quantitative Venereal Disease Research Laboratory (VDRL) (Becton, Dickinson and Company, Franklin Lakes, New Jersey) and all reactive samples were confirmed with the Microhemagglutination Assay for Treponema Pallidum Antibodies (Sera-Tek kits, Fujizoki Pharmaceutical Co, Ltd, Tokyo, Japan).
Each study participant was allocated a unique identifying number to protect patient confidentiality and data were abstracted from the medical records of all study cases. Data collected included age, sex, date of visit, HIV status (newly diagnosed and known HIV infection), reason for visit, and the STI diagnosis. The research was focused on the use of routinely collected data using the routine predesigned pro forma surveillance form used for all clients visiting the clinic, which captured all the study variables. Data were also abstracted from the medical records of clients and the laboratory logbooks to obtain the clinical diagnosis and the laboratory diagnosis of STIs.
Ethical Approval and Informed Consent
The study protocol was approved by the Ethics Committee of the Faculty of Medical Sciences University of the West Indies, Eric Williams Medical Sciences Complex, Trinidad.
Data Collection and Data Analysis
All data collected on the structured surveillance forms and from the clinical and laboratory records were analyzed using IBM Statistical Package for Social Science (SPSS) version 22. Numerical variables were summarized using the mean, standard deviation, and range, and the means were compared using the independent samples t test. Chi square tests (χ2) or Fisher exact test was used as appropriate to examine differences in categorical variables by sex, clinic site, HIV status, and STI infection. Bivariate logistic regression analyses were conducted to examine associations between the independent variables and the presence of STI infections. The results were presented as odds ratios (95% confidence interval [CI]).
To identify the independent predictors of STI infections, multiple logistic regression analyses were conducted. The independent variables included age, sex, and all the variables that were significant in the bivariate analyses.
Results
A total of 385 PLHIV were seen during the period of study, 168 (43.6%) were males and 217 (56.4%) were females. The age range was 16 to 77 years and the median age was 34.0 years. Of these, 104 (27.0%) were newly HIV diagnosed and 281 (73.0%) had a known history of HIV infection (Table 1). Among those newly diagnosed, there was a significantly higher proportion of men than among those with known HIV (P = .004). Additionally, the percentage of persons from the north clinic was significantly higher among the newly diagnosed, than among those with known HIV (P < .001).
Baseline Characteristics of Study Population by HIV Status (Newly Diagnosed or Known HIV Infection).a

a n = 385. Boldface values are statistically significant.
Sexually Transmitted Infections
One hundred thirty-five (35.1%) of the 385 HIV-positive study patients were diagnosed with a STI (Table 2). The STIs reported included syphilis 51 (13.2%), genital warts 46 (11.9%), nongonococcal urethritis/cervicitis (NGU/NGC) 27 (7.0%), gonorrhea 6 (1.6%), genital herpes 17 (4.4%), and Trichomonas vaginalis 6 (1.6%; Table 2). Among the 135 HIV-positive study patients with a STI, one STI was diagnosed in 117 (30.4%) patients and 2 concurrent STIs were diagnosed in 18 (4.7%).
Sexually Transmitted Infection Prevalence by HIV Status (Newly Diagnosed and Known HIV Infection).a

Abbreviations: CI, confidence interval; NGU/NGC, nongonococcal urethritis/cervicitis; OR, odds ratios.
a n = 385.
Table 2 shows the STI prevalence stratified by HIV status (newly diagnosed or known HIV Infection). Patients with known HIV infection were almost 3 and a half times as likely to be diagnosed with any STI compared with patients newly diagnosed with HIV infection (odds ratios [OR]: 3.41; 95% CI: 1.95-5.97). These significantly increased odds held true for syphilis (OR: 3.11; 95% CI: 1.29-7.54); genital warts (OR: 3.38; 95% CI: 1.30-8.81); and nongonococcal urethritis (OR: 4.98; 95% CI: 1.16-21.41). There were no stastically significant differences between new and known HIV cases for gonorrhea, herpes, or Trichomonas infections.
Table 3 shows the STI prevalence stratified by sex. On aggregate, there was no statistically significant difference in overall STI prevalence by sex (OR: 1.05; 95% CI: 0.69-1.60). However, males were twice as likely compared to females to be diagnosed with syphilis (OR: 2.23; 95% CI: 1.22-4.07) and were 25 times less likely to be diagnosed with nongonococcal urethritis/nongonococcal cervicitis than women (OR: 0.04; 95% CI: 0.01-0.33). There were no statistically significant differences between the other individual STIs and sex of patient.
Sexually Transmitted Infection Prevalence by Sex.a
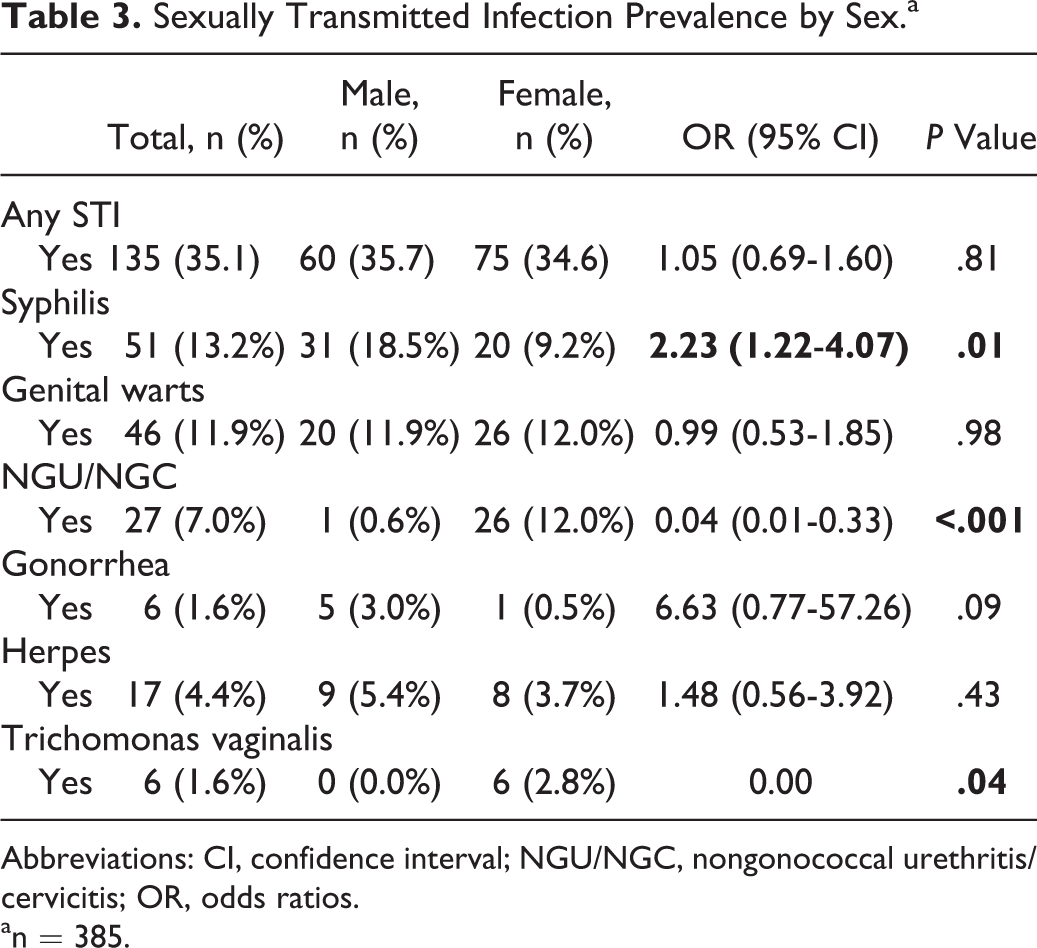
Abbreviations: CI, confidence interval; NGU/NGC, nongonococcal urethritis/cervicitis; OR, odds ratios.
an = 385.
Multivariate analysis using logistic regression (Table 4) showed that STIs were more likely to be diagnosed in patients with known HIV infection compared to those newly diagnosed with HIV (OR: 6.99; 95% CI: 3.79-12.89) and among study patients who attended the north clinic compared to those who attended the south clinic (OR: 6.65; 95% CI: 3.86-11.46).
Results of Multivariate Logistic Regression of the Independent Risk Factors for Having a STI Among HIV Infected Patients.
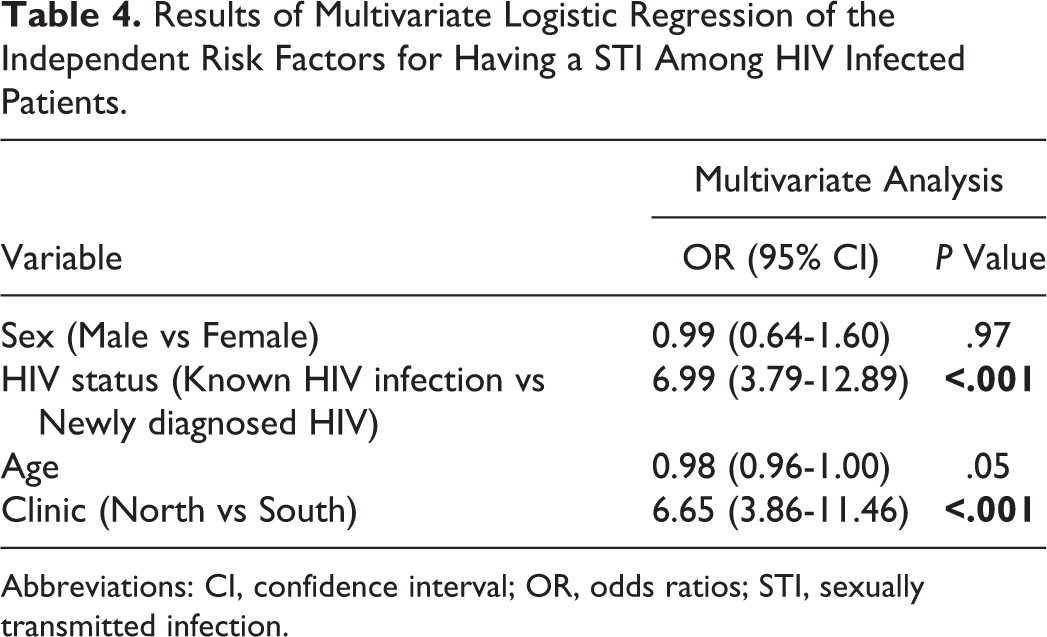
Abbreviations: CI, confidence interval; OR, odds ratios; STI, sexually transmitted infection.
Discussion
The prevalence of STIs among PLHIV in the study was 35.1%. The most commonly reported STIs included syphilis (13.2%), genital warts (11.9%), nongonococcal urethritis/cervicitis (NGU/NGC; 7.0%), genital herpes (4.4%), gonorrhea (1.6%), and Trichomonas vaginalis (1.6%). Our findings of high levels of STI/HIV coinfection in PLHIV is consistent with findings in the literature in other regions and settings. 11 -14 In a study by Baffi et al, 15 of 1544 HIV-infected patients attending a HIV clinic in the Southeastern United States, there were 40 (2.6%) incident cases of syphilis identified, the majority were male (76%) and men who have sex with men (MSM; 57%). 15 On the contrary, asymptomatic STIs were common in women and MSM, 15 hence warranting the need for more frequent screening in these populations. 16 In 2002, the United Kingdom implemented a chlamydia screening program for women and men under the age of 25 in clinical and nonclinical settings. 17
Multivariate analysis using logistic regression showed that that STIs were significantly more likely to be diagnosed in patients who attended the north clinic compared to those who attended the south clinic (OR: 6.65; 95% CI: 3.86-11.46). The results support the national STI statistics that most persons diagnosed with STIs are from areas in the north of Trinidad. 18 In addition, the daily attendance of clients to the north clinic is approximately twice that of the south clinic and there is a widely held view that some HIV/STI clients (especially those from south Trinidad) may go to clinics far away from their area of residence to avoid being recognized, stigmatized, and discriminated against. 19
Control of STIs include appropriate epidemiologic targeting of high-risk groups (eg, sex workers, MSM) through outreach and peer interventions, the promotion of increased education, and awareness programs to reduce HIV incidence among HIV-negative high-risk populations and also the reduction of comorbidities associated with HIV and STI infection in PLHIV. 20 In addition to primary prevention measures including the importance of the promotion of routine HIV/STI screening, condom distribution, increased condom use among high-risk populations, and the creation of an “enabling” environment for prevention are imperative. 2,9,21
Multivariate analysis using logistic regression showed that STIs were significantly more likely to be diagnosed in patients with known HIV infection as compared to those newly diagnosed with HIV (OR: 6.99; 95% CI: 3.79-12.89), so interventions among PLHIV and their sexual contacts (including disclosure of seropositive status) are needed. There are many challenges to the control of HIV especially among high-risk populations and a combination prevention approach is preferred. 23 This includes HIV testing and counseling, condom promotion, behavioural risk reduction, screening, diagnosis, and treatment of STIs, the treat-all strategy, 24,25 where all PLHIVs are offered antiretroviral therapy to suppress their viral loads reducing HIV transmissibility and pre-exposure prophylaxis. 26,27 In other settings, safe male circumcision and needle exchange programs form part of the combination package of services. 23 Training of health-care workers (HCW) is important as PLHIV may experience stigma and discrimination (from HCW) which may contribute to low self-esteem, negative self-image, increased sexual risk taking behavior, and reduction in the use of HIV prevention services. 23
Comprehensive clinical services include the clinical management of symptomatic STIs to shorten infectivity, screening for asymptomatic STIs, partner notification approaches to break the chain of infection, HIV testing and counselling of STI patients, pre-exposure immunization of persons at risk for vaccine preventable STIs (hepatitis B and human papillomavirus), and appropriate counselling and education services. 2,9,23
Before the introduction of combination antiretroviral therapy as treatment for HIV, there were many public health programs and AIDS awareness campaigns directed initially to the MSM community and later to the general population. 28 Therefore, during the 1980s, there was a decline in the prevalence of STIs among MSM in developed countries suggesting behavior change. 23,28,29 Advances in antiretroviral therapy and improvements in HIV management resulting in increased quality of life and survival have been beneficial for PLHIV, but may have had a negative impact on sustainability of engagement in protective health behavior in high-risk populations. 30,31 In recent times, the resurgence of syphilis among MSM in developed countries has been associated with coinfection among PLHIV, multiple sexual partners, and recreational drug use. 22,30,31
Prevention programs for PLHIV should be strengthened, including the motivation of HIV-infected individuals to embrace prevention and essential services which promotes healthy lifestyles through education and awareness campaigns, adherence to Highly active antiretroviral therapy (HAART) regular screening for STIs among high-risk groups (like MSM and sex workers), and safeguards for partner health including disclosure support. 23 In addition, training of HCW should be carried out to reduce stigma and discrimination of PLHIV. 2,23
The scope of our study design is limited because it is from an existing database, where questions were captured a priori, hence we were not able to capture important demographic variables that may have acted as moderators or confounders. For instance, we were not able to identify the sexual orientation of the patients so we could not compare STIs in heterosexual men and MSM. Other potential unmeasured confounders included condom use, alcohol and illicit drug use, and the number of sexual partners. However, these data unavailable and are potential limitations of the study. We are likely to have underestimated the prevalence of STIs among PLHIV attending the STI clinic in Trinidad because there were neither facilities available to test for Chlamydia nor equipment for anal smears/testing. Some testing modalities used in this study have limited sensitivity to diagnose STIs including the diagnosis of nongonococcal urethritis/cervicitis and the Tzanck smear used to diagnose genital herpes simplex infection. Despite these limitations, the study clearly showed that STIs remain a problem among PLHIV. In addition, these results should not be generalized to the general population of PLHIV in Trinidad as persons who attend the STI clinic are probably not a representative sample.
Conclusions
This is the one of the few studies in the Caribbean to demonstrate the STI patterns in HIV-positive persons. 32 Sexually transmitted infections are relatively common among PLHIV attending the STI clinic in Trinidad. Persons who are already aware of their HIV status, and who might be expected to be more cautious, are demonstrating higher rates of STIs as compared to those whose HIV status was previously unknown to them. Targeted and sustained interventions among PLHIV to reduce STI/HIV transmission are urgently needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.