
Abstract
This qualitative longitudinal study examined the experiences of people living with HIV who engaged in a structured community-based exercise (CBE) program under the supervision of a fitness coach. Twenty people living with HIV were invited to participate in 3 semi-structured interviews over time. Participants engaged in exercise 3 times per week for 6 months with one weekly session supervised by a coach. Interviews were audio-recorded, transcribed verbatim and underwent longitudinal thematic analyses. Eleven participants were included representing a total of 30 interviews. Participants valued their experiences with the CBE program, particularly the motivation provided by the coach. Concerns about the environment, stigma and episodic health challenges affected their overall experience. To foster independence and promote self-management, health providers should consider these findings when encouraging CBE with people living with HIV. It is important to understand their goals and offer a variety of exercise options to meet their needs.
What Do We Already Know about This Topic?
In spite of the documented benefits, engagement in physical activity and exercise is difficult for people living with HIV due to unique physical, mental health and psychosocial challenges.
How Does Your Research Contribute to the Field?
While people living with HIV who engaged in community based exercise were able to increase their confidence over time, concerns about the environment, stigma and episodic health challenges affected their overall experience.
What Are Your Research’s Implications Toward Theory, Practice or Policy?
To foster independence and promote self-management, health providers should consider several factors when encouraging community-based exercise with people living with HIV.
Introduction
The life expectancy of people living with HIV, who have access and are adherent to anti-retroviral therapy, is approaching that of individuals without HIV. 1 Consequently, HIV has been transformed into a chronic illness in which many may experience disability related to the side effects of medication, effects of the virus and natural consequences of aging. 2,3 Rehabilitation can play an important role in helping people living with HIV manage their disability and increase their quality of life. 4 As with many chronic illnesses, self-management strategies can be important to the overall management of HIV- related disability. 5
Exercise is a self-management intervention that can address disability among people living with HIV. 6 In people living with HIV, formal exercise and physical activity have been associated with enhancements to physiologic and metabolic outcomes, 7 -10 cognitive health, 11 social support, and quality of life. 12 Regular exercise is safe and can lead to improvements in cardiopulmonary fitness, strength, body composition, and mental health in people living with HIV. 13 -15
In spite of the documented benefits, engagement in physical activity and exercise is challenging for people living with HIV. A recent systematic review reported people living with HIV were less active than others with chronic illness and recommended that physical activity counselling be a key component of their rehabilitation. 16 They are also less likely to meet recommended weekly activity levels than others with chronic illness. 17
Community based exercise (CBE) is a promising approach to improve the health of people living with HIV within a self-management framework. CBE involves a group of individuals exercising with the assistance of an instructor with the goal of promoting regular exercise in the community. 18 -20 CBE can foster social interaction, provide support and encouragement to exercise, and can promote emotional, cognitive and behavioural self-management strategies to help independently manage chronic health challenges. 21,22
People living with HIV have unique health challenges or disability, defined as physical, cognitive, mental and emotional symptoms and impairments, difficulties with day-to-day activities, challenges to social inclusion, and uncertainty or worrying about future health. 23 Disability experiences can impact the ability of people living with HIV to engage in CBE, including those related to physical health (e.g., fatigue), 24 mental health (e.g., depression), 25 and psychosocial (e.g., stigma, poverty) 26 well-being. Additionally, disability associated with HIV is recognized as having a temporal component as it may be episodic in nature. 23,27 The fluctuations over time and associated uncertainty that result from episodic disability may complicate both engagement in and measurement of effectiveness of CBE interventions. Understanding how episodic disability affects the CBE experiences of people living with HIV will be incomplete using only cross-sectional research designs. Quantitative study designs do not provide an in-depth understanding of the lived experiences of people living with HIV engaging in CBE. Qualitative longitudinal study designs can complement quantitative designs and provide nuanced insights for developing treatment strategies to decrease disability. 28 This methodology can promote increased understanding of health challenges and strategies that individuals use to make sense of the past and plan for the future. 29
The overall purpose of the study was to examine the experiences of adults living with HIV who participated in a structured 6-month exercise intervention in a community setting over time.
Methods
We used qualitative longitudinal methods to examine the experiences of adults living with HIV who engaged in a CBE intervention. The primary aim of qualitative longitudinal research is to understand changes that occur over time and the processes associated with these changes. 30,31 It seeks to explore how and why change occurs. 31
This study was part of a larger 3-phase community-based exercise study which examined changes in fitness among 108 adults living with HIV. 22 Adults living with HIV who considered themselves safe and medically able to engage in exercise were recruited from community-based organizations in Toronto, Canada.
Participants engaged in aerobic, resistance, flexibility and balance exercises. Phase 1 was a baseline monitoring phase (8 months). Phase 2 was the exercise intervention phase in which participants were provided with a Young Men’s Christian Association (YMCA) membership and expected to exercise 3 times per week for 90 minutes each (6 months). A key feature was the supervision by a certified personal coach for 60 minutes for one of the sessions each week. The qualitative study occurred primarily in Phase 2. During this phase, participants also were invited to attend monthly in-person self-management education sessions related to HIV and health. Self-management educational sessions took place each month of the intervention phase (6 sessions in total), focused on topics related to self-management and healthy lifestyle living with HIV. Participants had the option to attend 6 of 7 possible sessions, of which topics included: HIV and exercise, nutrition and healthy weight, mindfulness and stress reduction, sleep health and hygiene, HIV and neurocognitive health, complementary and alternative therapies in HIV, and role for rehabilitation in the context of HIV. In Phase 3, participants were expected to continue with exercise independently 3 times per week at the YMCA (6 months). Participants underwent physical fitness and questionnaire assessments at 2-month intervals as part of the study evaluation.
We invited 20 participants from the larger study to participate in a series of 3 semi-structured interviews. We used purposive sampling in which we sought variation in gender, age, ethno-cultural background, time since HIV diagnosis and experience with exercise. There is little literature to guide sample size calculations in qualitative longitudinal research. For single interview studies, a sample size between 20 and 30 is considered a conservative guideline. 32 Qualitative longitudinal research elicits a large amount of data, thus we recruited 15 adults living with HIV (potentially 45 interviews). As some participants withdrew after the first interview, we recruited 5 additional participants. Qualitative interviews occurred just prior to the start of the exercise intervention (Time 1), mid-way (Time 2) and at the end of the intervention (Time 3). As we were interested in the experiences of those who completed the intervention, we included only those who participated in at least 2 interviews including the final interview.
Three experienced interviewers were involved in data collection over the course of the study. In the initial interview, interviewers explored past experience with exercise, limitations to functional activities and their motivation and goals for participating. Participants were asked to reflect on their expectations, anticipated benefits and concerns with the upcoming CBE intervention. In the subsequent interviews (Time 2 and 3), we explored experiences with the CBE intervention. Interviewers shared the participant’s responses allowing them to reflect and build upon past interviews, a form of transactional validity in which member checking is part of the data collection process. 33 We further explored issues that were identified at Time 1, probing the participants to consider if any and what changes had occurred. Emergent themes were documented and discussed with participants at Time 2 and/or Time 3. Interviews were audio recorded and transcribed verbatim.
Analyses
Longitudinal qualitative analyses are complex, requiring summaries of data both cross-sectionally and longitudinally. A previously documented analytic process guided our qualitative analyses. 28 We developed in-depth summary profiles for each participant at their initial interview from the verbatim transcript. Cross-sectional summary profiles were then developed for subsequent interviews, documenting perceived changes in health and disability and emergent issues that had occurred over time on a summary form. Next, using the forms, we developed an in-depth summary profile of each participant’s experiences with the CBE intervention over time. In the final step, we compared the longitudinal summary profiles of each participant to document similarities and differences in the experiences over time. This comparison resulted in the identification of preliminary themes reflecting the participants’ experiences over time. Final themes resulted from team consensus following discussion and modification of the preliminary themes. All interview summary sheets were developed by the first author, and then independently reviewed, verified and supplemented by at least one other co-author.
Ethical Approval and Informed Consent
Ethics approval was received by University of Toronto (HIV Ethics Board; Approval #32910). All participants provided written informed consent prior to enrolment in the study.
Results
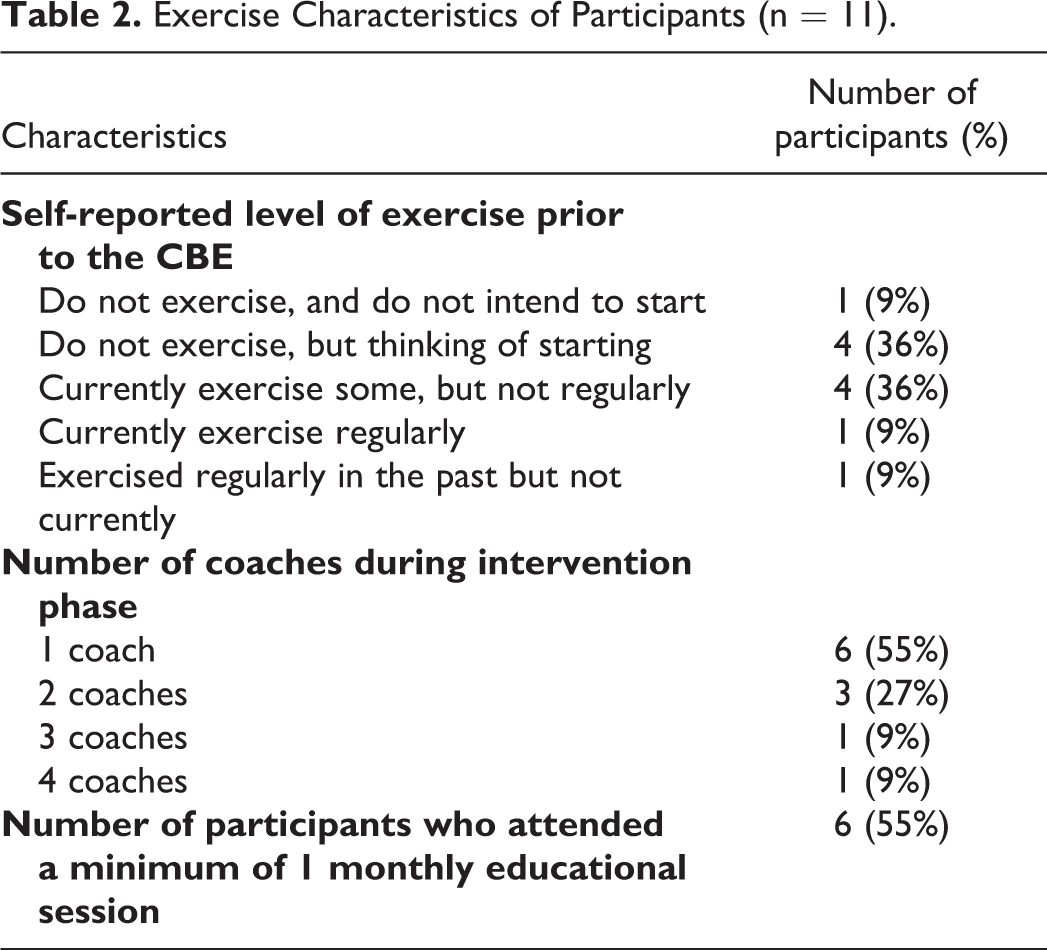
Thirty interviews from 11 participants were included in the analyses; 8 participants completed 3 interviews and 3 participants completed 2 interviews. The majority identified their gender as man (n = 7; 64%) with a median age of 52 years (interquartile range (IQR) 37, 61) and median 11 years since HIV diagnosis (IQR 22, 5). Additional demographic and exercise characteristics of participants are outlined in Tables 1 and 2.
Demographic Characteristics of Participants (n = 11).

Exercise Characteristics of Participants (n = 11).
The emergent themes reflected the experiences of the participants over time including development of increased confidence. They experienced worrying about their body image and exercising in a gym environment, which changed over time as some became more confident and comfortable. These experiences were affected by their complex lives with episodic illness challenging their ability to engage in CBE. They encountered motivating factors including meeting their goals as they progressed. Participants also described valuing the relationship that developed with their coaches over time. Each of the themes are described in detail below with representative quotes.
Increasing Confidence
Participants spoke of experiencing increased confidence in a number of areas and feeling better about themselves over time. Several who had never exercised in the past were nervous about starting the intervention and about their ability to complete an exercise program at Time 1. Others initially worried about being able to exercise regularly when having an exacerbation of symptoms and developed the ability to modify their program when having a “bad day”. By the end of the program most expressed confidence in their ability to exercise safely, remember their exercise program, and knowledge of how to progress their exercises. But when I go in this study I get the proper instruction or is it I’m doing right or wrong. (My coach) knows better. Like what is my goal, he can give some guidance. According to that I can go from that. So that next year without his help I can do my own. (P29, man, 40 years old, >5 years since HIV diagnosis) Now I really learn a lot from this because when I started I was emotionally and mentally not good at all because I didn’t accept (my diagnosis). But since I started the exercise my mind is better and I’m sleeping much better because before I was thinking too much what will happen, what will happen, when something is going to strike me, when I’m going to die. But now I’m seeing there’s light to it. So one day at a time and my life is not ending (P61, woman 55 years old, >5 years since HIV diagnosis) It boosts my own self confidence and my self esteem and my personal image of myself. That energy shift inside translates outwardly and people see that and people respond to that. (P56, woman, 39 years old, >5 years since HIV diagnosis)
Worrying About Body Image and the Gym Environment
Many participants experienced worries about how they would integrate into the YMCA environment initially. Most were not interested in attending group exercise classes. They did not see themselves as people who engaged in “hard core workouts” or as competent exercisers and perceived that others in the gym would be observing them. Others worried that they were “too skinny” or “too old” or about others in the environment observing the effects of lipodystrophy. One 70-year-old man spoke of how uncomfortable he felt exercising among young men who were in “great shape”. Over time, some grew more comfortable exercising in an open gym environment, stating they didn’t feel as “out of place.” It’s one of those stigma things and you not lifting all the heavy weights, you not doing all the stuff that’s around you and all that moaning and groaning. I always feel that people are looking at you if you’re just doing very light things (P89, man, 62 years old, >5 years since HIV diagnosis) I just find (the small gym) not as threatening or intimidating by a bunch of younger men and in better great shape. There are some young men in great shape there but I avoid them more by being in the plus membership. (P108, man, 70 years old, >5 years since HIV diagnosis) I will see (if I will interact with others in the program). I don’t know. I’m not trusting that much because I lost so much trust in people. (P26, woman, 48 years old, >5 years since HIV diagnosis)
Living Complex Lives With Episodic Challenges
Many participants described complex lives which challenged their ability to adhere to the exercise program. They experienced episodic health challenges and co-morbidities (e.g., diabetes, fibromyalgia, chronic pain) that meant there was a need for the coach to be flexible about attendance. Some recognized they had “good and bad days” and worried about motivating themselves to attend. One woman spoke of how interruptions due to episodes of ill health led to a feeling of forever “restarting” her program. This man spoke of his struggles of managing multiple episodic co-morbidities: …it is a lot of struggle to maintain day to day routines and all. If one problem, it’s still manageable. But two or three problems…it’s too many problems. (P29, man 40 years old, >5 years since HIV diagnosis)
Contextual factors compounding participants’ physical and mental health challenges added further complexity to their lives. Managing their complex lives often meant that exercise was not a top priority. Some participants described living precarious lives with financial insecurity and relying on disability pensions, and were often socially isolated. As one man stated, “HIV is our first thing but we have all this other crap that goes with it.” (P89, man, 62 years old, >5 years since HIV diagnosis).
Experiencing Motivation and Setting Goals
Participants experienced motivators which enabled them to engage and continue in the CBE intervention. The intervention served as a catalyst for those who had exercised in the past but needed an incentive to get started again, or as one participant described it, “a push.” As many were living on limited income such as disability pensions, the free membership to the YMCA offered through the study also provided the initial motivation. Geographical proximity to home and easy access by public transport made attendance easier. A routine structure was important; knowing that there was a schedule to adhere to allowed participants to plan their weeks as noted by this woman: But this time I know that I am scheduled in something I have to do. I know someone is waiting for me. I know that someone made time for me. I have to go. (P26, woman aged 48, >5 years since HIV diagnosis) I definitely notice that I can do more without getting winded, out of breath. So I have better stamina. I think it really helped for going on the two trips that I did because you know I didn’t have any problems walking. (P108, man, 70 years old, >5 years since HIV diagnosis) Exercising is my coping strategy for my depression. So when I feel down and I go (to the gym) I get distracted. I see people. I do something I enjoy. (P26, woman, 48 years old, >5 years since HIV diagnosis)
Valuing the Coach Relationship
Most participants spoke highly of their relationship with their coaches and expressed sadness about “losing them” following the 6-month intervention. Participants expressed that the coaches helped them to learn and progress exercises in ways not possible in a group situation. Over time, the coaches supported the participants in many ways by providing motivation and encouragement, adapting exercises, providing feedback, and ensuring that participants “didn’t cheat” as reflected by this participant: Every time I meet the coach it’s a new week. I always feel energized and ready to go, great interaction with her. I know she sees me, hears me, accommodates on my program because she’s trying to get the optimum that I can do for this (P79; man, 64 years, >5 years since HIV diagnosis) It was her [the coach’s] involvement with me that I felt I was her only person and I know I wasn’t but that’s how I felt when I was dealing with her, which is great (P89, man, 62 years old, >5 years since HIV diagnosis).
Discussion
Our findings suggest that participants living with HIV valued their experiences with a 6-month CBE intervention over time, particularly the motivation and weekly support provided by the coach. While they were able to increase their confidence over time, concerns about the environment, stigma and episodic health challenges affected their overall experience.
In a cross-sectional focus group study, Neff et al also identified personal (e.g., lack of motivation and confidence), environmental (e.g., comfort in gym) and physical (e.g., pain) factors to initiating and maintaining exercise in older men living with HIV. 34 However, our longitudinal design revealed unique challenges related to the episodic nature of HIV and provided insights into the changes in confidence over time. Participants also identified factors which encouraged them to continue with the program, such as location of the gym and tailoring the program to individual needs that were similar to those found in other chronic illnesses. 35,36 Following participants over time revealed the motivation provided by meeting their goals and through the relationship they developed with their coaches.
There were concerns related to body image and exercising in an open gym environment. Some long-term survivors may have concerns related to lipodystrophy while others may be concerned with their overall body appearance in a setting where many individuals engage in weightlifting activities. 34 These environmental concerns underline the importance of identifying who is best suited to exercising in an open gym environment. For some, especially those in which distance to the gym presented motivational challenges, home-based exercise may be an option. Recent advances in telehealth delivery promoted by the COVID 19 pandemic may extend the possibilities of remote coaching. 37,38 As coaching contributed to motivation and was perceived positively by the participants, it will be important to assess the effectiveness of at-home coaching delivered online.
People living with HIV can also have challenges related to stigma, with many long-term survivors still experiencing residual trauma from the early days of the HIV epidemic. 39 Although societal attitudes have changed since the early years of the epidemic, stigma remains and can add stress, particularly to those recently diagnosed, as was evident with our participants. The fear of experiencing stigma and accidental disclosure did not change over time in several of the participants suggesting that some may be more comfortable in an exercise environment which is solely targeted to those living with HIV.
Social support has long been considered an active ingredient in chronic disease self-management programs and has been rated as the most helpful self-management strategy in people living with HIV. 40 Following the participants over time allowed for insight into the value of the relationship with the coach for motivation, education and social support. While we also provided opportunities for educational group sessions, few participants regularly engaged in these sessions, suggesting that they did not consider their peers to be an important source of social support. This is in contrast to a previous study in which people living with HIV preferred exercising in groups, although participants in this study were not followed over time. 41 Participants’ reluctance to take part in group-based exercise classes offered at the YMCA or educational group sessions may in part be due to the varied schedule of the participants, as participants were not organized to exercise in groups or partners. However, independent exercise in a traditional gym may not be the best alternative for those in which ongoing social support is an important goal.
The benefits of exercise for people living with HIV are well established. 13,14 It is evident, however, that CBE programs cannot meet the diverse needs of all people living with HIV. Given the complexities of lives of many people living with HIV, the episodic nature of the disease and the mental and physical health challenges, it will be important to have a variety of exercise programming and delivery options to meet their needs and to determine who best benefits from a CBE program. Weekly access to a coach over a 24-week period was highly valued by our participants. Yet there were some who had anticipated that the coach would provide mental health and counselling supports, a service which is outside their scope of practice. It is worth highlighting that in 3 participants, the coaches made efforts to collaborate with other health providers to ensure that the exercise program complemented other exercise initiatives and was adapted to their health challenges and disabilities. CBE programs which provide comprehensive interprofessional support may be warranted for some. Indeed, Goulding et al found that in people living with HIV experiencing depression and/or mental health issues, exercise alone was insufficient to sustain improvements in quality of life and concluded that other supporting interventions are required. 42 Some people living with HIV may benefit from a more structured group approach which provides opportunities for peer interaction and support. 43 Peer-based models of physical activity, in which people living with HIV offer mutual support and motivation to exercise, may also be more financially sustainable than formal coaching models.
The longitudinal study design was a strength of this study which allowed us greater insights into the participants’ experiences over time. Additionally, our recruitment strategy ensured we had variation in gender, age, ethno-cultural background, time since diagnosis and experience with exercise. There is a possibility that those who completed the interviews were those most positive about the program and the most successful. However, there were a range of experiences with some participants critical of the program and stating that they were not likely to continue to exercise following the intervention. There were insufficient numbers of women to perform separate gender analyses. 44 Future work should examine gender-specific exercise experiences. 45
In conclusion, while participants in the study valued their experiences in CBE, they experienced challenges unique to living with HIV that need to be considered in program development. Given the diversity of needs of people living with HIV, it is unlikely that one program will meet the needs of this population. A menu of options and a coordinated care plan may be necessary in those with complex needs or who are experiencing an episode of ill health. Further research with people living with HIV, including quantitative studies to examine long term adherence to exercise, feasibility of sustained programs, and to identify who would most benefit from a CBE program is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Canadian Institutes of Health Research (CIHR) HIV/AIDS Community-Based Research Initiative CIHR FRN: 139685. Kelly K. O’Brien is supported by a Tier 2 Canada Research Chair in Episodic Disability and Rehabilitation.