
Abstract
Background:
We aimed to study the factors associated with clinical forms of lipoatrophy in patients receiving highly active antiretroviral therapy (HAART) in Yalgado Ouédraogo Teaching Hospital, Ouagadougou, Burkina Faso.
Methods:
This cross-sectional review from March 10 to November 10, 2011, included a nonprobability sample of HIV-infected adults receiving antiretroviral (ARV) medications for at least 6 months and monitored in the internal medicine department. The diagnosis of lipoatrophy was clinical.
Results:
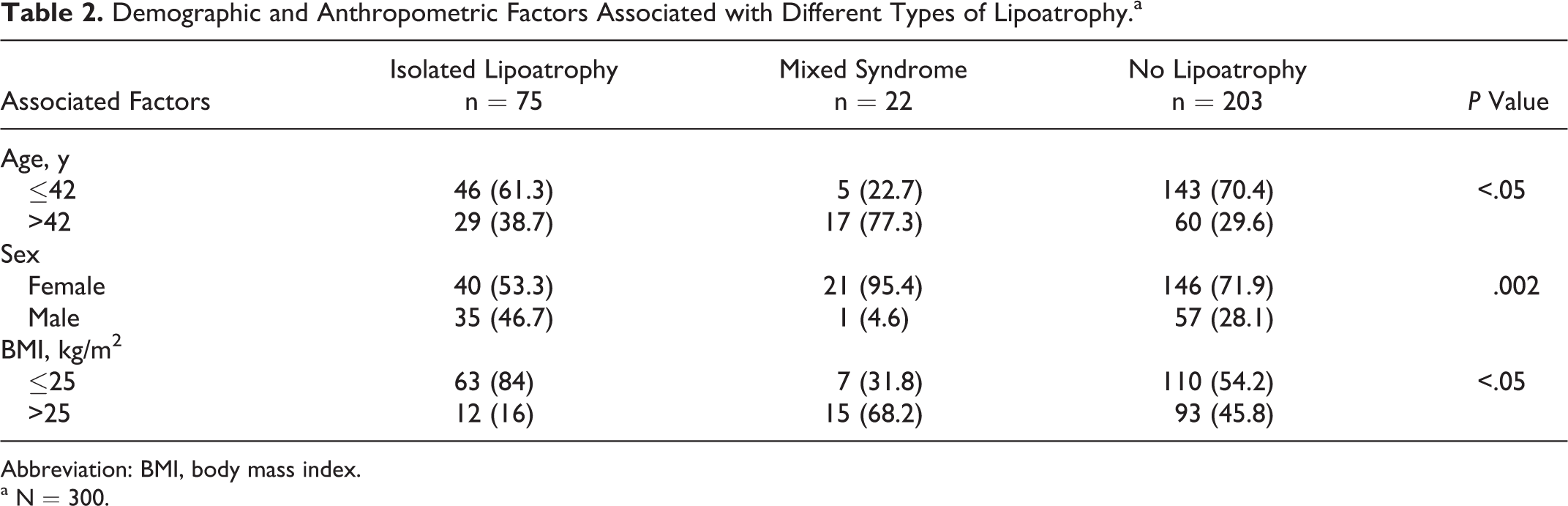
Three hundred patients were included. The sex ratio was 0.4 and the mean age was 42.1 ± 8.5 years. The mean duration of HAART was 73.2 ± 30.9 months. In all, 97 (32.3%) patients had lipoatrophy: 75 (25%) isolated and 22 (7.3%) mixed syndrome. Facial lipoatrophy was frequent (61.8%). Isolated lipoatrophy was associated with male sex (P = .002) and body mass index ≤25 (P < .05). Mixed syndrome was associated with female sex (P = .002), age >42 years (P < .05), physical activity (P = .003), smoking (P = .001), stavudine (d4T; P = .0001), or protease inhibitors (P = .01).
Conclusion:
Prevention of lipoatrophy associated with HAART requires the exclusion of modifiable risk factors that we identified.
Keywords
Introduction
Lipodystrophy is a disorder in fat distribution, which may occur with highly active antiretroviral therapy (HAART) during the management of HIV/AIDS. 1,2 It consists of 2 entities that can appear together: lipoatrophy and lipohypertrophy. 3 These phenotypes arise from different mechanisms so that their study in a single entity seems inappropriate. 4 Lipoatrophy is certainly the most stigmatizing side effect of antiretroviral (ARV) medications and is associated with impaired quality of life, treatment noncompliance, and other deleterious metabolic comorbidities. 1–3,5,6 Because of the characteristics of HAART regimens commonly used in developing countries, including Burkina Faso, this study was undertaken to determine the prevalence of different forms of lipoatrophy as well as the associated factors in a cohort of HIV-infected patients receiving ARV medications in Ouagadougou. The study will help to consider preventive measures against these disorders in light of the associated factors.
Materials and Methods
This was a cross-sectional study conducted from March 10 to November 10, 2011, in Yalgado Ouédraogo Teaching Hospital (CHUYO), Ouagadougou, Burkina Faso. The study included HIV-infected adults (18 years or older) receiving ARV medications for at least 6 months and who were followed in the day care hospital of the internal medicine department and had consented to participate in the study. Those with edema and/or a Karnofsky performance status <70% were not included. The sample was accidental and nonprobabilistic. Isolated lipoatrophy was defined as a loss of subcutaneous fat in the face, buttocks, and upper and/or lower limbs. Mixed syndrome was defined as the coexistence of lipoatrophy and lipohypertrophy with fat accumulation in the abdominal, neck, breast, and/or pubic regions. The diagnosis was clinical and determined by the same investigator in accordance with the patient’s opinion. Demographic, anthropometric, clinical, biological, and therapeutic variables were collected during the medical consultation and from the patients’ clinical records. Analysis was performed using chi-square or Fisher (when size <5) test to compare qualitative variables. A P value of less than .05 was considered statistically significant.
Results
Epidemiological and Clinical Features of Lipoatrophy
Three hundred patients were studied; the sex ratio was 0.4 and mean age was 42.1 ± 8.5 years. The mean duration of HAART was 73.2 ± 30.9 months. The main HAART regimens noted were zidovudine (ZDV)/lamivudine (3TC)/nevirapine (NVP) (32.3%); stavudine (d4T)/3TC/NVP (26.3%), and ZDV/3TC/efavirenz (EFV; 14.3%). Of these patients, 97 (32.3%) had lipoatrophy, including 75 (25%) isolated lipoatrophy and 22 (7.3%) mixed syndrome. Thirty-one (10.3%) patients had isolated lipohypertrophy. Table 1 shows the demographic and anthropometric features in different groups of patients.
Anthropometric and Demographic Characteristics in Different Groups of Patients.a

Abbreviation: BMI, body mass index.
a N = 300.
Lipoatrophy affected the face, lower limbs, buttocks, and upper limbs, respectively, in 60 (61.8%), 22 (22.7%), 21 (21.6%), and 10 (10.3%) patients. Forty-five (46.4%) patients had lipoatrophy with multiple localizations.
Factors Associated with Different Forms of Lipoatrophy
As factors related to lifestyle, smoking was reported by 5 (6.7%) patients who presented with lipoatrophy, 4 (18.2%) with mixed syndrome, and 4 (2%) without lipoatrophy (P = .001). The practice of physical activity was reported by 7 (9.3%) patients with isolated lipoatrophy, 3 (13.6%) with mixed syndrome, and 5 (2.5%) without lipoatrophy (P = .003).
The baseline CD4 count was lower than 200 cells/mm3 in 36 (48%) patients with isolated lipoatrophy, 7 (31.8%) with mixed syndrome, and 105 (51.7%) without lipoatrophy; P = .20. Tables 2 and 3, respectively, show the demographic and anthropometric and the therapeutic factors associated with different phenotypes of lipoatrophy.
Demographic and Anthropometric Factors Associated with Different Types of Lipoatrophy.a
Abbreviation: BMI, body mass index.
a N = 300.
Therapeutic Factors Associated with Different Types of Lipoatrophy.a

Abbreviation: HAART, highly active antiretroviral therapy.
a N = 300.
Discussion
Lipoatrophy was reported in 32.3% patients and the isolated form predominated. Lesions usually occured on the face. The factors associated with different phenotypes of lipoatrophy sometimes differed from those reported in other studies.
Unlike the data reporting the frequency of isolated lipohypertrophy 7 or mixed syndrome 8–11 during HAART, isolated lipoatrophy was reported as the most frequent anomaly in fat distribution in our patients. Precision concerning the clinical forms of lipoatrophy is often limited. Some studies reported a lower frequency of lipoatrophy: 9.8% in Rwanda, 8 13% in France, 9 and 21% in Spain, 11 while the mixed syndrome was were frequent: 19% in Rwanda, 8 27% in France, 9 and 24% in Spain. 11 Similar to our study, a Korean study 2 reported a frequency of isolated lipoatrophy of 24.3%. 2 The incidence of lipoatrophy in studies may be influenced by the variability of diagnosis criteria. Contrary to studies using specific criteria based on anthropometric 8,11 imaging or absorptiometry 7 assessment, we performed an inspection diagnosis which is likely to underestimate the frequency of anomalies in fat distribution. Compared to our findings, the reduced frequency of isolated lipoatrophy in some European cohorts could be related to the less frequent use of stavudine 9,11 as well as their short exposure to HAART 9 ; this last condition supports why in Rwanda, despite the most frequent use of stavudine, isolated lipoatrophy was less frequent. 8 Similarly, the propensity to use protease inhibitors (PIs) justifies a greater frequency of mixed forms in European cohorts. In the French study, only patients receiving regimens containing PIs were included. 9
Factors associated with lipoatrophy are sometimes different in the literature. Most studies agree that d4T is an important factor associated with lipoatrophy 2,6,9,11–13 ; despite its less frequent use (35.7%), the prevalence of lipoatrophy was higher in our cohort than the Rwanda and South Africa cohorts who were using more than 90% of HAART regimens containing d4T. This finding may be partly explained by further exposure of our patients to the regimen. This condition is often associated with the occurrence of lipoatrophy 2,6,12 and justifies the opinion to reconsider further continuation of d4T after 12 months of use. Moreover, in contrast to our finding concerning the higher frequency of mixed syndrome during the use of d4T, a French study reported an association with isolated lipoatrophy. 11 The role of PIs in the occurrence of lipoatrophy is not univocal: the French study reported an association of saquinavir (SQV) with lipoatrophy or mixed syndrome; while in our survey, lopinavir boosted with ritonavir (LPV/r) was associated with mixed syndrome. Our finding could be explained because LPV/r was the single PI used in our cohort. 11
Demographic, anthropometric, and behavioral factors associated with lipoatrophy are also variously reported. Similar to a Canadian study, 4 we found an association between female sex and mixed syndrome. Age greater than 42 years was also an associated factor. The trend to central adiposity with aging, a phenomenon more pronounced in women consecutive to hormonal influence, may promote such a phenotype. 14 Smoking and practice of physical activity were other factors associated with mixed syndrome. On the other hand, male sex and not being overweight were associated with isolated lipoatrophy as reported in Canadian 4 and Danish surveys. 12 The inverse relationship between fat tissue size and earlier visibility of lipoatrophy makes the observation of lipoatrophy phenotype easier in these conditions. 11 A Japanese study found an inverse relationship between fat tissue size and aging in men. 14 However, an association between female sex and lipoatrophy was found by other authors. 2,9
The frequency of facial lipoatrophy is consistent with most data, probably due to the reduced thickness of the fatty tissue on the face. Unfortunately, facial lipoatrophy contributes more to stigma because it is not concealable. To this end, strategies for facial fillers are recommended. These methods are unavailable in developing countries. However, according to the Antiprotéases Cohorte study, facial lipoatrophy takes second position next to the lower limbs, after 2 years of follow-up. 10
Conclusion
Lipoatrophy during HAART is not uncommon. Regardless of whether lipoatrophy appears isolated or as part of a mixed syndrome, it deserves more attention in terms of prevention and care. In Burkina Faso, removal of d4T in HAART regimens is an important step in this direction. Later in subsequent studies, it would be pertinent to assess the association of lipoatrophy with cardiovascular risk factors and its psychological impact.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.