
Abstract
Women with HIV (WWH) may be more vulnerable to cognitive impairment than men with HIV (MWH), which may be explained by the direct effects of HIV or by sociodemographic and psychiatric characteristics. We recruited 105 people with HIV (PWH; 76 women) with incomplete antiretroviral therapy adherence, comorbid major depressive disorder, and socioeconomically disadvantaged backgrounds. Participants completed neuropsychological testing and measures gathering sociodemographic, medical, and psychiatric information. We compared WWH and MWH cognitive performance using unadjusted and adjusted regressions, and within each respective group, we explored predictors of cognitive performance. Results showed no significant between-sex differences in cognitive performance, both globally and within domains. Fewer years of education (β = 0.94), illiteracy (β = 4.55), and greater food insecurity (β = −0.28) predicted lower cognitive performance in WWH but not MWH. We conclude that sex differences in PWH are likely due to sample characteristics representing broader inequalities, rather than true biological differences.
Introduction
Although some studies suggest that women with HIV (WWH) may be more vulnerable to cognitive impairment than men with HIV (MWH),1–10 this finding is not replicated consistently across studies.11–16 A recent systematic review of 11 studies summarizing this literature suggested that WWH perform more poorly in the cognitive domains of motor skills, information processing speed, audioverbal learning and memory, and executive functioning. 17 Within each of these domains, fewer than 50% of the studies that measured performance in that particular domain found WWH performed more poorly. The rest found no sex differences in performance. Six studies included in the review measured global cognitive performance; none of those 6, found WWH performed more poorly than MWH after analyses were adjusted for disease and demographic characteristics.
A recent meta-analysis of 6 studies in this literature 18 found small performance differences between WWH and MWH in 3 specific cognitive domains. WWH tended to perform significantly more poorly than MWH on tests measuring motor skills, visuospatial learning, and visuospatial memory, although effect sizes were small (d = −0.16, −0.43, and −0.30, respectively). The meta-analysis detected no sex differences in global cognitive performance and in performance in other cognitive domains (eg, information processing speed, attention and working memory, audioverbal learning, audioverbal memory, and executive functioning [verbal fluency, inhibition, and switching]).
HIV disease factors may contribute to the manifestation of sex differences in cognitive performance. People with HIV (PWH) who have suboptimal antiretroviral therapy (ART) adherence and who therefore may not have well-controlled HIV disease factors (eg, viral load and CD4 count) are at greater risk for developing HIV-associated cognitive impairment.19,20 Some studies have found that WWH have less optimal ART adherence than MWH.21,22 Of particular interest here is that a few studies also report that WWH may have higher levels of systemic immune activation and inflammation in response to HIV infection, which may contribute to higher rates of cognitive impairment.10,23–25
Significant sex differences in cognitive performance may also be explained (at least partially) by sex-based variation in sociodemographic and psychiatric characteristics, such as level of educational attainment and presence/severity of depressive symptomatology. 26 For instance, Sundermann et al 27 found that statistically significant sex differences in global cognitive performance no longer existed after analyses were adjusted for lower reading levels in WWH. Women are also known to have higher rates of depression than men,28–31 which could contribute to impaired cognitive performance.32,33
Hence, the inconsistent appearance of sex differences in HIV neuropsychology studies might be explained by variability in the magnitude of between-sex sociodemographic and psychiatric differences across studies. In other words, if a study finds differences in cognitive performance between WWH and MWH, those differences might arise from study-specific sampling issues or might represent broader structural and psychosocial inequalities between sexes in the populations from which they are drawn. In contrast, a study finding no such performance differences might have sampled from a population where there are less marked sex-based structural and psychosocial inequalities. For instance, in samples drawn from populations where women have less overall access to education, restricted access to high-quality education, or a higher likelihood of greater depression severity, WWH will likely perform more poorly on cognitive testing.34–38
In low-and-middle-income countries (LMICs), women often experience a disproportionate burden of poverty, greater levels of stress and trauma, and greater food insecurity.39–44 All of these are associated with lower performance on cognitive tests generally,45–48 and with lower performance in PWH specifically.49,50 Furthermore, in most LMICs HIV prevalence is highest in women and in communities with higher levels of poverty, poorer education, and less access to socioeconomic opportunities. Hence, it is worth considering the contribution of these factors to lower cognitive test performance of WWH in these populations. 51
Despite this growing circumstantial evidence that sex differences in the cognitive performance of PWH might be driven by sociodemographic (including psychosocial) and psychiatric factors, these variables are not routinely measured in HIV neuropsychology research studies.
South Africa has the highest number of PWH in the world, two-thirds of whom are women.51,52 Therefore, the question of whether WWH are more vulnerable to cognitive impairment than MWH, and which factors might contribute to this differential vulnerability, is of particular importance in this setting. Consequently, the aim of the current study was to compare global and domain cognitive performance in a well-defined and clinically important population of South African WWH and MWH, with a particular focus on the performance contributions of HIV disease variables related to incomplete ART adherence (eg, greater viral load, lower current, and nadir CD4 count), depression severity, and psychosocial factors (eg, quality of life and food security). To that end, we sampled from a population of PWH with incomplete ART adherence, current major depressive disorder (MDD), and a socioeconomically disadvantaged background—due to the factors outlined in the review above, sex differences are more likely to manifest in a group with these characteristics than in the general population of PWH. In other words, if sex differences in cognitive performance exist in South African PWH, then we would be more likely to find them in this sample and we could explore both biological and psychosocial effects driving the differences. Research on such clinically important samples is vital: it helps inform public health interventions that focus on the increased risk for HIV-related morbidity and potential for onward transmission of the virus in this group.
Based on extant findings in the HIV neuropsychology literature, we tested these specific hypotheses: (1) WWH will perform more poorly than MWH in the domains of motor skills and visuospatial learning and memory; (2) sociodemographic (eg, level of education and literacy), psychosocial (eg, quality of life and food security), and psychiatric (eg, depression severity) factors will be associated with cognitive performance in both WWH and MWH.
Materials and Methods
Setting and Participants
Data were collected, as part of a larger research program, from 2 primary care clinics in Khayelitsha, a peri-urban community in Cape Town, South Africa.53–55 Khayelitsha was established under the principle of racial segregation executed by the apartheid regime. As a consequence of this legacy, today almost all of its residents are Black African and it is one of the poorest areas of Cape Town. Most adult residents of Khayelitsha speak isiXhosa as a first language. Fewer than one-third of those residents have completed high school, and there are high levels of HIV infection, crime, and unemployment.56–60
Participants were 105 PWH. Inclusion criteria were (a) age ≥ 18 years; (b) HIV-seropositive status (confirmed via medical record); (c) current diagnosis of MDD as measured on the Mini International Neuropsychiatric Interview, Version 7.0 (MINI) 61 ; and (d) having failed first-line ART (ie, being identified by the community clinic as not having collected their medication regimen for > 3 months).
Because we wanted the sample to be representative of the clinical population of interest (ie, PWH with MDD and incomplete ART adherence), we did not exclude participants with medical and psychiatric comorbidities (other than those noted below) and/or other factors that could influence cognitive performance. The only exclusion criteria were (a) active and untreated serious mental illness (eg, psychosis or mania) that would interfere with study participation, (b) inability or unwillingness to provide informed consent, and (c) lack of sufficient fluency in English or isiXhosa. Participants using antidepressants were eligible if they met criteria for a current depressive episode; however, they had to have been on a stable antidepressant regimen and dose for at least 2 months.
Materials
Cognitive Assessment
The neuropsychological battery comprised 12 standardized tests, each of which assessed performance in 1 of 7 cognitive domains commonly affected by HIV. 62 We clustered tests into cognitive domains according to theoretical knowledge about the construct of each test63,64 and according to standard practice in the field of HIV neuropsychology.65–68 This battery of tests has been used extensively in studies of South African PWH.67,69
The domains, tests, and outcome variables were: (1) executive functioning, as measured by the Color Trails Test 2 (CTT2)—completion time; Wisconsin Card Sorting Test (WCST)—perseverative errors; (2) verbal learning and memory, Hopkins Verbal Learning Test-Revised (HVLT-R)—total across the 3 immediate recall trials, total on the delayed recall trial; (3) visuospatial learning and memory, Brief Visuospatial Memory Test-Revised (BVMT-R)—total across the immediate recall trials, total on the delayed recall trial; (4) verbal fluency, category fluency test—total number of animals/total number of fruits and vegetables named in 1 min; (5) attention/working memory, Wechsler Memory Scale-Third Edition (WMS-III) Spatial Span subtest—total raw score; Wechsler Adult Intelligence Scale-Third Edition (WAIS-III) Digit Span subtest—total raw score; (6) processing speed, CTT1—completion time; WAIS-III Digit Symbol Coding subtest—total raw score; WAIS-III Symbol Search—total raw score; (7) motor skills, Grooved Pegboard Test (GPT) dominant (DH) and nondominant hand (NDH)—completion time; Finger Tapping Test DH and NDH—completion time.
Tests were administered in either English or isiXhosa, depending on the participant's preference, by a bilingual neuropsychology technician. AJD, a registered clinical neuropsychologist, supervised test administration, and scoring protocols.
Measures
Sociodemographic Variables
Participants self-reported basic sociodemographic information (ie, gender, age, highest level of education, monthly household income, primary language, and employment status) as well as details of their school performance (eg, whether they had ever been held back or repeated a year in school, whether they were fully literate).
Psychosocial and Socioeconomic Variables
The Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q) 70 assessed overall satisfaction with the quality of daily life. A modified version of the Adult AIDS Clinical Trials Group (ACTG) SF-21 71 assessed health-related quality of life (asking, for example, if health interferes with or limits physical, social, or cognitive functioning and emotional wellbeing). The Household Food Insecurity Access Scale (HFIAS) 72 measured household food insecurity. Each of these was completed by interviewer-administered self-report.
HIV Disease Variables
HIV viral load and current CD4 cell number were extracted from medical records. Participants self-reported whether their nadir CD4 count had ever been below 100 cells/μL. If participants did not have recent (1-month) testing, we collected blood samples (see reference 54 for additional detail). Details regarding ART regimens (ie, reinitiated on first line, second line, or third line) were also extracted from the participant's medical record.
Medical History
Participants were classified as having a significant history of neurological problems if they reported ever having experienced one or more of the following: closed or open head injury with loss of consciousness > 30 min; stroke; coma; epilepsy; seizure without a diagnosis of epilepsy; and bacterial meningitis.
Participants were classified as having a significant history of vascular risk factors if they reported 2 or more of the following: any heart problem (eg, coronary artery disease, heart arrhythmia, or other heart diseases); heart attack; diagnosis of hypertension (irrespective of whether they were on medication or not); diagnosis of diabetes; history of having smoked cigarettes.
Psychiatric Variables
Psychiatric disorders were diagnosed using the MINI structured diagnostic interview. 61 This interview was conducted by a psychiatric nurse and supervised by a clinical psychologist. The Alcohol Use Disorders Identification Test (AUDIT; cut off >20) 73 was used to identify high-risk alcohol use. The Hamilton Rating Scale for Depression (HAM-D)74,75 was used to assess depression severity.
Statistical Analyses
We used R version 4.1.2 (2021-11-01) and RStudio version 2021.09.0 to complete all analyses, with the threshold for statistical significance set at α = .05.
First, we calculated sample descriptive statistics for the WWH and MWH groups and used t-tests (or Welch two-sample t-tests when groups had unequal variance) and chi-square analyses (or Fisher's exact tests if cell sample sizes were too small) to investigate between-group differences on sociodemographic, psychosocial, medical, and psychiatric variables.
Second, we processed and standardized the neuropsychological data. Normative standards for the tests were based on raw control data collected in previous studies conducted by the UCT HIV Mental Health Research Unit.69,76,77 Data were provided on personal request from co-authors JJ (personal communication, November 2017) and HG (personal communication, June 2018). To assure similarity across key sociodemographic (age, ethnicity, language, and education), psychosocial, and socioeconomic characteristics, these data were collected between 2008 and 2016 from healthy community-dwelling individuals (N = 233) who presented at the same community clinics in Khayelitsha from which the current sample was recruited. In the studies that collected the control data, participant inclusion criteria were (1) HIV seronegative, (2) ≥ 18 years of age, and (3) at least 5 years of formal education. Exclusion criteria were the presence of (1) a major psychiatric condition, (2) neurological disease that could affect brain integrity, (3) lifetime history of head injury resulting in loss of consciousness >30 min, or (4) current substance use disorder.
We used the control data to calculate demographically corrected z-scores (M = 0, SD = 1), using standard regression-based norming processes.65,78 Therefore, raw scores were adjusted if sex, years of education, and age were significantly associated with cognitive test performance in the normative sample. This process ensured that z-scores were corrected for any sex differences in the control data. The z-scores were then converted to demographically corrected T-scores (M = 50, SD = 10). If participants had z-scores more than 5 SD below the mean, the conversion to a T-score resulted in negative value. In these cases, we assigned a score of 0, the lowest possible T-score to maintain the clinical significance of the low performance. Neuropsychological data were summarized into domain and global T-scores by taking the average of T-scores within each domain and then the average across domain T-scores.
Third, bivariable linear regression models compared domain and global T-scores between the WWH and MWH groups.
Fourth, multivariable linear regression models compared domain and global T-scores while adjusting for potential confounders (ie, sociodemographic, psychosocial, medical, and/or psychiatric variables that earlier analyses had identified as being significantly different between the WWH and MWH groups).
Finally, a secondary subanalysis focused on the WWH and MWH groups separately investigated univariable associations with the global T-score, using linear regression models. Variables significantly associated with global T-scores were entered into multivariable linear regression models to determine those that best explained cognitive performance in each of the WWH and MWH groups. A backwards stepwise approach was used for model building (ie, the variable with the smallest t-value was removed from the model first). Cook's D was used to investigate influential outliers. A similar analysis conducted on the whole sample is presented in another manuscript. 55
Ethical Approval and Informed Consent
The study protocol was approved by the University of Cape Town (UCT) Faculty of Health Sciences Human Research Ethics Committee (HREC 010/2018 and HREC 010/2014) and the University of Miami Institutional Review Board (IRB Study Number: 20150399). All patients provided written informed consent prior to enrollment in the study.
Results
Participant Characteristics
The sample included 76 WWH and 29 MWH. As Table 1 shows, analyses detected no significant between-group differences with regard to most sociodemographic and clinical variables. However, MWH had significantly fewer years of education and a significantly worse HIV disease profile (ie, higher HIV RNA viral loads and lower current CD4 counts) than WWH. Moreover, a significantly greater proportion of MWH than WWH met the AUDIT criterion for high-risk alcohol use. Finally, WWH scored significantly lower than MWH on the ACTG SF-21, indicating that they reported experiencing worse health-related quality of life.
Sample Sociodemographic and Clinical Variables: Descriptive Statistics (N = 105).

ACTG SF-21: Adult AIDS Clinical Trials Group SF-21; ART: antiretroviral therapy; AUDIT: Alcohol Use Disorders Identification Test; ESE: effect size estimate; HAM-D: Hamilton Rating Scale for Depression; HFIAS: Household Food Insecurity Access Scale; HIV: human immunodeficiency virus; MWH: men with HIV; Q-LES-Q: Quality of Life Enjoyment and Satisfaction Questionnaire; WWH: women with HIV; ZAR: South African Rands.
aThe effect size here is estimated by Cohen's d.
bWelch t-test used due to unequal between-group variance.
cHigher score indicates greater food insecurity.
dScore recorded as a percentage.
eThe effect size here is estimated by the Cramer's V statistic.
fSelf-reported nadir CD4 < 100.
gFisher's exact test used instead of conventional chi-square analysis due to small group size.
hHigh-risk alcohol use indicated if AUDIT score > 20.
*P < .05
Differences in Cognitive Performance Between WWH and MWH
Unadjusted linear regression models detected no significant sex differences with regard to either global or domain T-scores (see Table 2). For the most part, mean global and domain T-scores for both the WWH and MWH groups fell within the average range of cognitive performance (ie, T = 45-54). The only exceptions were the T-scores for audioverbal learning and memory and executive functioning, both of which fell within the low average range for both WWH and MWH. 79
Cognitive Test Performance: Descriptive Statistics and Sex Differences (N = 105).
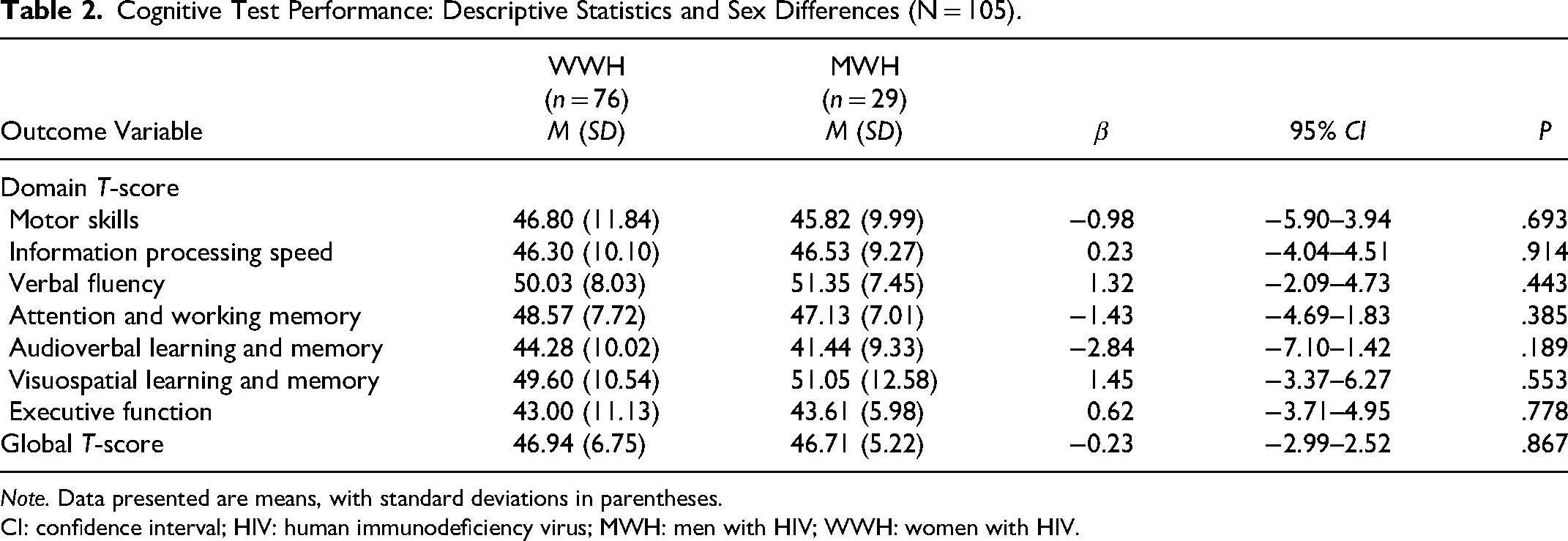
Note. Data presented are means, with standard deviations in parentheses.
CI: confidence interval; HIV: human immunodeficiency virus; MWH: men with HIV; WWH: women with HIV.
Linear regression models that adjusted for covariates (ie, potentially confounding sociodemographic, psychosocial, medical, and/or psychiatric variables) also detected no significant sex differences with regard to either global or domain T-scores (see Table 3).
Cognitive Test Performance: Sex Differences When Controlling for Covariates (N = 105).
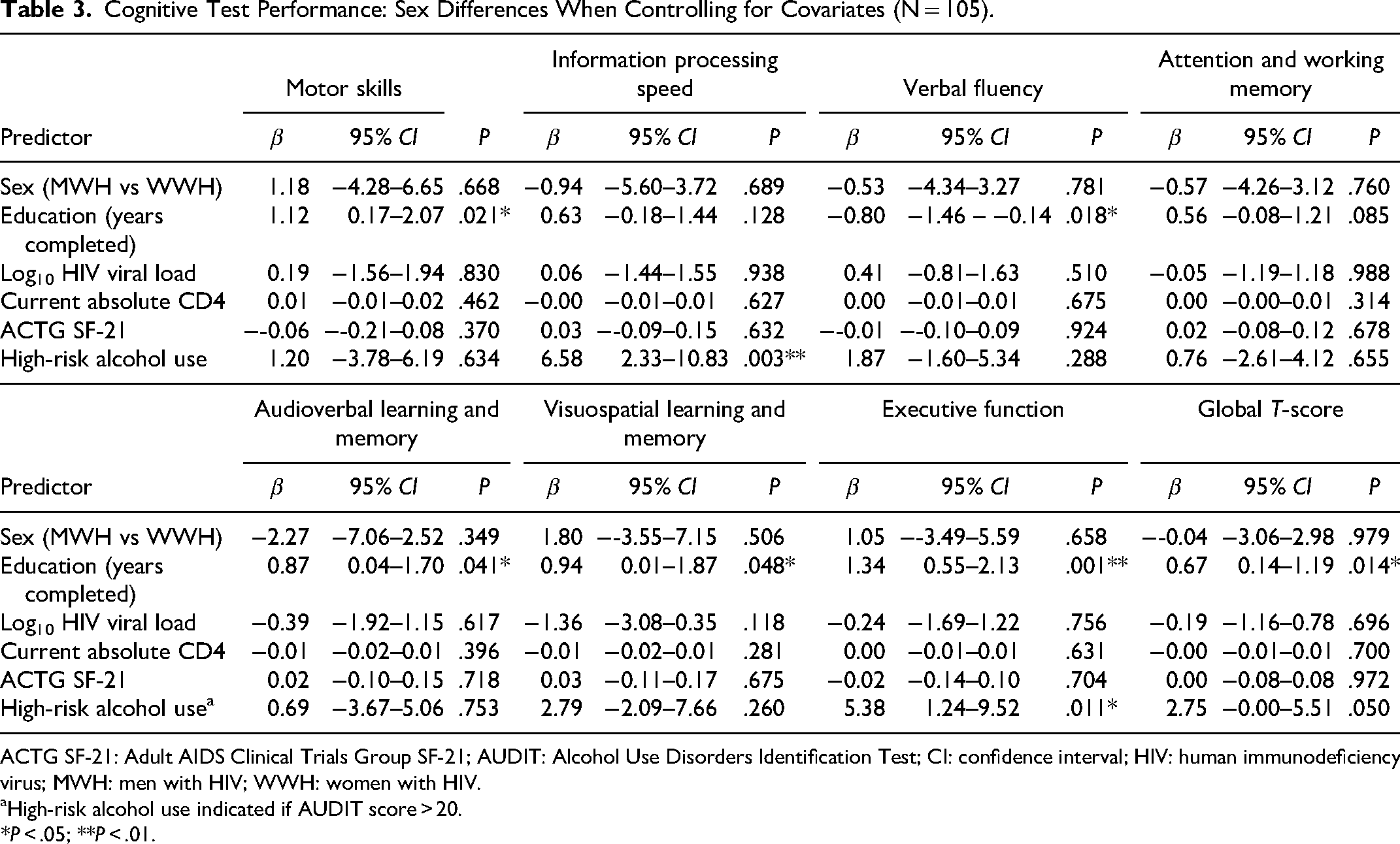
ACTG SF-21: Adult AIDS Clinical Trials Group SF-21; AUDIT: Alcohol Use Disorders Identification Test; CI: confidence interval; HIV: human immunodeficiency virus; MWH: men with HIV; WWH: women with HIV.
High-risk alcohol use indicated if AUDIT score > 20.
*P < .05; **P < .01.
Associations With Cognitive Performance in WWH and MWH
For WWH, level of education, HFIAS score, and literacy (ie, whether the participant was illiterate or not) were significant predictors of global T-score (see Table 4). For every year of education completed, the global T-score increased by 0.94 points; for every one unit increase in HFIAS score (ie, every one unit increase in food insecurity), the global T-score decreased by 0.28 points; and for WWH who reported being literate, global T-score was, on average, 4.55 points higher than WWH who were illiterate.
Cognitive Test Performance: Within-Group Univariable Associations With Global T-Score (N = 105).

ACTG SF-21: Adult AIDS Clinical Trials Group SF-21; ART: antiretroviral therapy; AUDIT: Alcohol Use Disorders Identification Test; CI: confidence interval; ESE: effect size estimate; HAM-D: Hamilton Rating Scale for Depression; HFIAS: Household Food Insecurity Access Scale; HIV: human immunodeficiency virus; MWH: men with HIV; NA: not applicable; Q-LES-Q: Quality of Life Enjoyment and Satisfaction Questionnaire; WWH: women with HIV.
The effect size here is estimated by Pearson correlation.
Removed a participant's data from the analyses because was an influential outlier. Cook's D for this participant's models with age, education, HFIAS and literacy are 0.14, 0.18, 0.24, and 0.18, respectively.
Removed an outlier who had a monthly household income of ZAR15000 (> 4 SD above the mean for MWH) and whose data were therefore disproportionately influencing the model.
The effect size here is estimated by point-biserial correlation.
Self-reported nadir CD4 < 100.
High-risk alcohol use indicated if AUDIT score > 20.
*P < .05.
When building the multivariable linear regression models to determine the best model of global cognitive performance in WWH, we entered the 3 variables whose individual associations with global-T score were statistically significant: education (years completed), HFIAS score, and literacy.
The first iteration of the multivariable model indicated that literacy had the smallest t-value. Hence, we removed that variable and reran the model. Comparing this model to the previous one showed that the removal made no significant difference to overall predictive power (P = .276).
Therefore, the final model (adjusted R2 = .12; P = .004) included years of education and HFIAS score. For every year of education completed, global T-score increased by 0.82 points (CI: 0.06, 1.59; P = .036) and for every one unit increase in HFIAS score, global T-score decreased by 0.24 points (CI: −0.44, −0.03; P = .023), on average. Data from one participant were removed from the analyses because they contained influential outliers (Cooks’ D = 0.23).
For MWH, analyses detected no significant univariable predictors of global T-scores (see Table 4). Hence, we could not build a multivariable linear regression model of global cognitive performance.
Discussion
This study set out to investigate (a) if there were differences in cognitive performance between WWH and MWH in a distinct and clinically important sample of PWH with incomplete ART adherence, comorbid major depressive disorder, and a background of socioeconomic disadvantage, (b) the sociodemographic, medical, and psychiatric variables associated with cognitive performance within the WWH and MWH groups.
Despite the small sample of MWH (n = 29) in this study, the findings we report are novel and important because the sample was drawn from a particularly vulnerable population of PWH: those with incomplete ART adherence, a background of socioeconomic disadvantage, and a comorbid mood disorder. We did not exclude from participation any individual with medical and psychiatric comorbidities (other than active and untreated serious mental illness) and/or other factors that could influence cognitive performance because we wanted to ensure our sample represented the population of PWH attending primary care clinics in South Africa. These PWH are important to study because they are especially vulnerable to HIV-related morbidities and there is an increased risk for the onwards transmission of the virus. Moreover, the specific adherence, psychosocial, sociodemographic, and psychiatric characteristics of our sample means that sex differences in cognitive performance are more likely to manifest in this group than in the general population of PWH. These sex differences, in this population, have not been described before.
Regarding sample sociodemographic and clinical characteristics, analyses detected several significant differences between the MWH and WWH groups. First, on average MWH had significantly fewer years of education than WWH. Broadly speaking, this statistic reflects the current state of the educational landscape in South Africa. Government school enrollment statistics report relative equality in access to education for men and women and note that, if anything, a slightly greater proportion of females are enrolled in secondary and tertiary level education.80–82 Many non-South African studies have found the opposite pattern2,7,27; these data may reflect the persistent global gap in educational attainment and opportunity between women and men. 41
Second, a significantly greater proportion of MWH than WWH met the criteria for high-risk alcohol use. This sex disparity is well-known in the general population of PWH, 83 including in South Africa.84,85
Third, MWH had a significantly worse HIV disease profile (ie, higher HIV RNA viral loads and lower current CD4 counts) than WWH. Similar sex differences have been reported in many studies.1,7,8,10 In South Africa, MWH are less likely than WWH to seek access to HIV care; if they do seek such access, they tend to present later than WWH. Hence, they are more likely to present with more advanced disease and to have increased mortality risk.86,87 Several mechanisms have been offered to explain this gender disparity. These include gender differences in health-seeking behavior, a generally higher mortality risk for men than women in South Africa, and the fact that South African public health systems prioritize maternal and child services. 88
Despite this sample of MWH having a worse HIV disease profile, WWH experienced worse health-related quality of life. WWH reported to a significantly greater degree than MWH that their poorer health interfered with their physical, occupational, social, and cognitive functioning, and reduced their emotional wellbeing. Similar results have been reported in studies emerging from other LMICs such as Ethiopia and Vietnam.89,90 Gender-related socioeconomic and structural inequalities may explain these findings. For instance, socioeconomic status (which, in LMICs particularly, is much likelier to be lower in women than in men) has been more strongly associated with health-related quality of life than disease factors. 91 Relatedly, women living in LMICs consistently report worse quality of life than men in the same countries,92–94 and there are strong and consistent sex differences in the expression of somatic complaints and psychological illness. 90
Our first a priori hypothesis, that WWH will perform more poorly than MWH in the cognitive domains of motor skills and visuospatial learning and memory, was not supported. Analyses (both those unadjusted and adjusted for covariates) detected no significant between-sex differences, both globally and in any specific domain of cognitive functioning. The result with regard to global cognitive performance is consistent with that reported in previous systematic reviews and meta-analyses.17,18
However, the nonsignificant findings in the domains of motor skills and visuospatial learning and memory contrast with the results reported by the most recent meta-analysis summarizing this literature. 18 However, the effect sizes detected by the meta-analysis were relatively small and might be explained by between-group differences in depression severity and educational level.
Other individual studies have reported sex differences in specific cognitive domains such as information processing speed, audioverbal learning and memory, and executive functioning.8,10 Notably, however, the samples used in those studies differ in several ways from the sample described here. For instance, whereas Maki et al 8 analyzed data from the Women's Interagency HIV Study (WIHS) and the Multicenter AIDS Cohort Study (MACS) based in the United States, we collected data from socioeconomically disadvantaged South African PWH with comorbid MDD. Hence, we conclude that sex differences in PWH cognitive performance do not appear universally, and that when they do they are likely explained by sociodemographic and/or psychosocial characteristics that vary significantly across the samples of WWH and MWH within the individual study.
Our second a priori hypothesis was that sociodemographic, psychosocial, and psychiatric (eg, depression severity) factors will be associated with cognitive performance in both WWH and MWH. This prediction was partially supported. Our analyses detected no significant influence of depression severity on global cognitive performance in either WWH or MWH. This result is inconsistent with a report from a recent systematic review, which observed a significant relationship between depression and cognitive outcomes. 34 For the most part, the larger depression literature includes depressed and nondepressed individuals; therefore, it is possible that our analyses did not detect a significant relationship because the current sample included only those with diagnosed MDD. It is also possible that our analyses did not detect such a relationship because depression affects domain-specific, but not global, cognitive performance and we did not examine whether depression affected the individual domain scores. This speculation is supported by studies observing significant effects of depression on performance in the specific domains of motor skills, processing speed, attention/working memory, learning and memory, and executive functioning.32–35,95
Consistent with our a priori prediction, fewer years of education, the presence of illiteracy, and greater food insecurity were independently associated with lower cognitive performance in WWH. Multivariable analyses further established that, in the sample of WWH, the variables that best explained global cognitive performance were level of education and food insecurity. These findings provide preliminary evidence that food security, educational attainment, and literacy may be protective against cognitive impairment for WWH who are also managing depression.
Lower education and illiteracy are both well-established predictors of cognitive performance in the general population.36,37 In the HIV literature, the WIHS (one of the largest studies of WWH neuropsychology) found that years of education and reading level were strong predictors of cognitive performance; in fact, reading level was the strongest such predictor, exceeding even the influence of HIV disease variables. 39 A South African study found similar results: educational attainment and cognitive reserve were the only factors consistently associated with cognitive performance in PWH from socioeconomically disadvantaged settings. 96
Food insecurity is, similarly, well-established as a significant correlate of poor cognitive performance, especially among older adults. This association has been described in both high-income countries, such as the United States 97 and LMICs, such as South Africa. 48
Several different mechanisms might explain the association between food insecurity and cognitive performance. One possible mechanism is that insufficient intake of vitamins and nutrients directly impairs cognitive functioning.98,99 Interestingly, however, when Gao et al 97 controlled for plasma homocysteine (a biomarker of the intake of B vitamins) and for the intake of fruit and vegetables, they found no attenuation of the relationship between self-reported food insecurity and objectively measured cognitive performance. One interpretation of this result is that food insecurity may be a proxy for socioeconomic disadvantage, and that therefore the relationship being scrutinized in such studies is actually the well-established association between lower levels of socioeconomic status and lower performance on cognitive tests.100,101 This interpretation would certainly make sense in the context of the current study: In South Africa, poverty is the main driver of food insecurity. 40
Few published studies have investigated the relationship between food insecurity and cognitive performance in PWH. Two studies with majority MWH samples from the United States both found that food insecurity was associated with worse global cognitive performance.49,50
It may be regarded as surprising that our analyses detected no strong influence of HIV disease factors in predicting cognitive performance. Given that many previous studies have reported such associations,102–107 we might have expected to find the same, especially in a sample with poorly controlled viral replication. However, our results are consistent with those from the WIHS, which that found that reading level, age, years of education, and income were all more strongly associated with cognitive performance than HIV status. 39
The results of this study should be interpreted with the following limitations in mind. First, many psychosocial variables that were not measured in this study (eg, socioeconomic opportunities, stress levels, and trauma history) could have influenced cognitive performance. Determining the impact of such variables on cognitive performance would have strengthened the study. Second, the sample included a relatively small number of MWH. Although the proportion of MWH to WWH is representative of the South African PWH population, 108 the small sample of MWH meant we may not have had sufficient statistical power to detect significant associations between cognitive performance and individual sociodemographic, psychosocial, HIV disease, and psychiatric predictors. For similar reasons, the nonsignificant between-group analyses should be interpreted with caution. Third, because our design dictated that all participants had to be incompletely ART adherent and diagnosed with MDD, there may not have been enough variation in HIV disease characteristics or depression severity to find associations between these variables and cognitive performance.
Although MWH might, in global terms, be underrepresented in this study, the fact that we studied a majority-female sample makes our results novel and useful because in this research field WWH tend to be underrepresented and understudied.17,109 A peculiarity of this field is that most HIV studies are conducted in high-income countries (such as the United States and the United Kingdom) and include majority-male samples, notwithstanding the fact that WWH (most of whom live in sub-Saharan Africa) comprise the majority of PWH globally. 51
Summary and Conclusion
We found, in a sample of South African PWH from socioeconomically disadvantaged settings, with incomplete antiretroviral adherence and comorbid MDD, that there were no significant differences in cognitive performance between WWH and MWH. This result held even after analyses were adjusted for potentially confounding variables (ie, education level, viral load, CD4 count, health-related quality of life, and high-risk alcohol use), and it remained stable whether considering global cognitive functioning or performance within discrete cognitive domains. We therefore conclude that sex differences in cognitive performance do not exist in all study populations of PWH, and that where they are observed they may be accounted for by variation in sociodemographic and psychosocial characteristics (representing broader issues of population-based gender inequality) within individual samples of WWH and MWH. These characteristics and their variation are not routinely measured in HIV research studies.
Our analyses also suggested that psychosocial factors (eg, level of education and food insecurity) best explained global cognitive performance in this group of WWH, exceeding the influence of mooted predictors such as depression severity and HIV disease variables. We detected no significant influence of sociodemographic, psychosocial, medical, or psychiatric variables on cognitive performance in this group of MWH, although this result must be interpreted with caution given the small number of men in our sample.
In conclusion, we recommend that future studies not simply focus on investigating sex differences in cognitive performance in PWH. Instead, they should ensure WWH are adequately represented in their research samples and that issues of gender inequality are addressed not only in their interpretation but in their design. Regarding recommendations for care and treatment of WWH, the results suggest that educational attainment and literacy may protect against cognitive impairment for WWH managing depression and interventions aimed at food insecurity in the context of support for HIV treatment may be beneficial.
Footnotes
Acknowledgments
We would like to acknowledge the research assistants, especially the neuropsychology technician, Teboho Linda, and the study participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute of Mental Health or the National Institutes of Health under grant 5R01MH103770-S1. Some additional support came from 1P30MH116867 for investigator support. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health or the National Institutes of Health.