
Abstract
HIV-associated neurocognitive disorders (HANDs) are common, often go undetected, and can impact treatment outcomes. There is limited evidence on how to perform routine cognitive screening in HIV clinical settings. To address this, 44 HIV-positive males were recruited from a Veteran Affairs Infectious Disease clinic and completed the Montreal Cognitive Assessment (MoCA), International HIV Dementia Scale (IHDS), and Depression Anxiety and Stress Scale-21. In all, 50% scored below the MoCA cutoff and 36% scored below the IHDS cutoff. Current CD4 was the strongest predictor of an abnormal MoCA score (P = .007, 95% confidence interval [CI]: 0.987-0.998) and elevated depression was the second strongest predictor (P = .008, CI: 1.043-1.326). Combination antiviral therapy use and age were not significant predictors in this model. The MoCA appeared to be a reasonable screening tool to detect cognitive impairment in HIV-positive patients, and although it is not sufficient to diagnose HAND, it has the potential to provide meaningful clinical data.
Introduction
HIV-associated neurocognitive disorders (HANDs) are common. Even in the era of effective combination antiviral therapy (cART), 30% to 50% of HIV-positive patients have been found to have some degree of mild–moderate cognitive impairment that is often undetected and can interfere with treatment adherence and other health outcomes. 1 –5 Further complicating this issue, many people living with HIV are aging. In 2011, there were over 25 000 HIV-positive veterans receiving care, 66% of whom were between the ages of 50 and 69. 6 There are many other comorbid factors that can contribute to cognitive impairment in this population, including hepatitis C coinfection, substance use (particularly methamphetamine abuse), depression, and anxiety. 7 –10
Using the Frascati criteria, HAND is defined as 1 of the 3 conditions: asymptomatic neurocognitive impairment in which neuropsychological test performance is at least 1 standard deviation (SD) below normative data in at least 2 domains with intact daily functioning; mild neurocognitive disorder is characterized by similar neuropsychological testing impairment, with impaired daily functioning; and HIV-associated dementia is characterized by severe deficits in at least 2 cognitive domains (typically ≥2 SDs below normative data) and more severe daily functioning impairment. Given the implications, screening is recommended to identify patients experiencing HAND. 2,11 Routine screening could elucidate functional impairment in patients and arm clinicians with the necessary knowledge to manage their patients’ limitations. However, there is insufficient evidence to guide when and how to screen. 12,13 Although brief batteries have been proposed and certain tests highlighted, 2,3,12,14,15 there remains a need for brief screeners that are sensitive, easily accessible, and can be administered by clinical staff across a range of disciplines and settings.
The Montreal Cognitive Assessment (MoCA) is a brief screening measure that has been shown to have high sensitivity and specificity in detecting mild cognitive impairment (MCI), with a 90% sensitivity rate for detection in an elderly population, compared to 18% detection of MCI with the Mini-Mental Status Examination (MMSE). 16 The MoCA and MMSE yield a maximum score of 30, with scores of ≥26 and ≥24, respectively, suggestive of normal cognition. 16,17 Among HIV-positive patients older than age 60, the MoCA identified patients with HAND at a sensitivity of 72% and specificity of 67%, using a cutoff of 25, suggestive of moderate performance characteristics. 12 In contrast, 74% of those with HAND obtained an MMSE score of ≥28 and paralleling earlier findings, the authors concluded that the MMSE is not a sensitive tool for detecting HAND. 12,18 –20 The authors recommended additional screening tools be employed to improve the use of the MoCA. 12 In a Korean sample with a mean age of 45.12, the MoCA had a specificity of 73% and sensitivity of 53% using a cutoff of ≤25 and using a cutoff of ≤10, the International HIV Dementia Scale (IHDS) had a specificity of 61% and sensitivity of 73%. 21 The MoCA has been validated for use with older adults and compared to neuropsychological batteries. 22,23 Valcour 3 reviewed existing literature on screening for cognitive impairment in HIV-positive patients and suggested that the MoCA shows promise but as of yet has insufficient data to support its use without additional measures. Koski et al 24 also found the MoCA was an adequately sensitive measure to assess cognitive impairment in HIV among a wide range of adults (mean age of 47.3), although it had reduced precision in detecting subtle declines in higher functioning individuals.
To address these gaps in the literature, the objectives of this pilot study were to (1) determine the proportion of patients who screened below the cutoff on the MoCA and the IHDS and (2) examine the relationship between performance on the MoCA, IHDS, and factors that might predict poor performance such as demographics, current and historical substance use, current viral load (VL) and CD4 count, CD4 nadir, current medication regimen, and mood (depression, anxiety, and stress).
Methods
Forty-four male, HIV-positive veterans, aged 40 or older, were recruited from an Infectious Disease clinic in an urban, VA Medical Center. Participants provided written, informed consent, and completed demographic questionnaires and measures evaluating substance use, mood symptoms, and cognitive impairment. The battery consisted of the MoCA 16 ; the IHDS, which has been validated for detection of HAND in an HIV-positive population 25 ; and the Depression Anxiety and Stress Scale-21 (DASS-21), a 21-item measure with subscales for depression, anxiety, and stress that demonstrates good reliability and validity. 26 Patients with active psychosis, acute intoxication at the time of consent, organic brain syndrome (HAND, alcoholic or hepatic encephalopathy, or multi-infarct dementia; as determined by an existing medical diagnosis), or previous neuropsychological testing within the past 2 years were excluded from the study. Participants were included in the study if their most recent laboratory results (HIV serology, CD4, plasma HIV VL, and CD4 nadir) were available by self-report and/or chart verification. A total of 118 patients were referred for this study and 39 declined to participate. In all, 5 were excluded due to recent neuropsychological testing and 2 were excluded due to a diagnosis of dementia. A total of 47 patients consented to participate and 3 were excluded from analysis due to incomplete screening data. If during the study participants scored below the accepted cutoff on the MoCA (26) and/or IHDS (10), they were referred for further evaluation and appropriate treatment. All analyses were conducted using SPSS 22.0. This study was approved by the Human Subjects Committee at the University of California, San Francisco.
Results
The mean age of this sample was 58.8 (SD 8.43) and 61.4% were caucasian, 20.5% were black, and 13.6% were hispanic (Table 1). Participants had a mean of 17.9 (SD 8.3) years since their HIV diagnosis and 93.2% were taking cART. Fifty-nine percent of patients had a history of a psychiatric disorder. There were no significant differences in age, education, income, psychiatric diagnosis, HIV clinical variables, and hepatitis C virus (HCV) coinfection between participants who scored above the MoCA cutoff from those who scored below (Table 1). The MoCA score had a strong Spearman rank correlation with the IHDS of 0.69.
Demographics by MoCA Score.

Abbreviations: cART, combination antiviral therapy; HCV+, hepatitis C virus seropositive; MoCA, Montreal Cognitive Assessment; SD, standard deviation; χ2, chi-square.
Direct logistic regression was conducted to evaluate the impact of CD4, age, use of cART, and depression on the likelihood of receiving a score below the cutoff on the MoCA. These variables were selected as important factors that can influence neurocognitive outcomes in HIV. Due to our sample size, the regression model was limited to inclusion of 4 variables. The overall model was statistically significant, χ2 (4, N = 44) = 23.020, P < .0005, indicating that it was able to distinguish MoCA scores above (≥26) and below (< 26) the cutoff (Table 2). This 4-factor model explained between 40.7% (Cox and Snell R 2) and 54.3% (Nagelkerke R 2) of the variance in MoCA score and correctly classified 77.3% of the cases.
Results by MoCA Score.
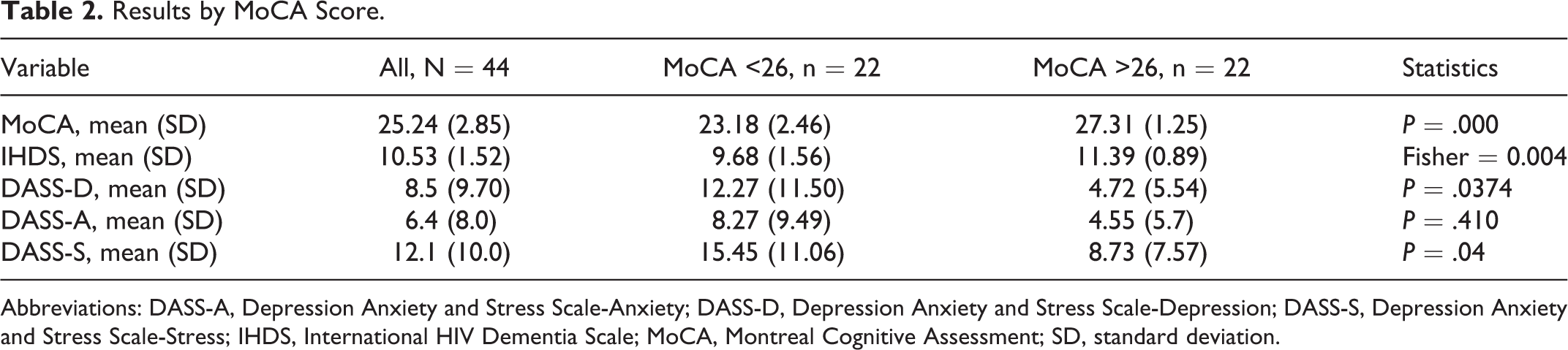
Abbreviations: DASS-A, Depression Anxiety and Stress Scale-Anxiety; DASS-D, Depression Anxiety and Stress Scale-Depression; DASS-S, Depression Anxiety and Stress Scale-Stress; IHDS, International HIV Dementia Scale; MoCA, Montreal Cognitive Assessment; SD, standard deviation.
As shown in Table 3, current CD4 and depression made a unique, statistically significant contribution to the model. The strongest predictor of a lower MoCA score was current CD4 count (odds ratio [OR] = 0.992; P = .007, 95% confidence interval [CI]: 0.987-0.998), even after controlling for age, cART, race/ethnicity, and depression score. The second strongest predictor of a lower MoCA was the DASS-21 depression score (OR = 1.176; P = .008, CI: 1.043-1.326), after controlling for current CD4, age, and cART. Age, race/ethnicity, and cART use were not significant predictors in this model.
Logistic Regression of the Likelihood of a MoCA Score <26.

Abbreviations: cART, antiretrovirol; CI, confidence interval; DASS-D, Depression Anxiety and Stress Scale-Depression; MoCA, Montreal Cognitive Assessment; SE, standard error.
Discussion
The primary goals of this study were to (1) determine the proportion of treatment-seeking, HIV-positive patients older than the age of 40 who screened below the MoCA and IHDS cutoffs for impairment and (2) examine the predictive factors that differentiated those patients who scored below the cutoff on the MoCA from those who scored in the nonimpaired range. Of the 44 patients, 50% (22) scored below the cutoff of 26 on the MoCA and 36% (16) scored below the IHDS cutoff of 10. Our statistical model was able to distinguish between these groups and accurately predicted performance in 77.3% of cases. Current CD4 count and DASS-21 depression score significantly differentiated between these groups.
Nearly half of the participants scored below the standard cutoff of the MoCA and over a third scored below the standard cutoff on the IHDS, which mirrors results from other studies 1,2 and points to the high burden of impairment in this patient population. Considering current CD4 count and depression may prove useful in determining who may benefit from additional cognitive screening and further assessment of psychiatric concerns.
There is current discussion in the field about HAND diagnostic criteria, effective assessment strategies, treatment implications, and the role of screening for cognitive impairment. 1,2,9,11,27,28 Given the lack of a gold standard, high rates of false positives, and the broad definition of cognitive impairment, 29 the risks of screening must be balanced with the clinical benefit. Another consideration for the implementation of screening is the availability of follow-up, which for mild or moderate levels of impairment should include providing cognitive rehabilitation services and appropriate medical and mental health follow-up, as indicated. Further examination of appropriate screening measures for reliably detecting HAND is imperative.
This study had several limitations. Given the small sample size, we were underpowered to detect certain potential and known correlates of cognitive impairment, such as CD4 nadir, cART adherence, and the impact of hepatitis C coinfection (see Table 1). However, CD4 nadir and HCV coinfection did not significantly differ between those who scored above or below the MoCA cutoff.
Although the presence of a psychiatric disorder did not significantly differentiate those who scored above or below the MoCA cutoff, low scorers had significantly higher depression and stress scores. This may have negatively impacted their performance on the battery, contributing to a lower score, as depression in elders is related to executive functioning deficits, even after the depressive symptoms have abated. 30,31 Although we obtained data on psychiatric history, specific diagnoses were unavailable. Very few of the patients who screened below the MoCA and IHDS cutoffs agreed to further neuropsychological testing; thus we were unable to determine the rate of false positivity. To obtain the most representative data of our clinic population and HIV clinics across the VA and allow comparison to the CNS HIV Anti-Retroviral Therapy Effects Research (CHARTER) study, 1 we set the lower age limit to 40 years.
Despite these limitations, the MoCA appears to be a reasonable screening tool for HIV-positive patients; however, its utility is heightened by the addition of other cognitive and psychiatric measures. The MoCA is feasible for use by nonphysician providers and paraprofessionals and is available in the public domain. It would be beneficial for future studies to compare multiple brief screening tools to a full neuropsychological test battery to optimize a screening tool that can reliably detect HAND and discriminate between HAND and normal cognition.
Footnotes
Acknowledgments
The authors wish to express their appreciation to the research participants and colleagues at the SF VAMC ID clinic for their support and cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Veterans Affairs (5101BX001048) and NIH (R01 NS051132) for research funding.