
Abstract
Keywords
HIV2 is localized in West Africa and its monitoring requires access to technology that is inaccessible to developing countries and the subject is poorly studied and attention and efforts given the epidemiology are focused on HIV1, so interpenetration in different populations is not to be overlooked.
Improving medical care of HIV2 patients in resource-limited countries.
HIV2 is becoming globalized and careful clinical and immunological monitoring of patients is saving HIV2 infected patients and we contribute to the availability of data regarding HIV2
Introduction
The Human Immunodeficiency Virus (HIV) type 2 was discovered in 1986 in West Africa [1]. It is endemic in the following countries: Guinea Bissau, Gambia, Senegal, Cape Verde, Ivory Coast, Burkina Faso, Mali, Sierra Leone, Nigeria. It is also found in countries with socio- economic relations with this region of Africa. An estimated 1 to 2 million people were infected with HIV2, including people with both HIV1 and HIV2 [2]. Its epicenter in West Africa is Guinea Bissau, where prevalence in the general population ranged between 6% and 10%. Recent studies show a decline in prevalence with a probable extinction of the HIV2 epidemic in 2068 [3,4].
Compared to HIV1 infection, the natural history of HIV2 infection is characterized by a much longer asymptomatic stage, a significantly lower plasma viral load, a slower decline in CD4 counts, an AIDS mortality lower rate [5–9], lower rates of mother-to-child transmission, genital excretion and sexual transmission [10,11]. Despite this, a significant proportion of people infected with HIV2 progress to AIDS and have the same opportunistic infections as HIV1 infection, with some differences [7,12].
In Burkina Faso, in 2017, the prevalence of HIV infection was estimated at 0.8% in the general population among people aged 15-49 years, with HIV1 infection predominating [13]. Sentinel surveillance in 2014 showed an HIV2 prevalence of 2% [13]. This no less significant prevalence makes HIV2 a matter of concern in Burkina Faso, particularly for the monitoring and management of these infected patients.
In our context, few studies have been done on HIV2 in relation to HIV1. Among them, a study by Harries et al found a prevalence of 2.5% and 3.6% respectively for HIV2 and HIV1 + 2 co-infection [14]. We initiated this observational study to evaluate the results of long-term follow-up of patients living with HIV2 in order to optimize their management.
Methods
This study took place at the day hospital /HIV care department of Internal Medecine Unit of university hospital Yalgado Ouedraogo, Ouagadougou. The study involved patients aged 18 years and older, followed for HIV2 or HIV2 + 1 infection screened according to the national algorithm: Determine Test© HIV-1/2 (Abbott Laboratories, Abbott Park, IL, USA) and the SD Bioline©HIV-1/2 3.0 test (Standard Diagnostics, Kyonggi-do,SouthKorea).
Screened patients were started on antiretrovirals (ARVs) according to national recommendations with an initial CD4 cell count test. The prescribed treatment regimen consisted of a ritonavir-boosted protease inhibitor (PI/r) and two nucleoside reverse transcriptase inhibitors (2NRTIs) as the first-line regimen and three nucleoside reverse transcriptase inhibitors (3NRTIs) as the second-line regimen.
The efficacy of the treatment was judged clinically and immunologically by measuring CD4 lymphocyte counts. The viral load assay was unavailable. In the case of HIV2 + 1 co-infection, the HIV1 viral load was carried out every six months or at least once a year.
This was a cross-sectional study with a descriptive and analytical focus from first January 2011 to 31 December 2015. For each patient, sociodemographic (age, sex, occupation), clinical (history of opportunistic infections and co-morbidities, WHO classification at inclusion in the active file, weight), biological (TCD4 lymphocyte count, hemoglobin level, white blood cell count, total lymphocyte count) and other data were collected, creatinine, blood glucose, cholesterol, triglyceridemia, transaminases (ALT), HIV1 viral load (for HIV2 + 1 co-infected patients), therapeutic (the different combinations of ARVs prescribed, changes and reasons), progress since enrollment (number of patients who died, number of patients lost to follow-up and transferred). The non-inclusion criteria were the patient who came for one -time assessment.
The data were extracted from the electronic database (ESOPE) and the hard files (paper) and collected using a collection sheet and analyzed using the Epi info software version 7.2.3.6. Statistical analysis of the qualitative variables was conducted using Fisher and Chi2 tests. Quantitative variables were analyzed by Student's t-test when conditions were met. The value of p < 0.05 was used as the significance level for differences and associations. Confidentiality and anonymity were ensured and no names or personal information that could identify a patient was mentioned on the collection form.
Ethical Approval and Informed Constent
Our study did not require an ethical board approval. We just required a statement for data use. Therefore, the data has been extracted anonymously.
Results
Epidemiological Aspects
In 2011, the proportion of patients infected with HIV2 and HIV2 + 1 was 4.3% for an active queue of 2780, with 48 (1.7%) patients infected with HIV2 and 67 (2.4%) patients co-infected with HIV-2 + 1 respectively. The sex ratio (male/female) was 0.53 (see Figure 1).

Flow chart of patients with HIV2 or HIV2 + 1 selected for the study.
The mean age was 50.3 ± 8.5 years and the age range of 50-59 years was the most represented. Patients over 50 years of age were the most numerous in the HIV2 group (70.8%). The circumstance of testing for HIV2 infection or HIV2 + 1 co-infection was clinical suspicion in 71.3% of cases.
Clinical and Biological Aspects
Weight loss, fever and diarrhea were the most frequently observed reasons for consultations (see Table 1).
Socio-Demographic, Clinical and Biological Characteristics of Patients Infected with HIV2 and HIV2 + 1 (N = 115).

*Hepatic abscess (1 case), cutaneous leishmaniasis (1 case), anal abscess (1 case).
Clinically, 40.9% and 36.5% of patients were classified as WHO stage 2 and stage 3, respectively. The number of HIV2 + 1 co-infected patients classified as stage 3 (n = 28) was double that of HIV-2 mono-infected patients (n = 14). Oral candidiasis (11.3%) and shingles (8.3%) were the main opportunistic infections found in patients. In our study, no cases of tuberculosis were observed
Therapeutic Aspects
The antiretroviral (ARV) combination therapies that were initially prescribed are detailed in the following table (see Table 2).
Répartition des Patients par Régime Thérapeutique ARV à L’initiation (N = 115).
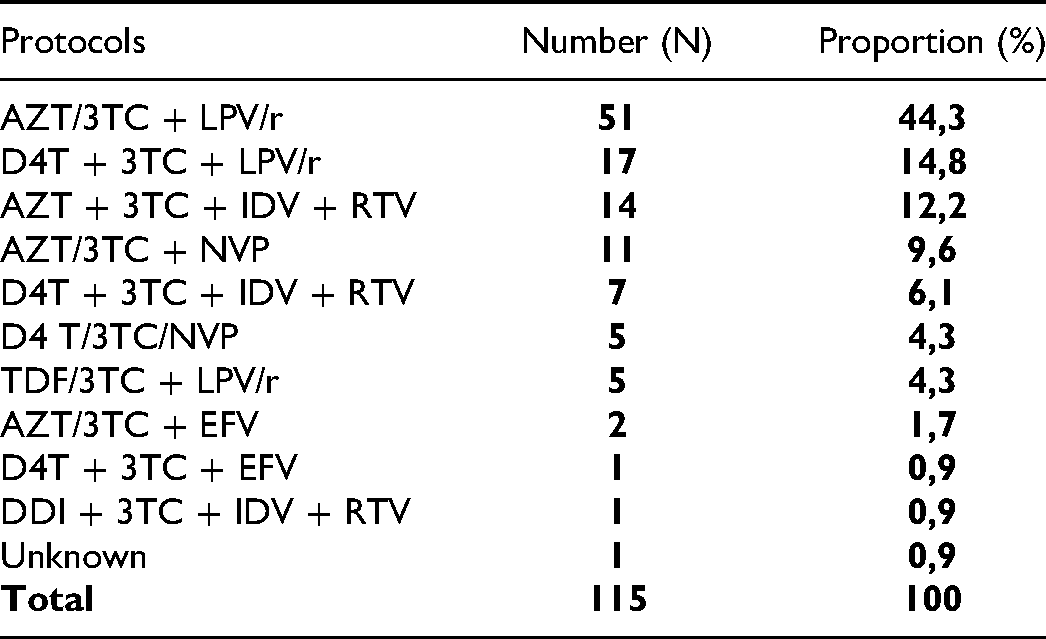
The association 2INTI + LPV/r was the most represented with 73 prescriptions (63.5%). We found 19 (16.5%) prescriptions that did not comply with the standards and protocols in force. These were: the association 2INTI + NVP or 2INTI + EFV. It was observed in 11 co-infected HIV2 + 1 patients and eight, HIV2-infected patients.
Evolutionary Aspects
The mean follow-up time for patients on treatment was 7.24 years; 95% CI [4.54-9.94] with extremes of 4 years and 13 years.
The average weight gain increased from 3 kg in 2011 to 7.3 kg in 2015.
This Figure (see Figure 2) highlights the evolution of the average weight of patients monitored from 2011 to 2015.

Progressive curve of mean weight in patients infected with HIV-2 and HIV-2 + 1 followed from 2011 to 2015.
Immunological Evolution
The annual mean CD4 lymphocyte evolution curve of patients on ARV treatment was increasing over the years from 2011 to 2015 (Figure 3).

Trend of mean CD4 cells count of patients followed from 2010 to 2015.
The average gain in TCD4 lymphocytes from baseline was: + 236; + 290; + 306; + 360 and + 364 cells/mm3 in 2011, 2012, 2013, 2014 and 2015 respectively.
The following table (Table 3) presents the results of comparing the averages of the initial CD4 count and the 2015 CD4 count.
Comparison of CD4 Count Averages by Patient (n = 75) Type from 2011 to 2015.

The variation in CD4 counts was important in both patient groups and the difference was statistically significant (p < 0.000). Patients’ immune status improved significantly during the follow-up period.
The proportion of highly immunocompromised patients with a TCD4 lymphocyte level < 200 cells/mm3 decreased from 59.0% at initiation to 6.7% in 2015; while the proportion of patients with alevel greater than 500 cells/mm3 increased: 33.7% versus 58.7%). Table 4 describes the distribution of patients according to their annual gain of TCD4 lymphocytes based on the year of follow-up.
Classification of Patients Infected with HIV2 and HIV2 + 1 According to the Level of TCD4 Lymphocytes Monitored from 2011 to 2015.

Therapeutic Evolution
During the study period, 108 types of therapeutic regimen changes for various reasons were observed (see Table 5). The new protocols consisted of the combination AZT or TDF or ABC + 3TC + LPV/r. Only one patient received the combination with raltegravir (RAL).
Distribution of Patients by Reason for Change in Therapeutic Regimen.
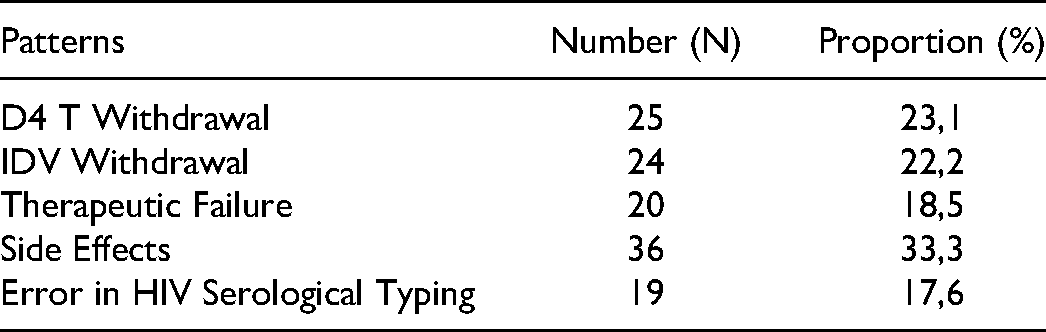
Adverse reactions were reported in 36 patients, represented in order of frequency by digestive disorders (n = 12; 35.3%), skin reactions (n = 8; 23.5%), neuropathies (n = 8; 23.5%), anemia (n = 3; 8.8%), one case of lipodystrophy, one case of hepatic cytolysis and one case of hyperglycemia.
Patient outcomes at the end of the study period are described in the following table (see Table 6).
Distribution of Infected Patients According to Treatment Outcome.

The total number of patients lost to follow-up increased during the follow-up. Intention to treat the death rate by years of follow-up was 13.9% (n = 16); 6.1% (n = 07); 22.6% (n = 26); 19.1% (n = 22); 32.7% (n = 37). The retention rate at grade 5 was about 70%.
Discussion
The limits of this study were the low number of participants, the lack of CD4 count for all and unavailabilty of viral load measure. In our study, HIV2 + 1 co-infection was superior to HIV2 mono infection. Harries et al [14] make the same observation According to the literature, the prevalence of HIV2 was higher than HIV2 + 1 [12,15,16]. Is the higher proportion of HIV2 + 1 co-infection related to diagnostic errors as reported in a study conducted in Dakar that showed that the majority of patients declared co-infected were mono-infected with HIV1 or HIV2 [17].
Housewives with low socioeconomic status were more at risk. These observations were also made during the study by Diouf et al in Senegal [5].
The most represented age group was 50-59 years old with 42%. However, the average age of patients varies according to the type of HIV. Thus, co-infected patients were younger with a mean age of 47.1 years; type 2 carriers exclusively had a mean age of 53.6 years (p < 0.002). This trend is observed by Ba et al, who found 49 years of average age in Senegal [18] and Peterson et al in the Gambia [19]. Indeed, the long clinical latency period of HIV2 infection favors late detection and entry into the care circuit.
This delay in diagnosis is reflected in the profound immunosuppression presented by patients at screening. Thus 59% of our patients had an average CD4 count below 200 cells/mm3 and 38.2% had WHO clinical stage 3 and 4. Authors in sub-Saharan Africa corroborate this fact [15,19].
In our series the first three reasons for consultation were weight loss, fever and diarrhea. These data were also found in other studies in the same order by Diouf et al Sørensen et al [12] found, in descending order, weight loss, fever, oral candidiasis and diarrhea. ARV treatment protocols without protease inhibitors (PIs) were found in 16.5% of patients. It was 33.7% in the IedEA-West Africa cohort [15]. Harries et al [14] in Burkina Faso observed 28.6% in HIV2 and 27.3% in HIV2 + 1, respectively. Indeed, limited access to protease inhibitors (PIs), the performance of discriminatory tests leading to diagnostic errors, stock-outs of PIs, inattention of prescribers, inadequate supervision, insufficient training and a breakdown of discriminatory tests could be causes of inappropriate prescriptions. Sarfo et al in Ghana [20] also found inappropriate prescribing of NNRTIs in 5.9% of HIV2 patients and 21.1% of HIV1 + 2 patients.
The evolution under medical supervision showed an improvement in the clinical condition of the patients translated by an increase in average weight from 61.4 kg to 65.7 kg ARV after five years. The overall mortality rate was 4.3%. The mortality rate varies according to the studies: 11.8% for Petereson et al [19], in less than two years of follow-up, to 15.4% for Harries et al [14].
In terms of intention to treat, our results are comparable to those found by some West African authors [7,8,21,22]. A meta-analysis by Prince et al showed that the mortality rate of HIV2 mono-infected patients was lower than that of HIV-2 + 1 co-infected patients [21].
Treatment efficacy was judged on both immunological (CD4 count) and clinical criteria due to the unavailability of the HIV2 viral load measurement technique. The average CD4 gain was + 331 cells/mm3. Immune restoration varies according to the authors: + 105 cells/mm3 in 12 months for Balestre et al in the IedEA-WA cohort, Wittkop et al in a European multi cohort with 12 months follow-up [23,24], + 405 cells/mm3 for Requena et al in Spain [25]. At the fifth year of follow-up the proportion of patients with CD4 + counts below 200 cells/mm3 was reduced to 6.7% compared to 16.3% initially.
ARV treatment was fairly well tolerated by patients, however, this work reveals a retention rate in the continuum of care that decreased to 69% in five years of follow-up, significantly higher than the 65% rate that was found across the different cohorts in sub-Saharan Africa [26].
The proportion of patients lost to follow-up was 24.3% at year five of follow-up. It was 25.7% for Tchounga et al, who found at 24 months of follow-up [27], 18.2% for Carriquiry et al [28] in Latin America and the Caribbean after five years of follow-up regardless of serotype. In Côte d'Ivoire after a 4-year follow-up, 49% of patients were lost to follow-up by Auld et al [29]. Self-transfer to other centers because we did not have unique identifier code, travel to other country, missed information that the therapy is longlife, residence outside or far from Ouagadougou or death would be the reasons founded. According to the literature, about 40% of those lost to follow-up were deceased patients [26].
Conclusion
Patients infected with HIV2 and HIV2 + 1 entered care late, but had a fairly good clinical and immunological response. In order to optimize the management of these patients, it would be useful to make HIV2 viral load available. More than half of the patients remained in the continuum of care after five years of follow-up, however, a study looking at the reasons for loss to follow-up would be beneficial.
Footnotes
Abreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.