
Abstract
Background
Using data from a national cohort study and focus groups, the Women-Centred HIV Care (WCHC) Model was developed to inform care delivery for women living with HIV.
Methods
Through an evidence-based, integrated knowledge translation approach, we developed 2 toolkits based on the WCHC Model for service providers and women living with HIV in English and French (Canada's national languages). To disseminate, we distributed printed advertising materials, hosted 3 national webinars and conducted 2 virtual capacity-building training series.
Results
A total of 315 individuals attended the webinars, and the average WCHC knowledge increased by 29% (SD 4.3%). In total, 131 service providers engaged in 22 virtual capacity-building training sessions with 21 clinical cases discussed. Learners self-reported increased confidence in 15/15 abilities, including the ability to provide WCHC. As of December 2023, the toolkits were downloaded 7766 times.
Conclusions
We successfully developed WCHC toolkits and shared them with diverse clinical and community audiences through various dissemination methods.
Plain Language Summary
Why was the study done?:
The research team created the Women-Centred HIV Care (WCHC) model to help healthcare providers deliver personalised and thorough care to women living with HIV in Canada. This study aimed to develop a practical toolkit based on the model. The goal was to share this toolkit with women and their providers in various ways to get feedback on its usefulness and to understand the best methods for sharing tools in the future.
What did the researchers do?:
Through an in-depth, collaborative process, English and French WCHC toolkits were developed by a large and diverse team of women and providers. Various methods including printed materials, national webinars and virtual trainings were used to share the toolkits across Canada. The team assessed the toolkit's reception by using surveys, focus groups and tracking toolkit downloads and webpage views.
What did the researchers find?:
The study found positive results, including a 29% increase in WCHC knowledge for 315 webinar participants and enhanced confidence in 15 abilities for 131 service providers during virtual training. The toolkits were downloaded 7766 times, indicating broad interest. Usability testing showed that the toolkits were easy to use and helpful. Attendees of the webinars and virtual trainings indicated they were likely to use the toolkit and recommend it to others.
What do the findings mean?:
Overall, the WCHC toolkits offer valuable guidance to women living with HIV and their providers. The study improved providers’ knowledge and confidence in delivering WCHC, especially during the virtual training sessions that focused on applying this knowledge to real clinical cases. During months when the toolkit was shared through printed materials, webinars and virtual training, more people visited the toolkit webpage. The study highlighted the importance of involving those who will use healthcare tools from the beginning and using many ways to share these tools to reach more people.
Keywords
Background
In Canada, women represent one quarter of all people living with HIV. 1 Gender inequalities in HIV prevention, acquisition and care leave women vulnerable to adverse social and health impacts. 2 Women living with HIV in Canada have lower rates of care retention, 3 antiretroviral therapy adherence, 4 and HIV viral suppression 1 than men with HIV. Clinical care of women living with HIV is influenced by a unique set of social issues including gender-based power imbalances, past experiences of trauma, fear of disclosure and violence, and sexism.5‐10 Nevertheless, comprehensive health considerations for women living with HIV are not often recognized in HIV care, with previous research finding more than 50% of women living with HIV reported at least 1 gap in comprehensive care, including not receiving Pap testing and mammograms per guidelines. 11 The 2018 World Health Organization's Consolidated Guideline on Sexual and Reproductive Health and Rights of Women Living with HIV calls for a women-centred approach to HIV care that addresses intimate partner violence, autonomy and choice and broad social determinants of health. 2 Created as a result of these guidelines, the Canadian National Action Plan, 12 as well as the global movement towards care that emphasises the holistic needs of the person, 13 demonstrates the need to strengthen comprehensive, women-centred models of care and to create tools to assist healthcare providers in implementing these principles.14‐17
Between 2010 and 2018, we carried out the largest national community-based cohort study of women living with HIV in Canada, the Canadian HIV Women's Sexual and Reproductive Health Cohort Study (CHIWOS) with 1422 women from British Columbia, Ontario and Quebec across 3 time points. 18 Based on the findings from CHIWOS and the existing women-centred model used at the Oak Tree Clinic in Vancouver, 19 we developed the ‘Women-Centred HIV Care (WCHC) Model’ to inform care delivery to women living with HIV (Figure 1). 20 Extensive information on CHIWOS and the development of the model has been previously published.20,21 The WCHC Model is an evidence-based, integrated care model that is depicted in the shape of a house to represent safety and stability. The model comprises 6 components: (1) trauma- and violence-aware care, (2) person-centred care with attention to social determinants of health and family, (3) women's health care including sexual and reproductive health and rights, (4) mental health and addiction care, (5) HIV care and (6) peer support, leadership and capacity building. Flexible application is intended to address the priorities of diverse women living with HIV across their life course.
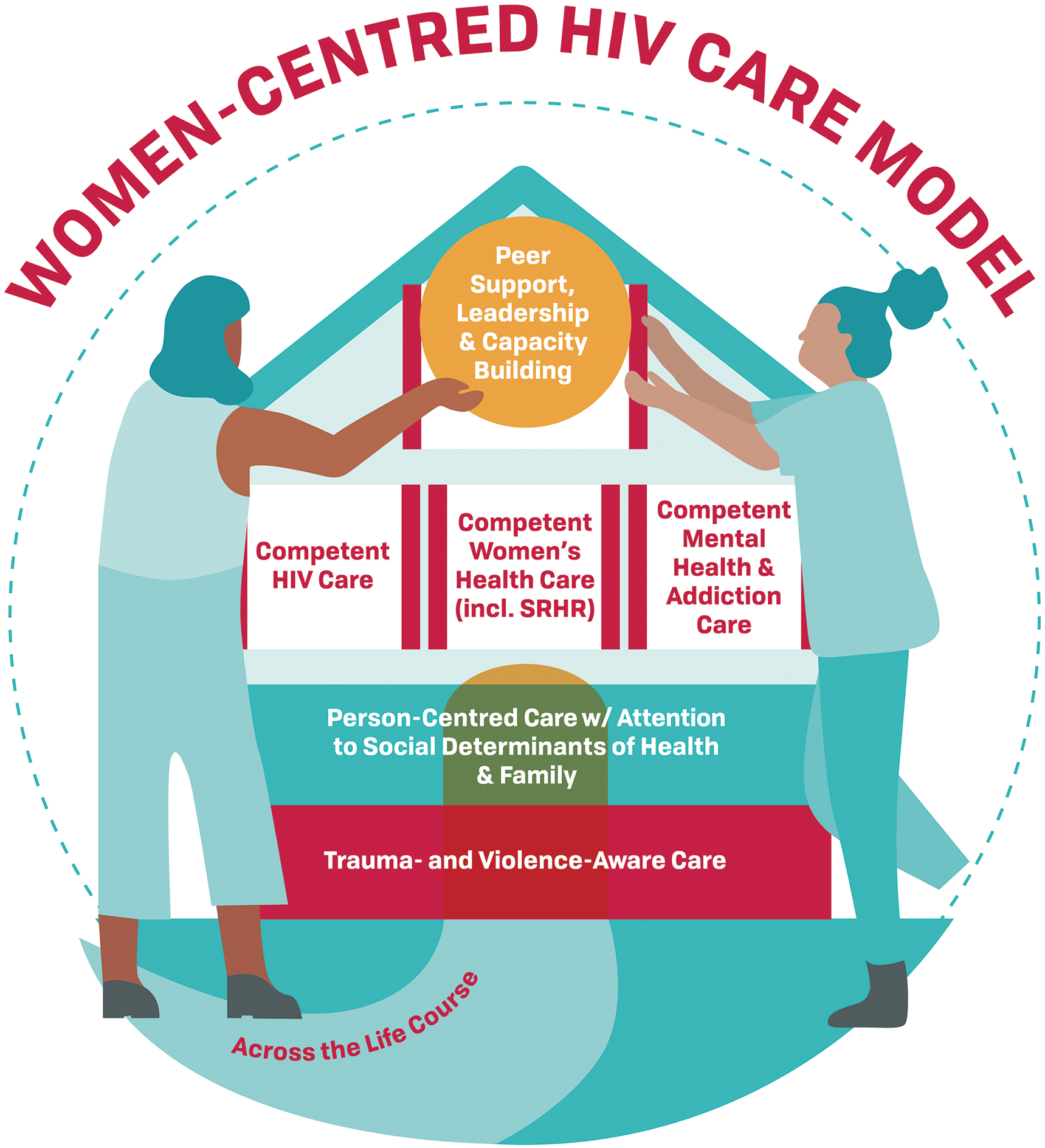
The Women-Centred HIV Care Model.
Despite strategies to facilitate uptake, experts note that there is often a considerable time lag between the evidence-based knowledge generation from research and the practical implementation of that knowledge.22,23 This is problematic given that the optimal use of guidelines and the integration of self-management into care delivery may improve the health status of patients with chronic conditions. 24 Focused efforts are essential to improving healthcare quality and system efficiency and ensuring maximum value from research investment. 25 Relatedly, active knowledge dissemination strategies (e.g. trainings, presentations, use of organisational champions,) have been found to be more effective than passive efforts (e.g. scientific publication, flyers, websites or email blasts) in increasing uptake of health-related evidence. 26 For instance, creating tools based on clinical guidelines, models and best practices has been found to have a significant impact on the uptake of recommendations. 27 A relevant example is the step-by-step, practical toolkit the Agency for Healthcare Research and Quality, a division of the U.S. Department of Health and Human Services, created to guide healthcare organizations in implementing the Chronic Care Model, one of the most widely used models of care. 28
Following a similar approach while embedding community-based research principles, 29 2 easy-to-use toolkits based on the WCHC Model were created as part of this study. Subsequently, a multimodal dissemination strategy was developed using population-specific active and passive knowledge translation methods.30,31 In this paper, we describe the development of the WCHC toolkits through knowledge-to-action and evidence-based integrated knowledge translation approaches developed by the Centre for Effective Practice (CEP). 32 We then evaluate the national dissemination of the model and toolkits through several methodologies.
Methods
Toolkit Development
The WCHC toolkits were developed over 20 months (2018-2020) by a multidisciplinary team (including women living with HIV, researchers and service providers) in collaboration with the CEP, a not-for-profit knowledge translation organization. The CEP's iterative and systematic approach to toolkit development, outlined in Figure 2, has been successfully applied to develop over 70 tools and resources 32 and has parallels to our team's community-based research principles. 29
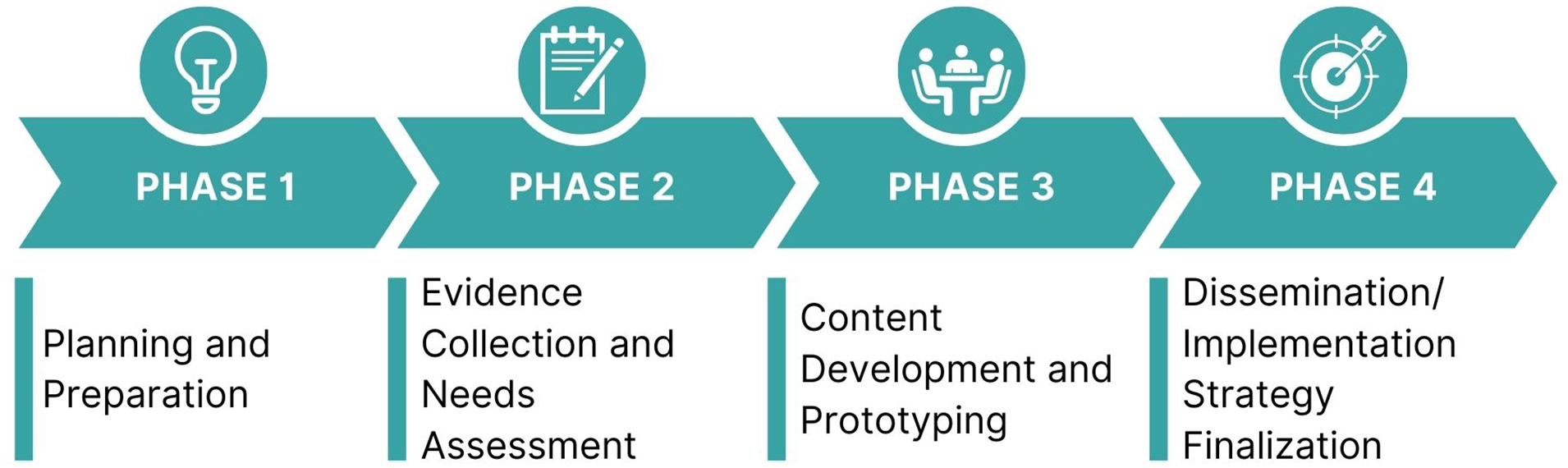
CEP toolkit development process.
Phase 1: Planning and Preparation
We began by identifying the toolkits’ purpose – to advance the WCHC Model into an evidence-based tool for practical use. To maximise usability by diverse end users, 2 versions were planned: 1 for clinicians and service providers to inform practice, and another for women living with HIV to use as a health self-management tool. Six small groups, each led by a clinical and a community chair with expertise in the relevant area, focused on the different components of the WCHC Model. The toolkits’ scope, key objectives and content plan were determined by these groups at a 2-day in-person meeting in 2018 and finalized through email.
Phase 2: Evidence Collection and Environmental Scan
To inform toolkit content, we conducted a systematic literature search and appraised 121 clinical practice guidelines from Canada, the United States, United Kingdom, European Union and the WHO using the AGREE II instrument. 33 Simultaneously, we conducted an environmental scan to identify stakeholders for toolkit usability testing. Team members were consulted on both the evidence collection and needs assessment to provide feedback.
Phase 3: Content Development, Prototyping and Usability Testing
We extracted content from 53 of the guidelines appraised in phase 2, with section-specific content assessed by component leads and team members. We invited women living with HIV from our existing networks in Ontario and British Columbia, as well as others identified in phase 2 to take part in usability testing. We utilised purposive sampling in our recruitment efforts, attempting to reach women from diverse sociodemographic backgrounds. The testing, which included focus groups (for women) and one-on-one interviews (for providers), asked participants to share insights on toolkit usability, content and terminology appropriateness and impressions of the proposed dissemination strategy.
Phase 4: Dissemination Strategy Finalization
Based on usability testing feedback, our team finalized the multimodal dissemination strategy (Figure 3) and evaluation plan.

Evidence-based development and implementation process of the WCHC Model and toolkits.
Dissemination and Evaluation
Passive Dissemination: Email Launch and Print Materials
The English toolkits were strategically launched online during the virtual 23rd International AIDS Conference (AIDS 2020) and shared broadly through email and social media. The French toolkit was subsequently launched on World AIDS Day 2020. We created, printed and distributed bilingual flyers, posters and postcards tailored for both women and service providers in Ontario and British Columbia. These print materials featured clear, audience-specific messages in addition to a QR code and shortened URL for convenient access. We evaluated these methods by correlating the monthly increase in traffic to the toolkit webpage with the timing of sharing email and print materials.
Passive Dissemination: National Webinars
In partnership with the Canadian AIDS Treatment Information and Exchange (CATIE), Canada's official knowledge broker for HIV and hepatitis C,
34
we hosted 3 national webinars (2 English webinars in October 2020 and 1 French webinar in March 2021). Interactive aspects included polls gauging attendees’ pre-webinar knowledge level of issues affecting women living with HIV (for the service provider webinar) and the frequency of person-centred care experiences and peer leadership activity participation (for the women's webinar). Presenters included women living with HIV, researchers, clinicians, and members of community-based organizations, and each session was opened and closed by an Indigenous Elder. The 3 distinct webinars included:
English: For women living with HIV and community-based service providers, this webinar provided an overview of the women's toolkit as a self-health advocacy tool. English: For clinicians and service providers, this webinar aimed to share evidence-based recommendations for caring for women living with HIV and strategies to support the use of the service provider toolkit in practice. French: For both groups, this webinar explored aspects of both the women's and service provider toolkits.
Participant demographic information was collected upon registration. During the webinar, the webinar software automatically calculated an ‘interest rating’ for each attendee, which considered several factors including engagement with Q&A, attentiveness and attendance length.
35
Post-webinar surveys assessed participant satisfaction, knowledge gain and content appropriateness, providing an opportunity for attendees to share their intended use of the information and main takeaways.
Active Dissemination: Project ECHO® Virtual Training
Next, we created a virtual capacity-building training based on the WCHC service provider toolkit utilizing the Project Extension for Community Healthcare Outcomes (ECHO)® model. 36 The ECHO® model, initially developed by Dr Sanjeev Arora in New Mexico, USA to expand Hepatitis C care capacity in rural practitioners, has seen global adoption, featuring nearly 7000 programs and engaging over 5 million participants in 195 countries. 36 ECHO® uses Zoom to connect remote general practitioners (spokes) to an academic specialist team (hub) to build capacity in a specific topic area (Figure 4). During these sessions, approximately 20 min are dedicated to didactic teaching by a hub member, followed by a spoke presentation of a real patient case, usually related to the didactic topic, for clinical guidance.
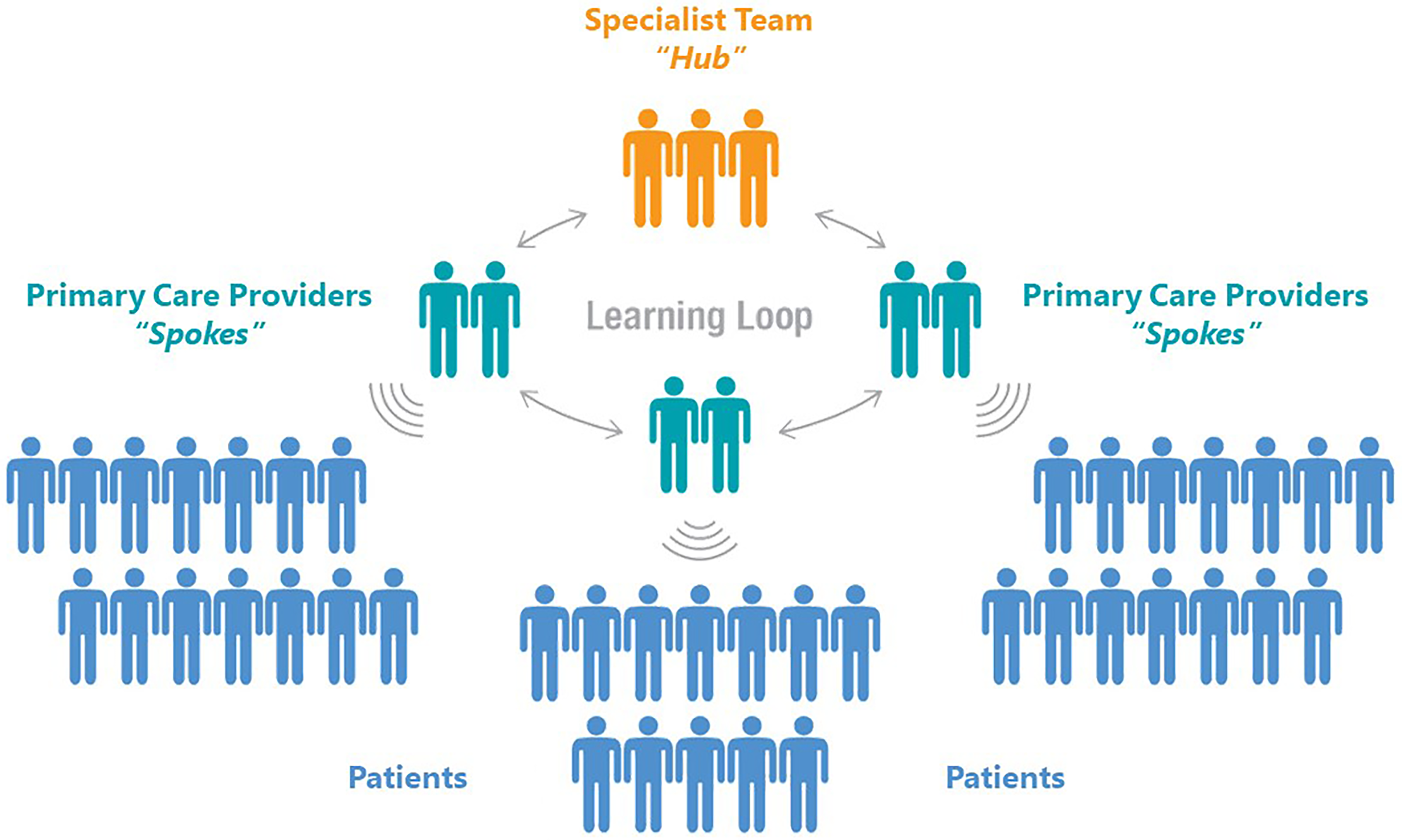
Project ECHO® model.
We conducted 2 cycles of Project ECHO®: WCHC, starting with a provincial pilot in Ontario from October 2021 to June 2022. This cycle involved 13 sessions, each addressing a different aspect of the model/toolkits. The findings from this provincial pilot then informed a national expansion of Project ECHO®: WCHC across Canada, which consisted of 9 sessions held from October to December 2022. Our team uniquely incorporated community-based research principles into the conventional ECHO® model, consistently featuring co-presentation of didactic material by 1 clinical and 1 community hub member.
We obtained continuing medical education (CME) accreditation from the University of Toronto's Faculty of Medicine for both cycles, allowing spokes to claim up to 1 hour of CME credits per session. Our recruitment efforts included distributing flyers through our own networks as well as established channels including the HIV Outpatient Clinic Network, the Ontario chapter of the Canadian Association of Nurses in AIDS Care, and family medicine residency programs and infectious disease fellowship programs in Ontario. For the national cycle, we expanded our outreach to include over 50 residency programs, community-based organisations, nursing and medical alumni networks, as well as infectious disease and primary care clinics across Canada.
For both cycles, evaluation data were gathered through quantitative surveys administered at several time points (including after each session, as well as pre- and post-ECHO cycle) via REDCap, a secure online survey database. The evaluations sought to quantify several metrics including spoke's self-efficacy, satisfaction, knowledge and change in practice associated with participating in the training. At the end of the Ontario cycle, all hub and spoke members were invited via email to participate in a virtual focus group to gather insights to inform the national cycle.
Ethical Approval and Informed Consent
For toolkit usability testing with women, ethics approval was obtained from the Research Ethics Boards of Women's College Hospital (ON), Simon Fraser University (BC) and the University of British Columbia/Providence Health (BC). Focus group participants provided informed consent. For toolkit usability testing with clinicians, recruitment and consenting were managed by the CEP. Project ECHO®: WCHC was formally reviewed by institutional authorities at Women's College Hospital (ON) and was deemed not to require Research Ethics Board approval. Instead, we obtained approval through the Women's College Hospital Assessment Process for Quality Improvement Projects pathway (APQIP). Participants received APQIP-approved email invitations for the evaluation project, emphasising voluntary participation and the confidentiality of responses. All Project ECHO®: WCHC focus group participants completed APQIP-approved informed consent forms.
Results
Toolkit Usability Testing
Women's Toolkit Usability Testing with Women Living with HIV
Eight focus groups were conducted (5 in Ontario and 3 in British Columbia) in small, medium and large municipalities. Fifty-one self-identified women living with HIV participated (34 in Ontario, 17 in British Columbia). The participant group was diverse in terms of race and ethnicity, with 47% identifying as White, 32% identifying as African, Caribbean and Black, 13% identifying as Indigenous and 2% each identifying as Latin, Asian, Middle Eastern/North African and Other.
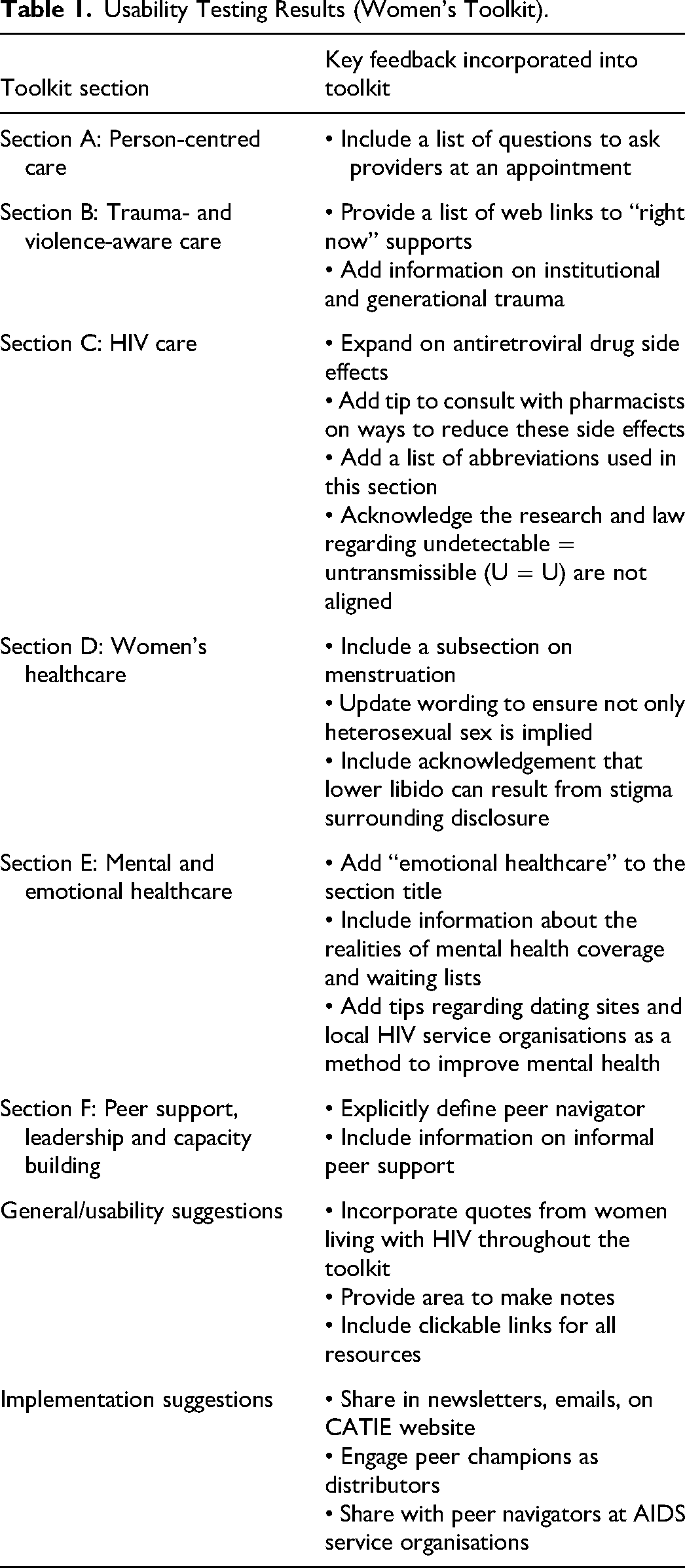
The key recommendations resulting from the usability testing are included in Table 1. Most participants stated they would recommend the toolkit with the changes they suggested, and that the toolkits would have an impact on women's lives and health. Participants emphasised the gap in care this toolkit filled, with 1 participant sharing: ‘When I go to the hospital there are kits for men and there are not many kits that are designed for us women’. It was noted that the toolkit would serve as a great resource for recently diagnosed women, as several recalled being given little to no information on women-specific services after diagnosis: ‘I was given a stack of papers about cervical cancer’. Additionally, participants emphasised the importance of this tool for immigrant women who may be less familiar with the health and social service systems in Canada.
Usability Testing Results (Women's Toolkit).
Service Provider Toolkit Usability Testing with Service Providers (Conducted by CEP)
The service provider toolkit prototype was shared in 11 one-on-one interviews with providers from 4 provinces (Ontario, Saskatchewan, British Columbia, Alberta). This included infectious disease specialists (n = 4), community-based workers (n = 3), registered nurses (n = 2), a family physician (n = 1) and a nurse practitioner (n = 1). These providers were representative of the target population as many worked in HIV-specific clinics or organisations and provided direct service to hundreds of people living with HIV across the country. Feedback from these interviews is summarized in Table 2.
Usability Testing Results (Service Provider Toolkit).
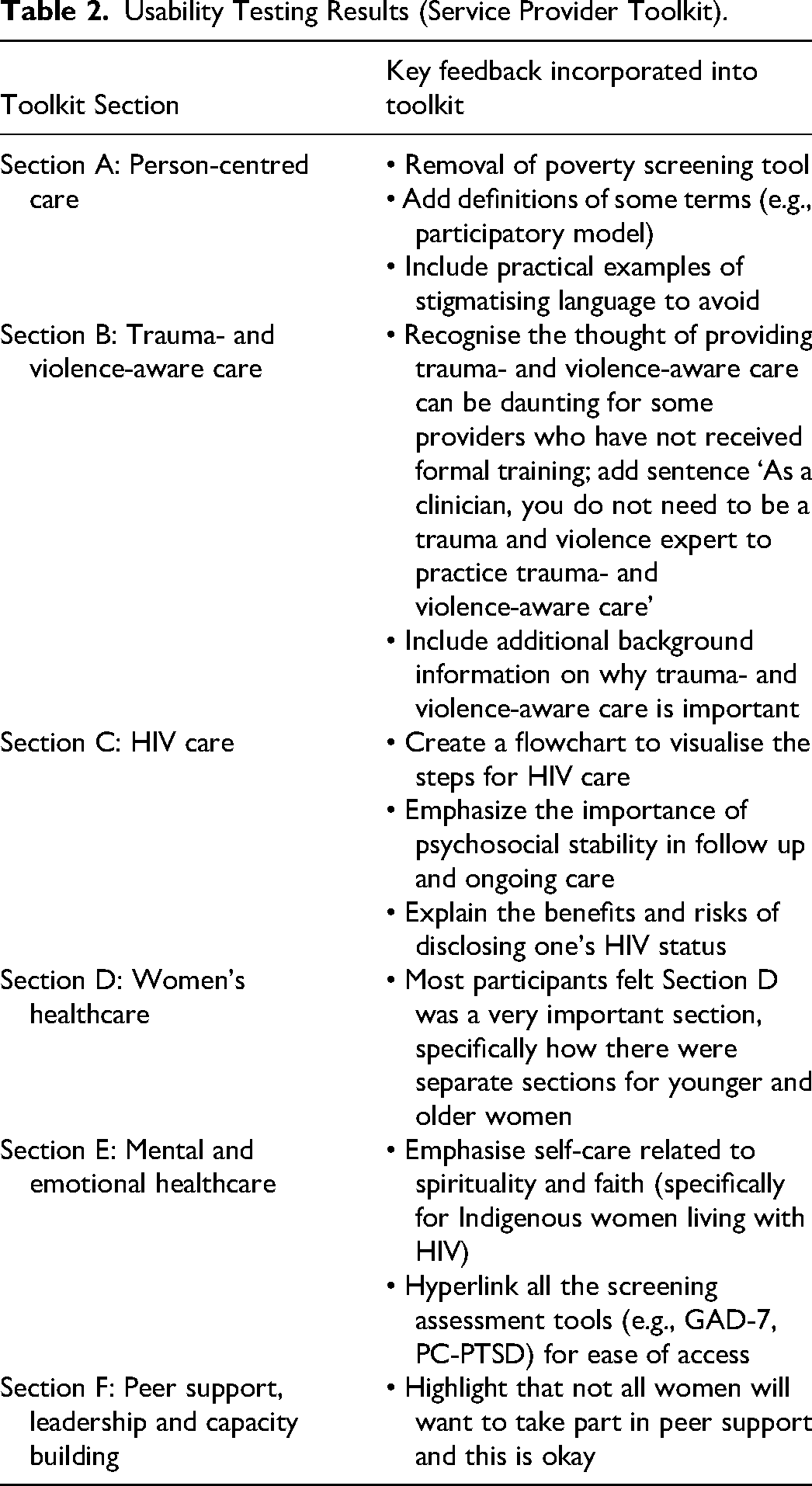
The participants were asked what they believed was the most important message for clinicians caring for women living with HIV. Answers included better understanding the stigma women face, acknowledging their resilience and the importance of working with women one-on-one to assess their needs based on culture, behaviours and concurrent conditions – all of which the participants agreed were explored in the toolkit. One participant highlighted a historical disparity in educational materials concerning HIV, emphasising that existing resources are designed for gay men as the target audience,leaving a significant void for women. They agreed that the toolkit effectively bridged this long-standing gap. All participants reported that they liked the toolkit, they would use it in their practice, and they would recommend it to other providers.
Dissemination and Evaluation
Email Launch and Print Materials
In the first month following the English toolkit launch, there were 859 pageviews. Following the French toolkit launch in December 2020, the toolkit pageviews increased slightly from the previous month by 6.25%. The printed advertising materials were distributed in June 2022, and in the following month, traffic to the toolkit page increased by 23%. As of December 2023, there have been 7766 downloads of the toolkit. Trends in pageviews over time are depicted in Figure 5.
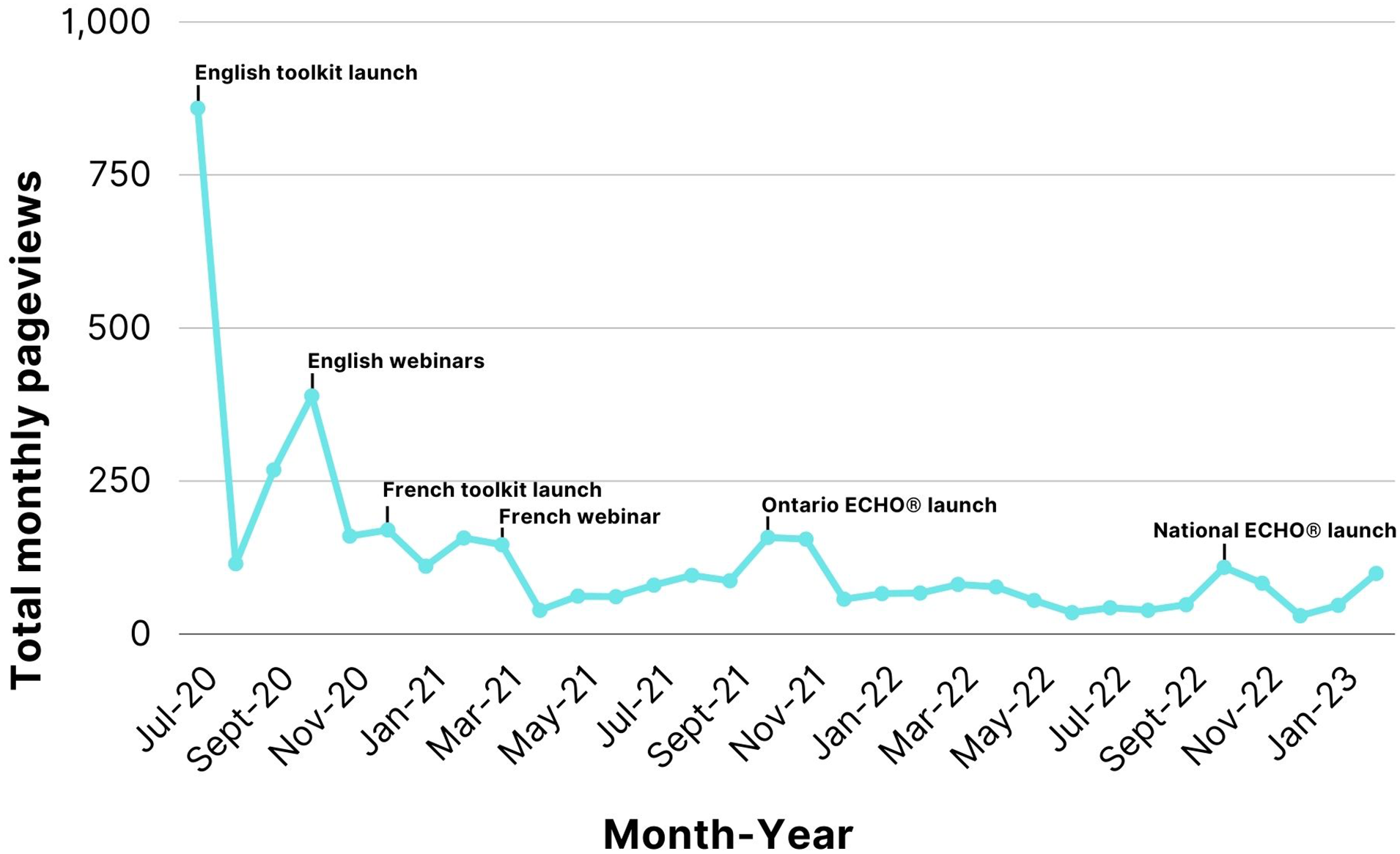
Pageviews by month and dissemination method.
National Webinars
The webinars had 315 attendees (162/101/51 for webinars 1, 2 and 3, respectively). The poll questions asked throughout the session had a good response rate (50%, 59% and 41%, respectively). The average interest rating across the 2 English webinars was 72/100 (SD 21.5) and was not calculated for the French webinar.
A total of 85 participants completed the post-webinar surveys (27% response rate) with overwhelmingly positive feedback. Across all 3 webinars, most participants agreed or strongly agreed they would use the gained knowledge (92%), the webinar increased their capacity to respond to HIV in their communities (89%), and they would recommend the webinar to others (90%). The participants also rated their knowledge of WCHC before and after the webinar on a scale from 1 to 10. On average, participant knowledge increased by 27% (6.22 to 7.92), 28% (6.11 to 7.85) and 41% (5.44 to 7.67) for the first, second and third webinars, respectively. Following the English webinars in October 2020, online traffic to the toolkit page increased by 45% (Figure 5), while no notable increase was observed following the French webinar.
Ontario Project ECHO® Virtual Training
The Ontario Project ECHO®: WCHC hub included 2 infectious disease specialists, a family physician, an HIV pharmacist, 2 HIV nurses and an internal medicine resident, along with 6 diverse women living with HIV. The pilot enrolled 35 spokes with diversity in specialty and location (Table 3). Of these, 31 spokes attended at least 1 synchronous session, with an average of 10 attendees per synchronous session (SD 5.6). Following the provincial ECHO® cycle launch, traffic to the toolkit webpage increased by 82% (Figure 5).
Demographic Characteristics of Spokes from the Ontario Project ECHO® (n = 33).
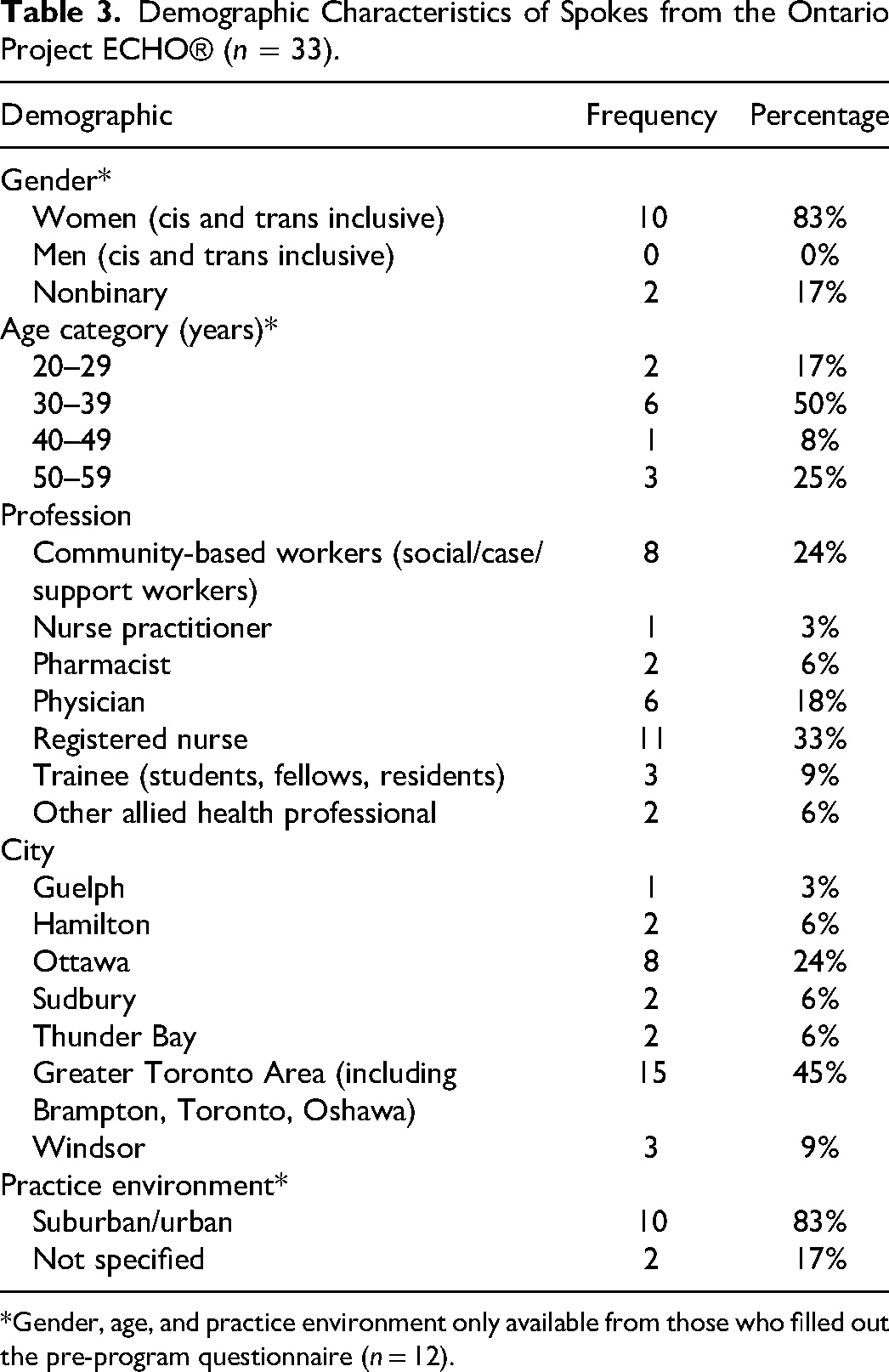
*Gender, age, and practice environment only available from those who filled out the pre-program questionnaire (n = 12).
Feedback from Post-session Surveys
Throughout the provincial cycle, 43 post-session surveys were completed by 13 unique spokes. Across all sessions, the spokes agreed or strongly agreed that the objectives in the session were clear (95%) and were met (100%). Notably, 79% noted a change in attitudes towards WCHC. The survey comments emphasised the invaluable insights gained from women with lived experience, the value of discussions with a multidisciplinary audience and the practical benefits of the shared resources. Suggestions included optimising the schedule to allow more time for case-based discussion.
Feedback from Post-program Survey
During the COVID-19 pandemic, participant attendance rates declined, impacting the post-program evaluation data and limiting the validity of the quantitative responses. Instead, qualitative data from open-ended feedback questions in the post-session surveys and the focus group provided insights into participant satisfaction and the training's impact on spoke practices.
Qualitative Feedback from Focus Group
Five hub members and 4 spoke members participated in this focus group that assessed self-efficacy, knowledge change and satisfaction and gathered general comments and suggestions about the program. Spokes indicated that the COVID-19 wave in December 2021 resulted in a reallocation of staff in their organizations, limiting their ability to participate in the ECHO® sessions. Some suggested hosting weekly sessions instead of bi- or tri-weekly to avoid the ‘out of sight out of mind’ phenomenon. An additional suggestion was to allow providers to join the program partway through the cycle and watch recorded sessions asynchronously. Overall, all participants shared positive feedback, with spokes emphasising the integration of content with the social determinants of health and a consistent person-centred focus. Spokes reported adopting specific practice changes regarding trauma- and violence-aware care, as well as peer support and capacity building, into their clinics.
National Project ECHO® Virtual Training
Based on the success of the pilot methodology, we replicated our approach on a national scale and incorporated hub members with both clinical and lived expertise from 5 provinces for a national Project ECHO®: WCHC cycle. The national hub included 3 infectious disease specialists, a family physician, an HIV pharmacist, a nurse practitioner, an internal medicine resident, a social worker and 7 women living with HIV. The changes that were implemented due to pilot feedback included allowing spokes to register at any point during the cycle, promoting recorded session viewing, running sessions every week to encourage habit-building, adding 15 min to the case-based discussion portion, and incorporating a new section at the end of every didactic presentation dedicated to priority population considerations (including trans women, Indigenous women, Black women and women who use substances).
The national cycle drew 96 registrants from 7 provinces (British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec and Newfoundland), which are home to the majority of all people living with HIV in Canada. 1 The spoke demographics were similar to those in the pilot (Table 4). Fifty-three spokes attended at least 1 synchronous session, with an average of 24 attendees per synchronous session (SD 5.2). Following the national cycle launch, traffic to the toolkit webpage more than doubled (127% increase).
Demographic Characteristics of Spokes from the National Project ECHO® (n = 96).
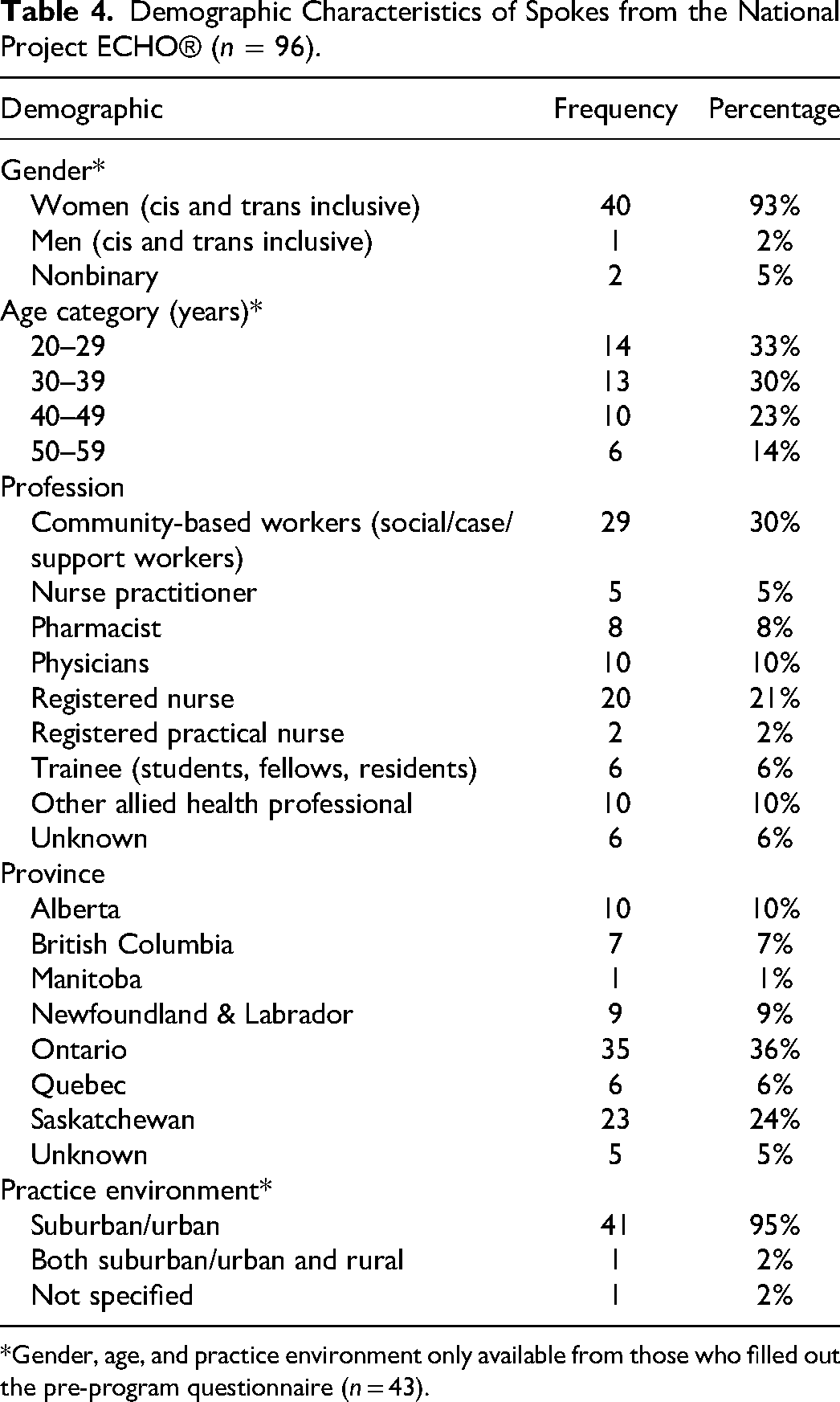
*Gender, age, and practice environment only available from those who filled out the pre-program questionnaire (n = 43).
Feedback from Post-session Surveys
Similar to the pilot, the post-session survey response rate declined as the cycle progressed. Ninety-three post-session surveys were completed by 42 unique spokes. Overall, the spokes agreed or strongly agreed that the objectives in the session were clear (95%) and met (94%), and the session changed their behaviors and attitudes towards WCHC (57%). Qualitatively, the spokes appreciated the inclusion of immediately implementable practical resources, the collaborative brainstorming and networking facilitated by the case-based format, and the option to view the recorded sessions asynchronously. The dedicated reflection on priority population considerations also received positive feedback. Specific quotes from spokes included: ‘I wish this was part of every health professional program as a regular standard of care’. ‘ECHO sessions seem to be the best HIV related online sessions [I] have attended’.
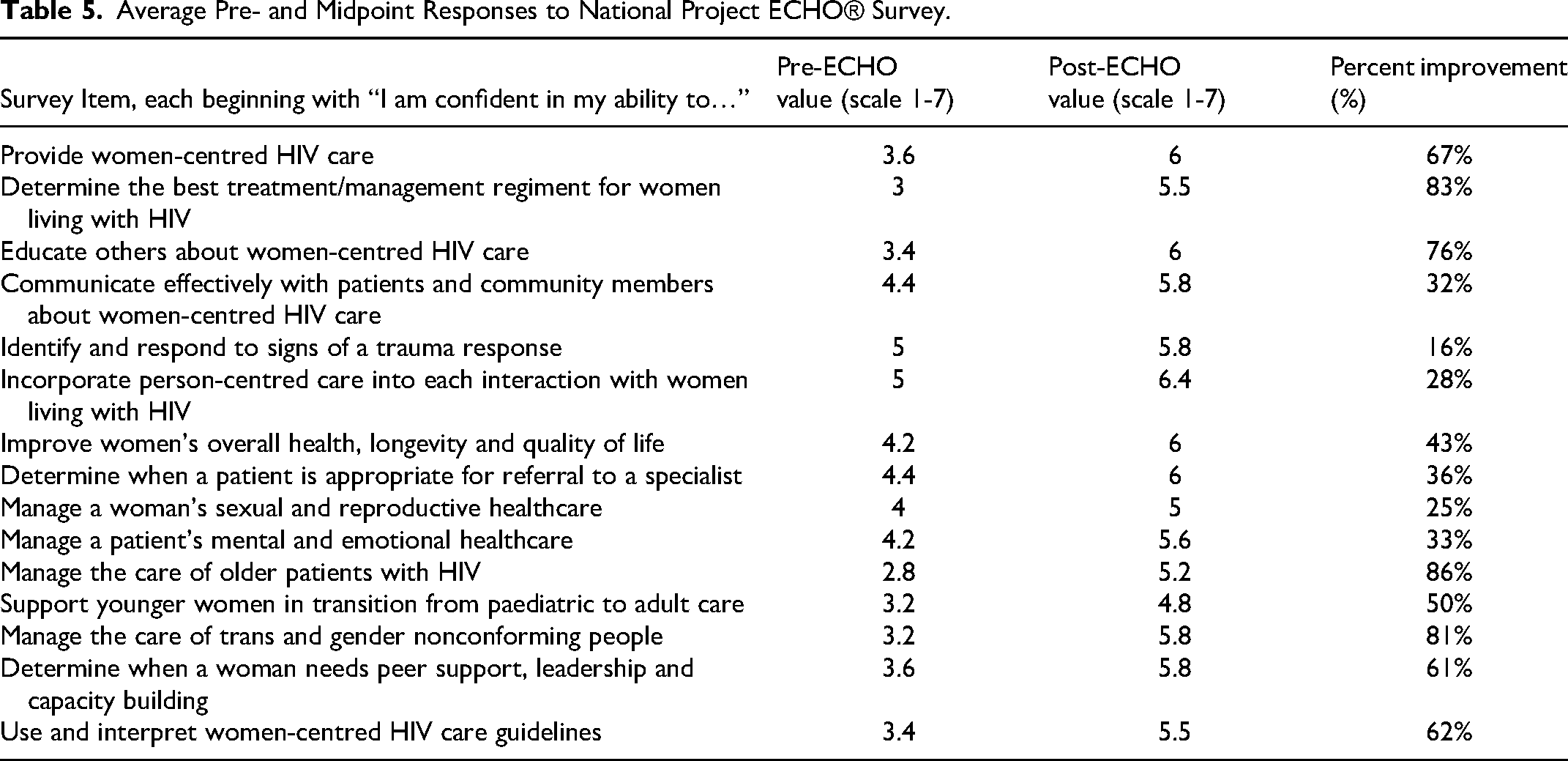
Feedback from Midpoint Surveys
Five spokes completed both the pre- and midpoint evaluations. On average, all 15 aspects of self-reported confidence increased over time, with the most significant being confidence in the ability to manage the care of older patients with HIV (86% increase), determine the best treatment regimen for women living with HIV (83% increase), educate others about WCHC (76% increase) and provide WCHC (67% increase). See Table 5 for full results
Average Pre- and Midpoint Responses to National Project ECHO® Survey.
Discussion
Toolkits were selected as the primary dissemination method for the WCHC Model due to their popularity in expanding healthcare models and promoting evidence-based practice for both providers and patients.37–42 Recently, a systematic review of 39 studies affirmed toolkits as a promising knowledge translation method for facilitating evidence use in practice and improving health outcomes. 43
The WCHC toolkits served as an effective method to condense extensive information and resources related to the model, standing out as the best choice for a practical and comprehensive resource with real-world examples on model implementation. 43 Strengths of thetoolkits include the iterative, community-based development process and the creation of separate toolkits for service providers and women. Their creation for use by a diverse, national audience increased usability and relevance. By translating the women's toolkit into French, we increased our reach to French speaking women who have previously been identified as having limited access to HIV services.44,45 Sharing the toolkits through virtual channels, such as webinars and Zoom, proved to be exceptionally effective, offering a level of convenience and accessibility that resonated with attendees. This approach enabled us to connect with audiences throughout Canada and extended our reach beyond our traditional networks.
For effective research uptake potentially leading to behavior and practice change, selecting dissemination strategies that are evidence-based and contextually relevant is essential. Existing literature on sharing models of care suggests that there is a need to set realistic goals reflective of staff capacity for change and enthusiasm of buy-in. 46 We planned for this need by involving community members and service providers from the very beginning stages of toolkit development and dissemination and continued with consultations at all points of the process. Given the toolkit's focus on equitable access to women-centred HIV care, CEP's expertise in evidence-based knowledge translation and our team's expertise in community-based research principles made an ideal partnership to achieve this buy-in. The development process involving usability testing was monumental in the successful uptake of the toolkit. Service providers appreciated the opportunity to share feedback on a tool that would have practical applicability in their specialities. This encouraged them to spread the word about the toolkit launch and dissemination methods including handing out flyers in their clinics, sharing the webinar registration link with their networks, and encouraging colleagues to join Project ECHO®. Most importantly, evaluations from usability testing demonstrated that women living with HIV felt heard and valued as experts. Many of those who completed the usability testing had been CHIWOS participants, and thus they were able to see that the wisdom and experiences they shared through CHIWOS were being used to improve women's health and wellbeing. They were excited by the potential of the toolkit and invested in the process, demonstrated by their eagerness to get a copy of the toolkit and share with their networks.
Previous knowledge translation research has shown that utilizing multiple dissemination methods maximizes reach with end users. 47 We chose to distribute bilingual, visually appealing print materials (posters, flyers and postcards) to advertise the toolkits as previous research has indicated printed educational materials likely improve healthcare professional's practice, especially as part of a multifaceted intervention. 48 This method was also chosen for its cost-effectiveness, familiarity and convenience with hopes that it would reach populations of women who mainly access HIV resources from their HIV providers or clinics as opposed to online. Understanding that tailored print materials have been proven more effective at engaging patients, we adapted the materials to the specific groups and used first-person language.49,50 Our dissemination strategy also included virtual methods (webinars, Project ECHO® and housing the toolkit online). This was partially influenced by the COVID-19 pandemic, but also our desire to reach a large national audience. We considered existing literature that suggests shared vision and recognised the need for a new care approach that increases care model acceptance when designing the 3 webinars. 46 Purposely hosting separate webinars for distinct end-user groups and in both national languages allowed us to tailor the webinar content as much as possible to those with a shared vision. Partnering with CATIE, a national leader in the HIV space, also increased our reach. Obtaining accreditation of the Project ECHO® program and being able to offer CME credits to physicians was also a strength. The format of the Project ECHO® model was ideal for the WCHC Model and toolkits as the 6 aspects of the model were easily broken into 1 to 2 didactic sessions each, and the case-based portion provided a way for service providers to gather advice from the hub and spokes on implementing WCHC in practice. Additionally, the asynchronous option used in the national Project ECHO® cycle provided a solution to staff capacity limitations to attend sessions synchronously. Using Project ECHO® as a dissemination strategy allowed for comprehensive evaluations to quantitatively measure practice change and uptake over time that would not be possible with printed materials and webinars alone. Interestingly, the practice environments of the majority of ECHO® participants were suburban or urban. This provides some evidence that Project ECHO®, which has traditionally targeted rural providers, is also beneficial to those practicing in more well-resourced areas, and it suggests that Project ECHO® is a useful option for all providers considering the current virtual care landscape.
There are some notable limitations of the toolkit and the dissemination strategies used. The majority of dissemination efforts took place during the COVID-19 pandemic, which impacted the ability of service providers to participate in educational activities, as noted in the Project ECHO® focus groups. The toolkits were designed in PDF format as a fixed resource, which created the risk that the content could become out of date. To mitigate this, we included links to webpages that are continually being updated. The toolkit PDFs were designed to be accessed via computer, which limits accessibility by women without access to technology. As a solution, some team members printed copies and made them available to women in British Columbia at the Oak Tree Clinic. The toolkits are long and content-heavy, which was necessary given the breadth of information to include, but this may have discouraged women from using them. Due to budgetary constraints, we were unable to translate the service provider toolkit into French; however, we do not anticipate that this was a large barrier to access for providers. The distribution of printed advertising materials was limited to Ontario and British Columbia due to associated printing and shipping costs that may have limited our reach to other provinces. The translation of the women's toolkit into only French and English may have limited access to other women living with HIV, particularly recent immigrants, who may not speak either language. Both the webinars and Project ECHO® were only accessible virtually, which may have created a barrier for those without internet access. These methods proved difficult to measure impact on practice: the webinar due to the single time point and the Project ECHO® due to the challenges incentivising spokes to complete pre- and post-evaluations. The lack of a control group for the ECHO® project limits our understanding of the effectiveness of the program, as there could be self-selection bias where persons who are more interested and open to learning signed up. Sampling bias may also have impacted the pre- and post-program data. The results should be considered in light of these limitations.
Conclusions
Our evidence-based WCHC toolkits, developed through collaborative knowledge translation, provide user-friendly integrated clinical guidance to comprehensively address the unique needs and priorities of women living with HIV. Launching the toolkits at an opportune time, hosting instructional webinars and developing a thorough virtual training to support the utilization of the toolkits were essential in their dissemination. Our study represents one of the first of its kind to examine the effectiveness of several dissemination strategies in the field of women and HIV. The findings from this study highlight the importance of engaging stakeholders early in the tool development process and using multiple dissemination methods to meet the needs of diverse end users. Our findings indicate that it is feasible to create a tool with specific practical application in the healthcare setting and that a multimodal dissemination strategy with both passive and active methods is an effective way to reach and train a diverse group of end users to achieve practical change.
Footnotes
Acknowledgements
The Core Research Team would like to especially thank all of the women with HIV who participated in the research that informed this study and entrusted us with their experiences of HIV treatment, care and support. The authors thank the knowledge translation experts at the Centre for Effective Practice (https://cep.health/) for their work on the WCHC toolkits. They extend a special thank you to The Public Studio (www.thepublicstudio.ca) for their help with the graphic design for the printed advertising materials.
The authors thank all of their webinar partners: the Canadian AIDS Treatment Information Exchange (CATIE), Women and HIV Research Program at Women's College Hospital, Women and HIV/AIDS Initiative, BC Women's Hospital Health Centre, Women's Health in Women's Hands, Simon Fraser University, BC Centre for Excellence in HIV/AIDS, ViVA Women, AIDS Vancouver, CATIE, the Coalition des organismes communautaires québécois de lutte contre le sida (COCQ-SIDA), AIDS Committee of Ottawa (ACO), Africans in Partnership Against AIDS (APAA).
The authors thank the Ontario HIV Treatment Network for their in-kind technical support for our Ontario Project ECHO® cycle, specifically Diana Campbell and Tanya Oskam. They thank the CAMH Project ECHO® Superhub for their in-kind support and oversight.
The authors wish to make a special acknowledgement to French webinar moderator and speaker, Alexandra de Kiewit who passed away October 2022. Alexandra was a fierce advocate and woman living with HIV. She believed in the WCHC model and in supporting women living with HIV and individuals who use drugs to receive the care and services they deserve. She contributed to this work with dedication and passion.
The CHWIOS Research Team includes:
British Columbia: Aranka Anema (University of British Columbia, Vancouver), Denise Becker (Positive Living Society of British Columbia, Vancouver), Lori Brotto (University of British Columbia, Vancouver), Allison Carter (British Columbia Centre for Excellence in HIV/AIDS, Vancouver and Simon Fraser University, Burnaby), Claudette Cardinal (Simon Fraser University, Burnaby), Guillaume Colley (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Erin Ding (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Janice Duddy (Pacific AIDS Network, Vancouver), Nada Gataric (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Robert S. Hogg (British Columbia Centre for Excellence in HIV/AIDS, Vancouver and Simon Fraser University, Burnaby), Terry Howard (Positive Living Society of British Columbia, Vancouver), Shahab Jabbari (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Evin Jones (Pacific AIDS Network, Vancouver), Mary Kestler (Oak Tree Clinic, BC Women's Hospital and Health Centre, Vancouver), Andrea Langlois (Pacific AIDS Network, Vancouver), Viviane Lima (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Elisa Lloyd-Smith (Providence Health Care Elisa Lloyd-Smith), Melissa Medjuck (Positive Women's Network, Vancouver), Cari Miller (Simon Fraser University, Burnaby), Deborah Money (Women's Health Research Institute, Vancouver), Valerie Nicholson (Simon Fraser University, Burnaby), Gina Ogilvie (British Columbia Centre for Disease Control, Vancouver), Sophie Patterson (Simon Fraser University, Burnaby), Neora Pick (Oak Tree Clinic, BC Women's Hospital and Health Centre, Vancouver), Eric Roth (University of Victoria, Victoria), Kate Salters (Simon Fraser University, Burnaby), Margarite Sanchez (ViVA, Positive Living Society of British Columbia, Vancouver), Jacquie Sas (CIHR Canadian HIV Trials Network, Vancouver), Paul Sereda (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Marcie Summers (Positive Women's Network, Vancouver), Christina Tom (Simon Fraser University, Burnaby), Clara Wang (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Kath Webster (Simon Fraser University, Burnaby), Wendy Zhang (British Columbia Centre for Excellence in HIV/AIDS, Vancouver).
Ontario: Rahma Abdul-Noor (Women's College Research Institute, Toronto), Jonathan Angel (Ottawa Hospital Research Institute, Ottawa), Fatimatou Barry (Women's College Research Institute, Toronto), Greta Bauer (University of Western Ontario, London), Kerrigan Beaver (Women's College Research Institute, Toronto), Anita Benoit (Women's College Research Institute, Toronto), Breklyn Bertozzi (Women's College Research Institute, Toronto), Sheila Borton (Women's College Research Institute, Toronto), Tammy Bourque (Women's College Research Institute, Toronto), Jason Brophy (Children's Hospital of Eastern Ontario, Ottawa), Ann Burchell (University of Toronto, Toronto), Allison Carlson (Women's College Research Institute, Toronto), Lynne Cioppa (Women's College Research Institute, Toronto), Jeffrey Cohen (Windsor Regional Hospital, Windsor), Tracey Conway (Women's College Research Institute, Toronto), Curtis Cooper (Ottawa Hospital Research Institute, Ottawa), Jasmine Cotnam (Women's College Research Institute, Toronto), Janette Cousineau (Women's College Research Institute, Toronto), Marisol Desbiens (Women's College Research Institute, Toronto), Annette Fraleigh (Women's College Research Institute, Toronto), Brenda Gagnier (Women's College Research Institute, Toronto), Claudine Gasingirwa (Women's College Research Institute, Toronto), Saara Greene (McMaster University, Hamilton), Trevor Hart (Ryerson University, Toronto), Shazia Islam (Women's College Research Institute, Toronto), Charu Kaushic (McMaster University, Hamilton), Logan Kennedy (Women's College Research Institute, Toronto), Desiree Kerr (Women's College Research Institute, Toronto), Gladys Kwaramba (Women's College Research Institute, Toronto), Lynne Leonard (University of Ottawa, Ottawa), Johanna Lewis (Women's College Research Institute, Toronto), Carmen Logie (University of Toronto, Toronto), Shari Margolese (Women's College Research Institute, Toronto), Marvelous Muchenje (Women's Health in Women's Hands, Toronto), Mary (Muthoni) Ndung’u (Women's College Research Institute, Toronto), Kelly O’Brien (University of Toronto, Toronto), Charlene Ouellette (Women's College Research Institute, Toronto), Je Powis (Toronto East General Hospital, Toronto), Corinna Quan (Windsor Regional Hospital, Windsor), Janet Raboud (Ontario HIV Treatment Network, Toronto), Anita Rachlis (Sunnybrook Health Sciences Centre, Toronto), Edward Ralph (St. Joseph's Health Care, London), Sean Rourke (Ontario HIV Treatment Network, Toronto), Sergio Rueda (Ontario HIV Treatment Network, Toronto), Roger Sandre (Haven Clinic, Sudbury), Fiona Smaill (McMaster University, Hamilton), Stephanie Smith (Women's College Research Institute, Toronto), Tsitsi Tigere (Women's College Research Institute, Toronto), Wangari Tharao (Women's Health in Women's Hands, Toronto), Sharon Walmsley (Toronto General Hospital Research Institute, Toronto), Wendy Wobeser (Queen's University, Kingston), Jessica Yee (Native Youth Sexual Health Network, Toronto), Mark Yudin (St. Michael's Hospital, Toronto).
Quebec: Dada Mamvula Bakombo (McGill University Health Centre, Montréal), Jean-Guy Baril (Université de Montréal, Montréal), Marc Boucher (Centre Hospitalier Universitaire Ste-Justine, Montréal), Isabelle Boucoiran (Centre Hospitalier Universitaire Sainte-Justine, Montréal), Nora Butler Burke (Concordia University, Montréal), José Côté (Centre Hospitalier de l’Université de Montréal, Montréal), Janice Dayle (McGill University Health Centre, Montréal), Danièle Dubuc, (McGill University Health Centre, Montréal), Mylène Fernet (Université du Québec à Montréal, Montréal), Marilou Gagnon (University of Ottawa, Ottawa), Fatima Kakkar (Centre Hospitalier Universitaire Sainte-Justine, Montréal), Maxime Kiboyogo (McGill University Health Centre, Montréal), Marina Klein (McGill University Health Centre, Montréal), Gary Lacasse (Canadian AIDS Society, Ottawa), Valérie Lamarre (Centre Hospitalier Universitaire Ste-Justine, Montréal), Carrie Martin (Native Women's Shelter of Montreal, Montréal), Lyne Massie, (Université de Québec à Montréal, Montréal), Brigitte Ménard, (McGill University Health Centre, Montréal), Ken Monteith (COCQ-SIDA, Montréal), Nadia O’Brien (McGill University, Montréal), Joanne Otis (Université du Québec à Montréal, Montréal), Doris Peltier (Communities, Alliances and Networks, Montréal), Alie Pierre (McGill University Health Centre, Montréal), Karène Proulx-Boucher (McGill University Health Centre, Montréal), Danielle Rouleau (Centre Hospitalier de l’Université de Montréal, Montréal), Geneviève Rouleau (Centre Hospitalier de l’Université de Montréal, Montréal), Édénia Savoie (McGill University Health Centre, Montréal), Cécile Tremblay (Centre Hospitalier de l’Université de Montréal, Montréal), Benoit Trottier (Clinique Médicale Urbaine du Quartier Latin, Montréal), Jason Szabo (Clinique l’Actuel, Montréal), Sylvie Trottier (Centre Hospitalier Universitaire de Québec, Quebec City), Christos Tsoukas (McGill University Health Centre, Montréal).
Other Canadian provinces or international jurisdictions:
Jacqueline Gahagan (Dalhousie University, Halifax), Catherine Hankins (University of Amsterdam, Amsterdam), Renee Masching (Communities, Alliances and Networks, Dartmouth), Susanna Ogunnaike-Cooke (Public Health Agency of Canada, Ottawa). All other CHIWOS Research Team members wish to remain anonymous.
Availability of Data and Materials
The datasets generated and/or analysed during the current study are not publicly available due to the potential epistemological, methodological, legal and ethical issues that arise when qualitative data from transcripts are shared or reused but are available from the corresponding author on reasonable request, and by following local research ethics procedures.
Authors’ Contributions
JK led the writing of the manuscript. VLK, M Kazemi and M Loutfy contributed significantly. AU, CL, MY, JR, AK and M Narasimhan provided feedback and edits on the manuscript. All other authors read and approved the final manuscript. VLK, LB, WT, CL, AU, NP, MY, JR, SI, VN, MH, AP, AK, M Kazemi, M Ndung’u and M Loutfy were involved in the toolkit development process, including appraising clinical guidelines, developing content and hosting focus groups and usability testing. VLK, AU, NP, KW, M Lee, VN, BG, AP, AK, M Kazemi, M Kesler, M Ndung’u and M Loutfy led the webinar series. JK, VLK, PM, NP, EK, JR, KW, VN, BG, MH, M Ndung’u and M Loutfy were involved in Project ECHO®.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Women and HIV Research Program (WHRP) at Women's College Hospital received a Canadian Institute for Health Research Foundation Grant to fulfil the objective of finalizing and preparing to pilot the WCHC model in Canada. This work was supported by the Canadian Institutes of Health Research (CIHR) (http://www.cihr-irsc.gc.ca/e/193.html) (grant number FDN154325). CATIE provided funding for the webinar series. AdP received support from Fonds de Recherche du Quebec – Sante (http://www.frqs.gouv.qc.ca/en/le-frqs). AC received support from a CIHR Doctoral Award. PM received support from a CTN Postdoctoral Fellowship. AK received salary support through a Tier 2 Canada Research Chair in Global Perspectives on HIV and Sexual and Reproductive Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.