
Abstract
Supplemental Questions
What do we already know about this topic?
The Short-Form HIV Disability Questionnaire (SF-HDQ) is a 35-item HIV-specific patient-reported outcome measure (PROM) developed to describe the presence, severity, and episodic nature of disability experienced by adults living with HIV.
How does your research contribute to the field?
To our knowledge, this is the first qualitative study to explore the utility and implementation of the SF-HDQ specifically in community-based settings from the perspectives of people living with HIV and community health providers.
What are your research's implications toward theory, practice, or policy?
Study results in perspectives from people living with HIV and community-based organization and community health center staff and volunteers perspectives toward the SF-HDQ in community-based settings, including considerations for future implementation within community-based contexts.
Introduction
People living with HIV can experience multi-morbidity at higher rates compared to the general aging population,1,2 which can increase the severity, complexity, and unpredictable nature of health consequences, collectively referred to as disability.3,4 Disability is defined by adults living with HIV as any physical, cognitive, mental-emotional symptoms, difficulties with day-to-day activities, challenges to social inclusion, and uncertainty about future health.3,4 People living with HIV can face additional challenges of ageism, stigma, mental health conditions, financial insecurity, limited access to long-term care housing, and lack of social support, further complicating disability over time.5–8
PROMs have a role in helping to better understand the needs of people aging with HIV by enhancing communication among patients and providers, facilitating goal setting and links to interventions, and ensuring timely and appropriate strategies, services, and interventions.9–11 HIV-specific PROMs are particularly relevant for person-centered HIV care; they go beyond traditional outcome measures of viral load or survival to describe person-centered outcomes (mental health, social inclusion, and uncertainty) and how these change over time,12–14 enhance communication by empowering people living with HIV to articulate their health challenges and needs, facilitate goal setting, and guide referrals to available services. 11 In clinical practice, PROMs can facilitate person-centered care by enhancing person-provider communication and identifying an individual's needs.9,10 At the community-based service delivery level, HIV-specific PROMs can help organizations to better understand the changing needs of individuals as they age with HIV, evaluate the impact of interventions, programs and models of service delivery, and inform areas of resource allocation for future programming and service provision. 11
We developed the HDQ, a 69-item PROM, to measure the presence, severity, and episodic nature of disability experienced by people living with HIV.15,16 Derived from the episodic disability framework, the HDQ possesses sensibility, reliability, and validity among adults living with HIV internationally.17–21 Using Rasch analysis we established a short-form version of the questionnaire (SF-HDQ) to enhance the feasibility for use in clinical practice. 22 This new 35-item SF-HDQ demonstrated structural validity and sensibility (face and content validity, and ease of use) for use with adults living with HIV in clinical settings in Canada, United Kingdom, and United States.22,23 In the clinical context, the SF-HDQ can measure health challenges and change over time, guide referral to specialists and services, facilitate goal setting and communication, and foster a multi-disciplinary approach to care. 23 However, hospital-based HIV clinics are distinct from community-based organizations, many of which are charitable non-profit settings that provide access to complementary health services to those living in underserved areas, and to those requiring additional or culturally accessible HIV and social support services (eg, food back, support groups) beyond the formal health system.24–26 The utility of the SF-HDQ in community-based organization settings and health centeres is unknown.
Our objectives were to (1) assess the sensibility (face and content validity, ease of usage, format) of the SF-HDQ, (2) explore perspectives on the utility of the electronic SF-HDQ in the community-based organization or community health center setting, and (3) identify considerations for implementation of the SF-HDQ in community-based organization or health care settings from the perspectives of adults living with HIV and community health providers in Canada.
Methods
Study Design and Setting
We conducted a descriptive mixed methods study design using quantitative (questionnaires) and qualitative (interview) methods of data collection. 27 This study was conducted at seven community-based settings, specifically five community-based organizations and two community health care centers sites across three cities and provinces in Canada. Sites in this study were identified by members of the team, who were representatives from HIV community-based organizations and community health care centers who identified measurement of disability as a research priority in HIV, aging, and rehabilitation. We defined community-based organization settings as non-profit charitable organizations without formalized medical services (eg, support groups, financial services, food banks); and community health care centers as settings embedded within the community that may be affiliated with a hospital, funded by the province, with access to comprehensive services offered by an interdisciplinary medical health care team. The five community-based organizations were in Toronto, Ontario (Alliance for South Asian AIDS Prevention (ASAAP), AIDS Committee of Toronto (ACT), Toronto People with AIDS Foundation (PWA), Vancouver, British Columbia (AIDS Vancouver); and Montreal, Quebec (AIDS Community Care Montreal (ACCM)). The two community health care centers were in Toronto, Ontario (St. Michael's Hospital Academic Family Health Team, Wellesley-St. Jamestown site) and Vancouver, British Columbia (Dr Peter Centre).
Patient and Public Involvement
This research was based on longstanding collaborations between community-academic-policy stakeholders in the field of HIV, aging, rehabilitation, and community-engaged research, who identified measurement of disability as a research priority in HIV, aging, and rehabilitation with the Canada-International HIV and Rehabilitation Research Collaborative.28–30 Our team includes community members living with HIV, clinicians, researchers, and representatives from HIV community-based organizations and community health centers. Community members were integrally involved in developing the original HDQ, identifying and prioritizing the need for a SF-HDQ and their role in this study. In this study, community collaborations involved adults living with HIV as “ambassadors” of the team, an engagement coordinator living with HIV, representatives from Community-Based Organizations (CBOs) (AIDS Committee of Toronto, AIDS Vancouver, ASAAP, AIDS Community Care Montreal), a specialty hospital (Casey House), community health centers (St. Michael's Hospital Academic Family Health Team, Wellesley-St. Jamestown site, Dr Peter AIDS Foundation/Dr Peter Centre), and Realize who foster guidance on the implementation, uptake, and knowledge translation of episodic disability in the context of HIV as a member of the core research team. Community members on the team guided recruitment and data collection, and participated in the interpretation of results.
Participants and Recruitment
We recruited adults living with HIV (≥18 years) and community health providers (staff, volunteers) across seven community-based settings in Canada who self-identified as having a role in addressing disability with HIV. Adults living with HIV were recruited using a recruitment poster. We used purposive sampling to obtain diversity among adults living with HIV across the lifespan, sex, gender, and ethnoracial background. We recruited community health providers using targeted recruitment of staff or volunteers working in HIV care who may or may not be living with HIV at community-based organizations or community health center sites identified by collaborators on the research team.
Data Collection
Data were collected remotely via Zoom 31 due to the COVID-19 pandemic and consisted of two parts (1) questionnaire completion/review and (2) a semi-structured interview. Participants living with HIV completed the SF-HDQ, 22 a Sensibility Questionnaire, a global rating scale of disability, and a demographic questionnaire electronically via Qualtrics 32 followed by a one-to-one semi-structured interview. Community health providers were asked to review the SF-HDQ and to complete the Sensibility Questionnaire, electronically (via Qualtrics), 32 before participating in the semi-structured interview. Three members of the team (MS, BT, GDS) were responsible for data collection, all of who possessed expertise conducting online interviews and administering questionnaires electronically with community-based research in the context of HIV, and who met regularly as part of the core community collaborator team to discuss impressions from the interviews, and refine the interview guide throughout.
Questionnaires
Short-Form HIV Disability Questionnaire (SF-HDQ): The SF-HDQ is a 35-item self-administered instrument developed to describe the presence, severity, and episodic nature of disability experienced by adults living with HIV across six domains: (1) physical, (2) mental-emotional, and (3) cognitive symptoms and impairments, (4) difficulties with day-to-day activities, (5) challenges to social inclusion, and (6) uncertainty about future health. 22 Participants were asked to rate the presence and severity of each health-related challenge and to indicate whether it fluctuated in the past week.
Sensibility Questionnaire: Derived from Feinstein's criteria for sensibility, 33 this questionnaire includes 18 statements (7-point response scale, from highly disagree to highly agree) asking about perspectives on purpose, face and content validity, method of administration, ease of usage and format of the SF-HDQ. 34 See Supplemental File 1 for the Sensibility Questionnaire.
Global Rating Scale of Disability: We administered a global rating scale of disability, asking participants living with HIV to check a box (minimum, moderate, or severe) that best described how they would rate their health-related challenges (or disability) that day.
Demographic Questionnaire: Participants living with HIV completed a demographic questionnaire comprised of items such as age, sex, gender, ethnoracial background, and concurrent health conditions.
Interviews
Utility: We conducted semi-structured interviews via Zoom 31 with adults living with HIV and community health providers. We asked about the utility of the SF-HDQ in practice, experience with completing or administering the SF-HDQ, strengths and challenges, feasibility, how and when it should be administered, who should administer it, and how often it should be administered (to capture the episodic nature of disability). See Supplemental File 2 for the Interview Guide. All interviews were audio recorded and transcribed verbatim.
Participants were provided with a CAD30 electronic gift card as a token of appreciation for taking part in the study.
Analysis
We derived sensibility findings from a combination of the sensibility questionnaire and interview data. Results pertaining to utility and implementation considerations were drawn entirely from the interview data.
Questionnaires. SF-HDQ:
We calculated median (25-75th percentiles) of SF-HDQ scores. We calculated severity and presence scores on an interval scale using algorithms developed through Rasch analysis (range 0-100). 22 Episodic scores included a simple sum transformed on a scale of 0-100. Higher scores indicate a greater presence, severity, and episodic nature of disability.
Sensibility questionnaire
We calculated median scores for each item. We considered the SF-HDQ sensible if median scores were ≥5 for adults living with HIV and ≥4 for community providers (7-point ordinal scale) for >80% of the items and if no items had median scores of ≤3, similar to criteria in our earlier HDQ sensibility assessment.18,34,35
Global rating scale of disability
We reported the number of participants who reported living with self-defined “minimum,” “moderate,” or “severe” health-challenges.
Demographic questionnaire
We calculated frequencies and proportions for categorical variables and medians and interquartile ranges (IQR) for continuous variables.
Interview data
We used conventional content analytical techniques and a team-based approach to analyze the interview data. 36 Conventional content analysis is an inductive approach to descriptive qualitative analysis whereby researchers avoid pre-conceived categories when coding data, commonly used when evidence on a concept is limited. In this study, we used conventional content analytical approaches to identify codes, and clustered into broader categories to describe perspectives related to our key concepts of interest in the study objectives: sensibility; utility; and considerations for implementation of the SF-HDQ. NVivo software Version 11 was used for data management. 37 The analytical working group comprised of 14 team members met two times. The group initially reviewed four transcripts independently and met to develop, by consensus, a preliminary list of codes based on the interview guide and the four transcripts. The lead analyst (MS) coded additional transcripts using the preliminary list of codes for the analytical working group to review and discuss. After all of the transcripts were coded, the analytical working group reviewed coding reports from the full data set focused on: utility and sensibility with quotations from adults living with HIV and community health providers. The working group met a second time to discuss specific considerations for SF-HDQ utility in community-based settings and the relationships between coding categories, key themes, and the study objectives.
Sample Size
Our sample size estimation was based on our qualitative methodology as the interview transcripts were the primary data source for the study. Based on our previous sensibility assessment of the original (long-form) HIV Disability Questionnaire, 34 the estimated number of interviews required to achieve an understanding of interview data, 38 and our previous sensibility assessment of the SF-HDQ with adults living with HIV and health care providers in the clinical context, 23 we anticipated 45 adults living with HIV and 10 community health providers across the seven community-based settings was sufficient to provide perspectives of sensibility and utility across the settings.
Ethical Approval and Informed Consent
We received ethics approval at the University of Toronto (Protocol #39967) to conduct this research with the community-based organizations (CBOs) and at St. Michael's Hospital (Protocol #21-091) with the St. Michael's Hospital Academic Family Health Team. We obtained written or verbal informed consent from all participants prior to administration of the questionnaires and the interview. During the consent process and throughout the data collection, members of the team administering the questionnaires and conducting the interviews (MS, BT, GDS) indicated that participants may choose not to answer any questions in the questionnaires or interview that they may not be comfortable with, and that they may choose not to answer questions for any reason and may stop taking part in the one-on-one interview at any time. If participants became upset during the interview or when filling out the questionnaires, members of the team referred participants to support staff at the health center or community organization (and provided contact details) and recommended discussing any feelings with their physician, counselor, or local support group, if available.
Results
We conducted 54 interviews (44 participants living with HIV and 10 community health providers) and administered the sensibility questionnaires between February 12, 2021 and January 17, 2022. Among the participants (both adults living with HIV and community providers), 33 (61%) were from the four community sites in Toronto, 15 (28%) were from the two community sites in Vancouver, and 6 (11%) were from the community site in Montreal, Quebec.
Characteristics of Participants Living with HIV
See Table 1 for characteristics of the participants living with HIV. Fifteen participants (34%) reported having minimum health-challenges, 27 (61%) reported having moderate, and 2 (5%) reported having severe health-challenges. All participants living with HIV reported they were taking anti-retroviral therapy and their viral load was undetectable (<50 copies/mL).
Characteristics of Participants Living with HIV (n = 44).
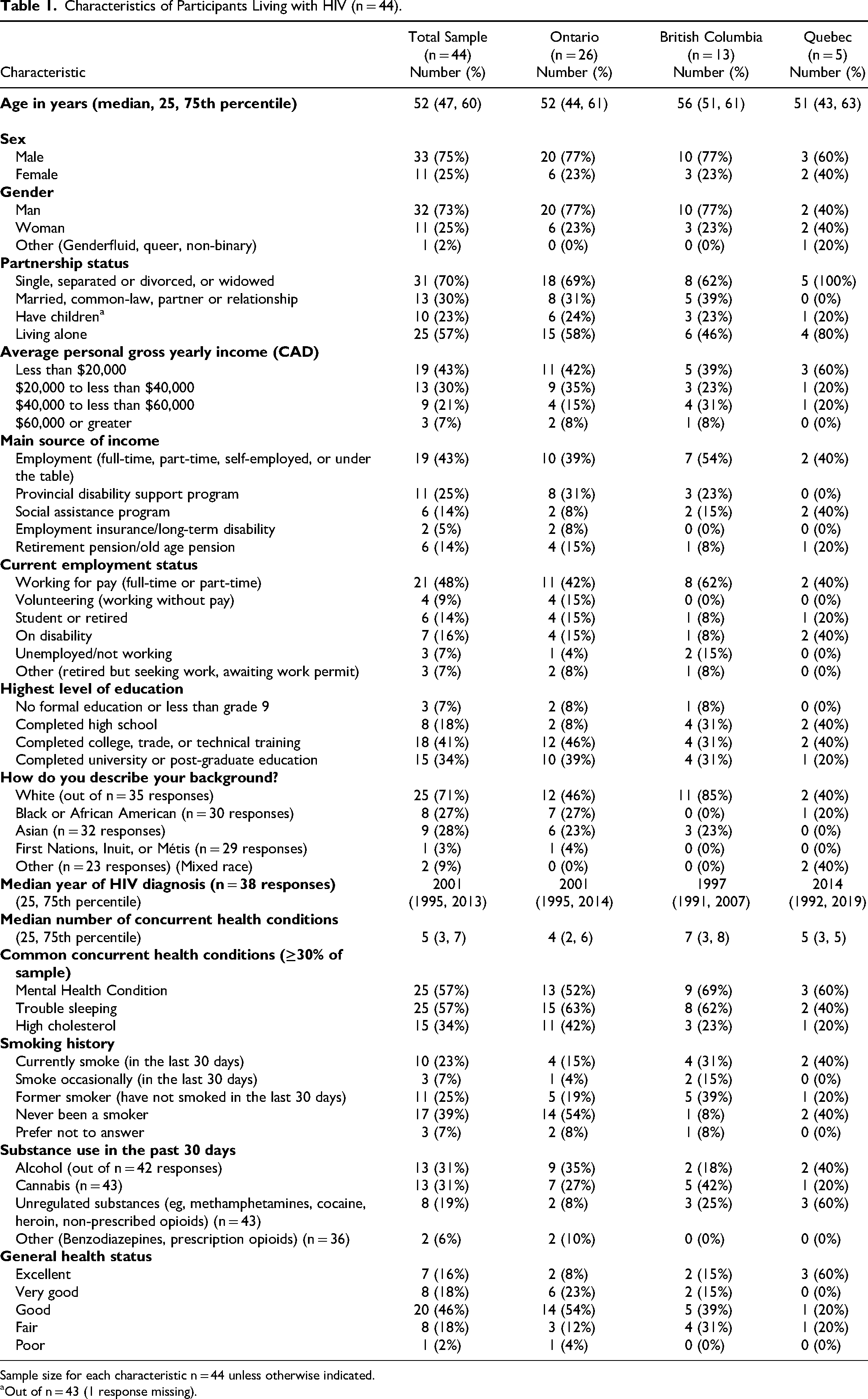
Sample size for each characteristic n = 44 unless otherwise indicated.
Out of n = 43 (1 response missing).
Among participants living with HIV (n = 44), the highest SF-HDQ scores for severity were in the uncertainty (median score: 42) and mental-emotional (median score: 41) domains. Highest SF-HDQ presence scores were in the cognitive (median score: 83) and mental-emotional (median score: 77) domains. Highest SF-HDQ episodic scores were in the physical domain reporting daily fluctuations in these health challenges within the past week. The majority of participants living with HIV (77%) considered themselves as having a “good day” on the day they completed the SF-HDQ in relation to their overall health (Supplemental File 3).
Sensibility, Utility and Implementation Considerations of the SF-HDQ
We describe sensibility findings derived in combination from the sensibility questionnaire and interview data. Results pertaining to utility and implementation considerations were drawn entirely from the interview data. We reference quotations with each participant number (P), the target population: participant living with HIV (PLWH) or community provider (CP); and province: Ontario (ON), British Columbia (BC), or Quebec (QC).
Sensibility
Results from the sensibility questionnaire and interviews indicate that the SF-HDQ possesses face and content validity and is easy to use with adults living with HIV in community-based settings. Sensibility questionnaire results indicate the SF-HDQ met our criterion for sensibility with adults living with HIV and community health providers with median scores ≥5 for 95% of the items (18/19) for participants living with HIV (Table 2); and ≥4 for 100% of the (19/19) for community health providers (Table 3).
Sensibility Questionnaire Results for Adults Living with HIV (n = 44).

Score range: 1-7.
Questionnaire responses were reversed for median scoring purpose.
Item that scored <5.
Sensibility Questionnaire Results for Community Health Providers (n = 10).

Score range: 1-7.
Questionnaire responses were reversed for median scoring purpose.
Interview findings support that the SF-HDQ is comprehensive, represents health-related challenges (disability) living with HIV and other health conditions, and adequately captures the episodic nature of disability. Participants indicated that the SF-HDQ was easy to complete, specifically that the items were easy to understand (ease of usage) and that the format was easy to use (adequate length, adequate response options).
Experiences Completing the SF-HDQ
Overall participants described that completing the SF-HDQ was a positive experience for them, as one participant described: “it was just like this check in that it didn’t actually say this could be a side effect of this and this. It wasn’t stuff put onto it. It was just like what's going on in your body and I appreciated that” (P1002-CP-ON).
SF-HDQ Items Captured Health-Related Challenges (Disability) Living with HIV in Community Settings
Participants described the SF-HDQ as comprehensively capturing the disability they experience living with HIV, on a daily or weekly basis, stating it was “all covered,” “whatever I’ve been experiencing, it was all there” (P1007-CP-ON). As one participant stated, “everything captured disability things that I didn’t even think of like not just your physical disability but mental disability. Things like that are just really important” (P23-PLWH-ON). Specific items that resonated with participants included financial issues, uncertainty or worry about the future, mental health, and taking part in social and community life. Some commented on items they felt were missing such as stigma, lipodystrophy, nutrition, and substance use. Many of these items are outside of disability, as one community provider noted: “maybe [it] just doesn’t fall into that sort of framework of disability but that's one thing that I thought of as definitely could like add to day-to-day challenges” (P1003-CP-QC).
HIV-Specific Versus Generic Phrasing of Some Items
Participants expressed mixed views on the HIV-specificity of some items in the questionnaire. In response to the item “I worry about my future health living with HIV” this participant stated: (this item) is valid you know … it's relevant to the context because I have HIV and sometimes you know I worry about my future because I’ve been taking medication for many years. I don’t know how these medications will play out in my body. … so sometimes I worry about my future health living with HIV… I worry about my lab test results such as CD4 count and viral load, I worry about the side effects of HIV treatments, that is valid. I worry about my income or financial security living with HIV, again the context is relevant. (P1004-CP-ON)
Alternatively, some participants commented on the broader relevance of items to other health conditions and contextual factors (such as the COVID-19 pandemic) that might influence responses to items such as worrying about the future, income security and stable housing. One participant explained “it might not specifically be HIV that's making it difficult to find housing” (P1003-CP-QC).
Capturing the Episodic Nature of Disability
Both groups of participants commented on the importance of the SF-HDQ capturing the episodic nature of disability and the benefit of reflecting on their episodic health trajectory since and before HIV diagnosis. Participants commented on how the SF-HDQ “makes you reflect” and the benefit of “looking back”, with one community provider highlighting how the episodic scale is unique: Sometimes with disability or with illness one of the things is that the idea of always telling your same story again I think is people get caught in a routine with the story and then they actually don’t talk about or they avoid talking about what's today and has that changed in the last seven days. I think that that's actually very helpful; that sort of focus helps to give perspective. (P1002-CP-ON)
One community provider expressed the desire for more description of the nature and extent of the episodic nature of disability: “If you’re going to ask me if it fluctuated over the week or if it's changed over the week, then me being able to explain to you how so, to what extent, would have been better” (P1006-CP-ON).
Participants had diverse viewpoints on the ideal timeframe for measuring fluctuations of health challenges with some commenting they “don’t find there's much of a change in one week” (P28-PLWH-ON) and a longer period such as a month may more likely capture fluctuations in health: a month would be more appropriate in my opinion just because a week… I mean I know HIV is episodic and whatnot. But… it doesn’t occur very often most of the time but it can occur. So, a week is a very short timeframe to make any difference. (P02-PLWH-BC)
Ease of Usage and Format
Participants stated that completing the SF-HDQ was “very easy and straightforward,” “easy to do,” “concise,” “simple,” and “clear.” The length of the SF-HDQ was adequate and the response options were “good,” “balanced,” with one PLWH referring to it as a “good grid” and noting “you can find where you are” (P37-PLWH-ON). Nearly all participants found the wording easy to understand, stating they “understood it well” and that while some questionnaires have “big words and some people don’t understand them” they had no problem understanding the SF-HDQ. Participants commented on how the SF-HDQ does not include “fancy words or such long words,” and has “no jargon” which facilitates usage among PLWH, particularly for participants where English may not be their first language.
While participants liked the provision of examples with the questions as it “adds some context to the question,” a few commented on how the double-barreled nature of the examples could lead to confusion if someone had difficulty with one activity (ie, climbing stairs) but not the other (ie, walking) as this participant stated: “for me appointments and medication are two different things”. … when you twin two things …it's like hmm, how do I answer this; one it could be a “yes” and the other one could be a “no.” (P24-PLWH-ON)
Finally, participants commented on the ease of electronic administration of the questionnaire. As one community provider stated: “I can easily hand this out to one of my community members and feel confident that anyone can do this” (P1006-CP-ON).
Utility
Community-Based Setting Use of the SF-HDQ
The majority of participants living with HIV and community providers believed the SF-HDQ would be useful in community-based settings, specifically for: (1) facilitating communication and fostering engagement with community, (2) taking a snapshot of health (disability) and tracking changes in disability over time, (3) guiding referrals to health services and supports, (4) fostering self-reflection, awareness of health and goal setting, and (5) informing community organization programs and planning. The process of completing the SF-HDQ was described by participants as fostering self-reflection, awareness of health, and goal setting.
Facilitating Communication and Fostering Engagement with Community
Participants described how the questionnaire could help clients communicate health-related issues, and facilitate engagement between community organization staff and clients. The SF-HDQ might enable adults living with HIV to “open up about themselves” and articulate health issues that they might not be comfortable discussing verbally, as indicated by this community provider: “by filling out a questionnaire it helps to give the answers without giving the answers…It does it in a way where the person doesn’t feel uncomfortable or puts them in a spot you know” (P12-PLWH-QC). Participants living with HIV reflected how the SF-HDQ “starts the conversation” and can “open up more room for dialogue” between community providers and adults living with HIV, which can help foster a conversation about strategies to address the health-related issues identified in the SF-HDQ.
With increased communication, participants described how the SF-HDQ could facilitate engagement with clients, helping community organization staff or volunteers to learn more about clients and their needs. Community provider participants noted that the SF-HDQ “would be very useful to get to know the client better,” stating that it includes items that they may not be routinely asked about, “we hardly ask about ‘are you worried about your future?’” Another potential use was: “as a tool before a [support] group starts to look at what the sort of temperature of the group is” (P1002-CP-ON).
Taking a Snapshot and Tracking Changes in Health (Disability) Over Time
Participants living with HIV and community providers described how the SF-HDQ could be used in community-based settings to help individuals and organizations assess health challenges at one time point or over time, identifying areas to address with services or supports. Participants viewed the SF-HDQ as a “quick snapshot” of health that provides “enough data that might highlight where the needs are for an individual” (P06-PLWH-ON), and “useful way to gauge just sort of where people are at in different areas of their life” (P1003-CP-QC) or a “holistic check-in” to periodically determine “whether that client or service user needs more support” (P8-PLWH-ON).
Participants indicated how the SF-HDQ may provide insight to measuring change in health over time: “the advantage is simply seeing your growth patterns and all that and what's really happening. A lot of times it's just in our head and we don’t see it” (P28-PLWH-ON). Some participants discussed how the SF-HDQ may be used as an evaluative tool to “document progress and change” and provide evidence of impact of community-based services or supports, as indicated by this participant: “I think it could be used as an after, so you do it before the group or your eight therapy sessions or whatever and then you would do it after and then also compare any change has happened” (P1002-CP-ON).
The utility of repeated administration in the context of the episodic nature of disability was described by one community provider: these kinds of questions will be great to track their progress or their movement to figure out ways to help them and to support their return to balance and recovery. … We’d track each time they took it. It doesn’t mean that the tracking would show some kind of progress …The first one they might be feeling great, the second one not so great and you know the third one not so great…but it would let us know ways that we could support the person….right now we don’t ask any questions about health. (P1010-CP-ON)
Guiding Referrals to Services and Supports
Both participants living with HIV and community health providers described how the SF-HDQ could guide referrals to services and programs. Community organization staff were viewed as having a direct role in addressing health challenges and as a conduit to facilitating referrals to members of the health care team. As one participant stated: “[the SF-HDQ], it kind of gives a good idea of what people are needing as they walk into the building like real time sort of” (P09-PLWH-BC). A community provider described how a case manager at a community organization may use SF-HDQ scores to inform referral to rehabilitation: I could see something like this informing a case manager … if there was a baseline score on which you would make a recommendation for this person to go see their doctor or whatever the most pressing issues are that might be impacting their lives and they would benefit from interventions. (P1008-CP-BC) I could see this being utilized by some of our peer navigators…especially in the areas of day-to-day activity, the cognitive one and the emotional one. … the peer navigator that works with seniors would definitely be able to utilize this with the work he does. … definitely plan services or seeing the barriers to health or any of the challenges the person would see. (P43-PLWH-BC)
Fostering Self-Reflection, Awareness of Health, and Goal Setting
Participants described the process of completing the SF-HDQ as a self-reflection tool that could facilitate goal setting for an individual living with HIV. Some participants described the SF-HDQ as a “body scan” or as a tool enabling them to “know where I am” and “see where my strengths and weaknesses are” stating “it enlightens you. It's very educational that way.” Others noted that it provides “some perspective on stuff because we can easily slip into the ‘oh woe is me’ and that's not always accurate” (P06-PLWH-ON). As one participant living with HIV described: there were some things that made me question and check in with myself about how I’m feeling about that. …it actually made me think.… it really kind of narrows down for me to …this is the problem or this is the worry right now and how can you tackle that or calm that down at least. (P23-PLWH-ON)
Fostering reflection and awareness of one's health was viewed as way to facilitate goal setting, identifying areas that an adult living with HIV may focus their efforts, as this participant stated: “when I was giving the answers… it also reminded me…I need to work on particular stuff because I’m not doing well. So that giving me a chance to look particular in my issues health and emotional issues. So it guided me” (P1007-CP-ON). Another participant described how receiving SF-HDQ scores could help them “understand what I’m going through and what area I should work like harder, which areas I should focus on taking care of myself and figure out my weakness, my strength” (P31-PLWH-ON). This participant referred to the SF-HDQ as a tool in the process for self-development, “if I feel the need to address some of these things that are listed in the questionnaire, I could use it as a self-development [tool], sometimes we experience challenges or we might be going through issues but we can’t pinpoint what these issues are. I think questionnaires bring these issues to light” (P13-PLWH-ON).
Informing Community Organization Programs and Planning
Some participants viewed the SF-HDQ as a tool that could be utilized by community-based organizations to “identify what's …needed in programming,” and “how to tailor services to what's most needed” and indicate “what type of programming we need to strive toward.” As one participant stated: “it could help the organization in terms of goal setting and planning. So, when you have data that supports the community and what the community needs, the data would help you to plan and get funding to support the issues that the community is having” (P13-PLWH-ON).
Implementation Considerations
Implementation considerations of the electronic SF-HDQ in community-based settings included strategies for administration and communication of questionnaire scores.
Administration
Considerations pertaining to administration included the importance of person-centered approaches for tailoring the mode of administration (use of technology, literacy, other health challenges), offering flexibility for administration (format, location, timing, frequency, persons administering, level of facilitation and supports available), burden of administration (time, conundrum of identifying health challenges with limited resources or supports to address them, logistical issues of community setting space, accessibility, and privacy), and the importance of buy-in from the community to utilize the tool. Table 4 includes participant quotes related to perspectives on the burden of administration and the need for person-centered approaches for administration of the electronic SF-HDQ in community-based settings.
Implementation Considerations for Administration of the Electronic SF-HDQ in Community-Based Settings.

Abbreviations: CP, community providers; PLWH, participant living with HIV; P, participant.
Communication of Scores
There were varied opinions around communicating SF-HDQ scores among clients and community organization staff and volunteers. Some participants living with HIV were comfortable sharing their scores with staff at the community agency while some indicated that they would prefer to share their SF-HDQ test scores with their health care professional. In terms of knowing their SF-HDQ score, there were diverse preferences expressed by participants living with HIV. Some described how knowing their scores could help them to identify areas to work on or changes in their overall health. Other participants living with HIV shared how knowing their score could lead to worrying, either about their health or the meaning of the scores. Both the importance of explaining how to interpret the SF-HDQ scores and the need to provide adults living with HIV with choice regarding who their scores from the SF-HDQ are shared with were identified in the interview findings (Table 5).
Implementation Considerations for Communicating Scores of the Electronic SF-HDQ in Community-Based Settings.
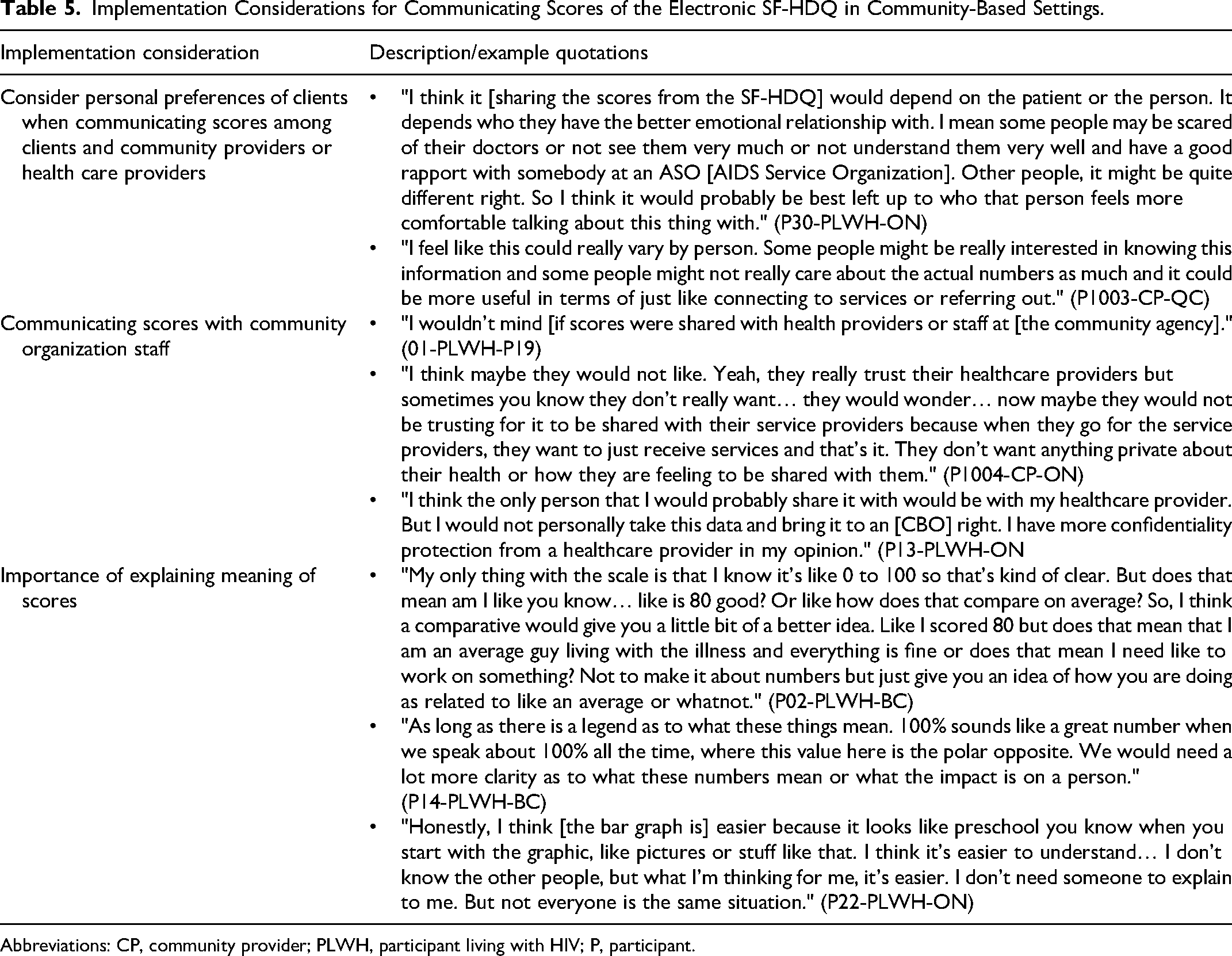
Abbreviations: CP, community provider; PLWH, participant living with HIV; P, participant.
Discussion
The SF-HDQ appears to demonstrate sensibility for use with adults living with HIV and community health providers across seven community-based organizations and community health centers in Canada. In these community-based settings, participants indicated the SF-HDQ possessed utility for facilitating communication and fostering engagement with the community, taking a snapshot of, and tracking changes in, disability over time, guiding referrals to health services and supports, and informing community organization programs and planning. The process of completing the SF-HDQ was described by participants as fostering self-reflection, awareness of health, and goal setting. Results highlight the need to use person-centered tailored approaches to administration, specifically providing options for mode and timing of administration, and communicating scores.
Results from this study suggest that the SF-HDQ is easy to understand with the length of the questionnaire appropriate and feasible to complete, and highlights the relevance of the episodic scale to experiences living with HIV. Increasingly PROMs in HIV care are recognized for their importance to consider outcomes beyond viral suppression such as symptoms, daily function, and health-related quality of life (HRQL). 39 The development of PROMs have emerged in the context of HIV, established to measure a range of health constructs in HIV ranging from HRQL, symptoms, psychological challenges, stigma, self-management, body and facial appearance, social support, and disability.39,40 Nevertheless, their measurement properties can vary. 41 The SF-HDQ and its multi-dimensional measurement of physical, cognitive, mental, and social health challenges address the call to incorporate person-centered experiences in assessing health outcomes that go beyond virological suppression. 42
While community providers positively commented on the utility of the SF-HDQ, some expressed hesitancy to use the SF-HDQ to identify health challenges when resources to address challenges are limited in the community setting. Challenges to implementation included: the burden of administration; a lack of space and personnel; and reluctance to measure disability with limited resources to address it. These challenges were similarly documented in a study that found that busy workloads posed challenges for taking up a PROM in community practice. 43 Authors highlighted the importance of choosing appropriate measures, co-creating PROMs with community staff, investing time and energy to PROM use, embedding PROMs into organizational culture while providing support with implementation in order for PROMs to be taken up for use in community. 43 Nevertheless, the burden of PROM use is a key barrier to their implementation. A panel of health professionals and persons living with HIV had opposing views on guidelines for PROM use. Persons living with HIV valued the use of PROMS (even without validation) viewing them as a contribution and useful for individualized care, whereas health professionals expressed negative impressions of PROM use citing an excessive number of PROMs and lack of time to administer. 44 These impressions may extend to community settings with limited resources, space, and personnel. Ultimately, having buy-in from all stakeholders will be critical for SF-HDQ uptake and use in community settings.
Participants highlighted the potential for the SF-HDQ as a communication tool to share information about disability across community and clinical settings, among the person living with HIV and their community and health provider team, as well as a way to foster self-reflection of health. Brief and comprehensive PROMs can enhance patient-provider communication and facilitate person-centered care.9,45,46 Utilization of the SF-HDQ may foster space to listen to patients’ concerns and acknowledge their experiences, with community providers. Our results align with a study that investigated PROM use as a way to support clinician and patient communication. PROM completion prompted patients to reflect on their health and provided the opportunity to raise issues with clinicians. 47 However, not all patients wished to discuss emotional or functional health-related quality of life issues with providers, suggesting PROM use will be shaped by the relationships that patient share with their providers. 47 Similarly, implementation considerations that emerged from this study highlighted the importance of personal preferences of persons living with HIV when communicating scores among clients and community providers. Future research may explore the interest and process for the transferability of SF-HDQ use (and scores) across community and clinical settings, and the desire to share scores between and among clinical and community health providers.
Results from this study highlighted the importance and ability of the SF-HDQ to capture the episodic nature of disability in community-based settings. To our knowledge, the HDQ (and SF-HDQ) is the first known to measure episodic nature of disability, and addresses the need to assess health outcomes beyond viral suppression. 39 The SF-HDQ can play a role in the pathway of care with value in measuring and identifying health challenges in order to gain knowledge on the need for rehabilitation and other health or supportive services.48,49 The SF-HDQ when administered cross-sectionally has the ability to assess the daily episodic nature of disability, higher SF-HDQ scores in the episodic scale tend to occur in the physical domain whereby these items (fatigue, pain) tend to fluctuate more on a daily basis as opposed to other domains (social inclusion) comprised of items we do not expect fluctuate daily (employment, relationships). 50 Measuring a concept that fluctuates within or over days, months, or years may be difficult to assess change over time. Future work should examine changes in episodic disability over time, and how these may represent clinically important changes to SF-HDQ scores.
This study builds on our previous work that assessed the utility, sensibility, and implementation considerations of the SF-HDQ and HDQ in clinical HIV care settings.21,23 While both confirmed the sensibility and utility of SF-HDQ across settings, findings from this study highlight unique implementation considerations for electronic administration of the SF-HDQ among participants in community-based settings. Discomfort with technology and lack of access to web-based platforms and lack of space at community organizations to administer the SF-HDQ on site can limit electronic questionnaire administration. 9 Web-based online administration of the SF-HDQ could facilitate portability of scores on a platform integrated across various sites and settings. Some persons living with HIV may find digital administration to be a barrier (eg, older population, those with cognitive impairments, low income). SF-HDQ administration will be dependent on the context and characteristics of the population served, which may differ within and across community settings. However, assessment of the SF-HDQ in both clinical and community settings highlighted the importance of buy-in from the community settings (or clinical settings) given the time constraints in a busy community setting with demands on clinician, or community organization staff and volunteer time. 23 Future work should consider an openly accessible platform for SF-HDQ to administer the SF-HDQ electronically and immediately provide scores and their interpretation.
Strengths and Limitations
Strengths of our study included our multi-methods multi-site approach with 54 participants, involving both persons living with HIV and community provider perspectives spanning seven different community contexts, assessing the utility of the electronic mode of SF-HDQ administration, and examining implementation considerations. Some community providers were also living with HIV, as many of the community providers offered insights into sensibility and utility from their personal lived experiences with HIV. Some participants in this study may have been collaborators on this study who were familiar with the SF-HDQ and more likely to consider the tool favorable. This study was limited to urban settings in a high-income country, and may not represent perspectives of persons living with HIV in more rural and remote regions. Our electronic administration of the SF-HDQ limited participation to individuals living with HIV who had access to and comfort with the use of technology in order to complete the questionnaires and, participate in a Zoom interview. Results highlight the importance of offering flexible options for SF-HDQ administration including a paper-based questionnaire for those with barriers to electronic administration, and providing support for those who might find the process of questionnaire completion distressing. Findings from this study will inform the development of a guide for SF-HDQ administration and scoring in community-based settings and increase knowledge about the intended utility of the questionnaire.
Measurement properties are specific to the context and population in which the tool is assessed, highlighting the importance of considering the characteristics of the participants living with HIV and community sites in this study. Our aim was not to compare sensibility and utility across sites, nor between adults living with HIV and community health providers. Given the heterogeneity across community contexts and target populations, we did not expect (nor was it a goal) to achieve saturation of themes. Rather, our aim was to obtain meaningful information through the exploration of the categories generated during the interviews, which could then be used to inform SF-HDQ sensibility and utility across a diversity of sites and perspectives. Results highlight the need for personalized tailoring of administration dependent on personal preferences and context.
Conclusions
The SF-HDQ possessed sensibility and utility for use in community-based settings in Canada with adults living with HIV. Community-based utility of the SF-HDQ included: facilitating communication and fostering engagement with community; taking a snapshot of disability and tracking changes over time; guiding referrals to services and supports; fostering self-reflection, awareness of health and goal setting; and informing community organization programs and planning. Considerations for implementation included flexible, person-centered approaches to mode and processes of administration, and communicating scores based on personal preferences among persons living with HIV. Future work should consider implementation strategies to foster feasible uptake and use of the SF-HDQ in community settings.
Supplemental Material
sj-doc-1-jia-10.1177_23259582231210801 - Supplemental material for Short-Form HIV Disability Questionnaire Sensibility, Utility, and Implementation Considerations in Community-Based Settings: A Mixed Methods Study
Supplemental material, sj-doc-1-jia-10.1177_23259582231210801 for Short-Form HIV Disability Questionnaire Sensibility, Utility, and Implementation Considerations in Community-Based Settings: A Mixed Methods Study by Kelly K. O’Brien, Francisco Ibáñez-Carrasco, Patricia Solomon, Soo Chan Carusone, Ann Stewart, Ahmed M. Bayoumi, Darren A. Brown, Adria Quigley, Puja Ahluwalia, Kristine M. Erlandson, Jaime H. Vera, Colm Bergin, Steven E. Hanna, Marilyn Swinton, Brittany Torres, Kiera McDuff, George Da Silva, Glen Bradford, Shaz Islam, Colleen Price, Joanne D. Lindsay, Carolann Murray, Natalia McClellan, Katrina Krizmancic, Praney Anand, Tammy Yates, Rosalind Baltzer Turje, Patrick McDougall, Vladislava Vlatka Maksimcev and Richard Harding in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-doc-2-jia-10.1177_23259582231210801 - Supplemental material for Short-Form HIV Disability Questionnaire Sensibility, Utility, and Implementation Considerations in Community-Based Settings: A Mixed Methods Study
Supplemental material, sj-doc-2-jia-10.1177_23259582231210801 for Short-Form HIV Disability Questionnaire Sensibility, Utility, and Implementation Considerations in Community-Based Settings: A Mixed Methods Study by Kelly K. O’Brien, Francisco Ibáñez-Carrasco, Patricia Solomon, Soo Chan Carusone, Ann Stewart, Ahmed M. Bayoumi, Darren A. Brown, Adria Quigley, Puja Ahluwalia, Kristine M. Erlandson, Jaime H. Vera, Colm Bergin, Steven E. Hanna, Marilyn Swinton, Brittany Torres, Kiera McDuff, George Da Silva, Glen Bradford, Shaz Islam, Colleen Price, Joanne D. Lindsay, Carolann Murray, Natalia McClellan, Katrina Krizmancic, Praney Anand, Tammy Yates, Rosalind Baltzer Turje, Patrick McDougall, Vladislava Vlatka Maksimcev and Richard Harding in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582231210801 - Supplemental material for Short-Form HIV Disability Questionnaire Sensibility, Utility, and Implementation Considerations in Community-Based Settings: A Mixed Methods Study
Supplemental material, sj-docx-3-jia-10.1177_23259582231210801 for Short-Form HIV Disability Questionnaire Sensibility, Utility, and Implementation Considerations in Community-Based Settings: A Mixed Methods Study by Kelly K. O’Brien, Francisco Ibáñez-Carrasco, Patricia Solomon, Soo Chan Carusone, Ann Stewart, Ahmed M. Bayoumi, Darren A. Brown, Adria Quigley, Puja Ahluwalia, Kristine M. Erlandson, Jaime H. Vera, Colm Bergin, Steven E. Hanna, Marilyn Swinton, Brittany Torres, Kiera McDuff, George Da Silva, Glen Bradford, Shaz Islam, Colleen Price, Joanne D. Lindsay, Carolann Murray, Natalia McClellan, Katrina Krizmancic, Praney Anand, Tammy Yates, Rosalind Baltzer Turje, Patrick McDougall, Vladislava Vlatka Maksimcev and Richard Harding in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors acknowledge those who volunteered their time to participate in this research as well as staff and volunteers in the community-based organization settings who supported the implementation of this research. We thank the following community-based organization and community health center settings for their collaborations and support in this research including the Alliance for South Asian AIDS Prevention (ASAAP), AIDS Committee of Toronto (ACT), Toronto People with AIDS Foundation (PWA), St. Michael's Hospital Academic Family Health Team, Wellesley-St. Jamestown site, Dr Peter Centre/Dr Peter AIDS Foundation, AIDS Vancouver, and AIDS Community Care Montreal (ACCM). Kelly K. O’Brien was supported by a Canada Research Chair (Tier 2) in Episodic Disability and Rehabilitation from the Canada Research Chairs Program. Ahmed M. Bayoumi was supported by the Fondation Alma and Baxter Ricard Chair in Inner City Health at St. Michael's Hospital and the University of Toronto.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Canadian Institutes of Health Research (Funding Reference Number: CBR-170102). Kelly K. O’Brien was supported by a Canada Research Chair (Tier 2) in Episodic Disability and Rehabilitation from the Canada Research Chairs Program. Ahmed M. Bayoumi was supported by the Fondation Alma and Baxter Ricard Chair in Inner City Health at St. Michael's Hospital and the University of Toronto.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.