
Abstract
Background:
To study the features of metabolic syndrome (MS) and its associated factors during highly active antiretroviral therapy (HAART), in Ouagadougou.
Methods:
It was a cross-sectional study from March to November 2011 in Yalgado Ouédraogo hospital. A nonprobability sample of adults receiving antiretroviral drugs for at least 6 months was studied. Pregnancy, ascites, or abdominal mass were noninclusion criteria. Metabolic syndrome met the criteria of International Diabetes Federation 2005.
Results:
The authors studied 300 patients. Metabolic syndrome was diagnosed in 54 (18%) patients: mean age 44.8 ± 7.4 years, sex ratio 0.17, and mean duration of HAART 71 ± 30.9 months. The current anomaly of MS was low high-density lipoprotein (HDL)-cholesterol in 37 patients (68.5%), and the common profile of MS was high waist circumference + low HDL-cholesterol + abnormal blood pressure (29.6%). Associated factors were protease inhibitor regimens (P = .000), female gender (P = .004), age > 42 years (P = .001), and lipodystrophy (P = .01).
Conclusion:
Cardiovascular risks should be regarded during the care of HIV-infected patients.
Introduction
Highly active antiretroviral therapy (HAART) decreases both morbidity and mortality in HIV-infected patients. However, it may involve deleterious side effects such the metabolic syndrome 1 -7 which affects sometimes more than 50% patients. 6 Many factors explain the occurrence of the metabolic syndrome in HIV-infected patients. 1,3,6,8,9 The prevention of this cardiometabolic morbidity by using antiretroviral (ARV) drugs with a low metabolic toxicity and the treatment after its early detection are the current control strategies. 1 In Burkina Faso, antiretroviral therapy is based on the World Health Organization (WHO) recommendations for developing countries. The prevalence of isolated metabolic disorders during HAART has been previously reported in Ouagadougou, 4 and metabolism syndrome is diagnosed in 10% to 12% patients in Bobo-dioulasso. 5 Because of its polymorphism in HIV-infected cohorts, 10 we aimed to determine the frequency of the metabolic syndrome as well as its clinical and biological features and to identify its associated factors in patients receiving HAART in Yalgado Ouédraogo teaching hospital (CHUYO). The study will allow raised awareness among physicians on this major cardiovascular risk factor.
Materials and Methods
Study Design
It was a cross-sectional cohort study carried from March 10 to November 10, 2011, in the day care hospital in the department of internal medicine, a tertiary care referral center in CHUYO, Ouagadougou.
Patients Selection
The study population was HIV-infected patients. We have selected an accidental and nonprobabilistic sample of outpatients (18 years old or more) who were receiving HAART for at least 6 months and have consented to the study. Pregnant women and patients suffering from ascites or abdominal mass were not included. The sample size (n = 288) were calculated with Schwartz formula:
Study Variables
Demographic, anthropometric, and lifestyle variables
The age, gender, physical activity, tobacco, and alcohol consumption were recorded by a questionnaire and patient’s clinical file. Height was measured with a wall-mounted height gauge to the nearest 0.5 cm. Weight was measured with a floor digital scale to the nearest 0.1 kg. Body mass index (BMI) was calculated by dividing weight (kg) by the square of height (m2). The BMI was classified in accordance with the WHO classification. Waist circumference was measured midway between the inferior angle of the ribs and the suprailiac crest with a measuring tape to the nearest 1 cm.
Clinical, biological, and therapeutic variables
Highly active antiretroviral therapy regimen and duration were obtained by patient’s clinical records. Blood pressure was measured with a mercury sphygmomanometer, in the sitting position, on the upper arm after a 5-minute rest period. Three readings were undertaken during the interview. First reading was discarded, and the mean of the last 2 readings was used in the analysis. The first measurement was taken on both arms to detect any difference in blood pressure between arms. If happens, the higher measure of arterial blood pressure was considered.
Operational Definitions
The diagnosis of metabolic syndrome was in accordance with the International Diabetes Federation (IDF) criteria 2005: waist circumference ≥ 94 cm in men and 80 cm in women associated with at least 2 of the following signs: triglycerides ≥ 1.5 g/L (1.7 mmol/L) or treated hypertriglyceridemia, high-density lipoprotein (HDL)-cholesterol < 0.40 g/L (1 mmol/L) in men and 0.50 g/L (1.3 mmol/L) in women, systolic blood pressure ≥ 130 mm Hg and/or diastolic blood pressure ≥ 85 mm Hg or antihypertensive treatment, fasting blood glucose > 1.0 g/L, or diabetes treatment. The diagnosis of lipodystrophy was based on clinical observations (visual diagnosis).
Statistical Considerations
Data were recorded and analyzed with Word, Epi-Info 3.5.1 (US Centers for Disease Control and Prevention, Atlanta, GA, USA), and SPSS 17.0. Quantitative data were expressed as mean ± standard deviation (SD), and proportions were used to express qualitative data. The chi-square test or Fisher test was used for comparison of proportions. To identify factors associated with the metabolic syndrome, calculations were based on 95% confidence interval.
Results
General Characteristics of the Study’s Population
Three hundred patients were studied. The main HAART regimens were zidovudine /lamivudine/nevirapine (ZDV/3TC/NVP; 32.3%) and stavudine (D4T)/3TC/NVP (26.3%). Of these patients, 54 (18%) met criteria for metabolic syndrome, of whom 46 (85.1%) were women and 8 (14.9%) men, their mean age was 44.8 ± 7.4 years, and the sex ratio was 0.17. The mean BMI was 24.4 ± 3.3 kg/m2: ≤18.5 in 2 (3.7%), from 18.5 to 25 in 18 (33.3%) and >25 in 34 (63%) patients.
Clinical Characteristics of the Metabolic Syndrome
Apart from the high waist circumference in all patients, we observed low HDL-cholesterol in 37 (68.5%) patients, abnormal blood pressure in 36 (66.7%) patients, high triglycerides in 27 (50%) patients, and high blood glucose in 16 (29.6%) patients. The different phenotypes of the metabolic syndrome in people living with HIV receiving HAART in Ouagadougou are reported in Table 1.
Frequency of Different Patterns of the Metabolic Syndrome in People Living with HIV Receiving HAART in Ouagadougou.a

Abbreviations: HAART, highly active antiretroviral therapy; high TG, high triglyceride; HTA, high blood pressure; low HDL-C, low high-density lipoprotein cholesterol.
aN = 54.
Factors Associated with Metabolic Syndrome
Demographic, anthropometric, lifestyle, clinical, and immunological factors
The metabolic syndrome was frequent in patients more than 42 years old (P = .001), in female (P = .004), and in case of lipodystrophy (P = .01). The frequency didn’t differ according BMI (P = .14), smoking status (P = .08), alcohol intake (P = .68), practice of physical activity (P = .83), and the initial CD4 count (P = .05). Table 2 reports the demographic, anthropometric, lifestyle, clinical, and immunological factors associated with metabolic syndrome in people living with HIV receiving HAART in Ouagadougou
Demographic, Anthropometric, Lifestyle, Clinical, and Immunological Factors Associated with Metabolic Syndrome in People Living with HIV Receiving HAART in Ouagadougou.a

Abbreviations: BMI, body mass index; HAART, highly active antiretroviral therapy.
aN = 300.
Therapeutic factors
In patients having metabolic syndrome, the mean duration of HAART was 71 ± 30.9 months. ZDV/3TC/lopinavir/ritonavir (LPV/r) and abacavir (ABC)/didanosine (DDI)/LPV/r were the main regimens, respectively, in 20.3% and 18.5% of patients. The metabolic syndrome was associated with exposure to protease inhibitor (PI) regimens (P = .000). Table 3 shows the therapeutic factors associated with the metabolic syndrome in people living with HIV receiving HAART in Ouagadougou.
Therapeutic Factors Associated with Metabolic Syndrome in People Living with HIV Receiving HAART in Ouagadougou.a
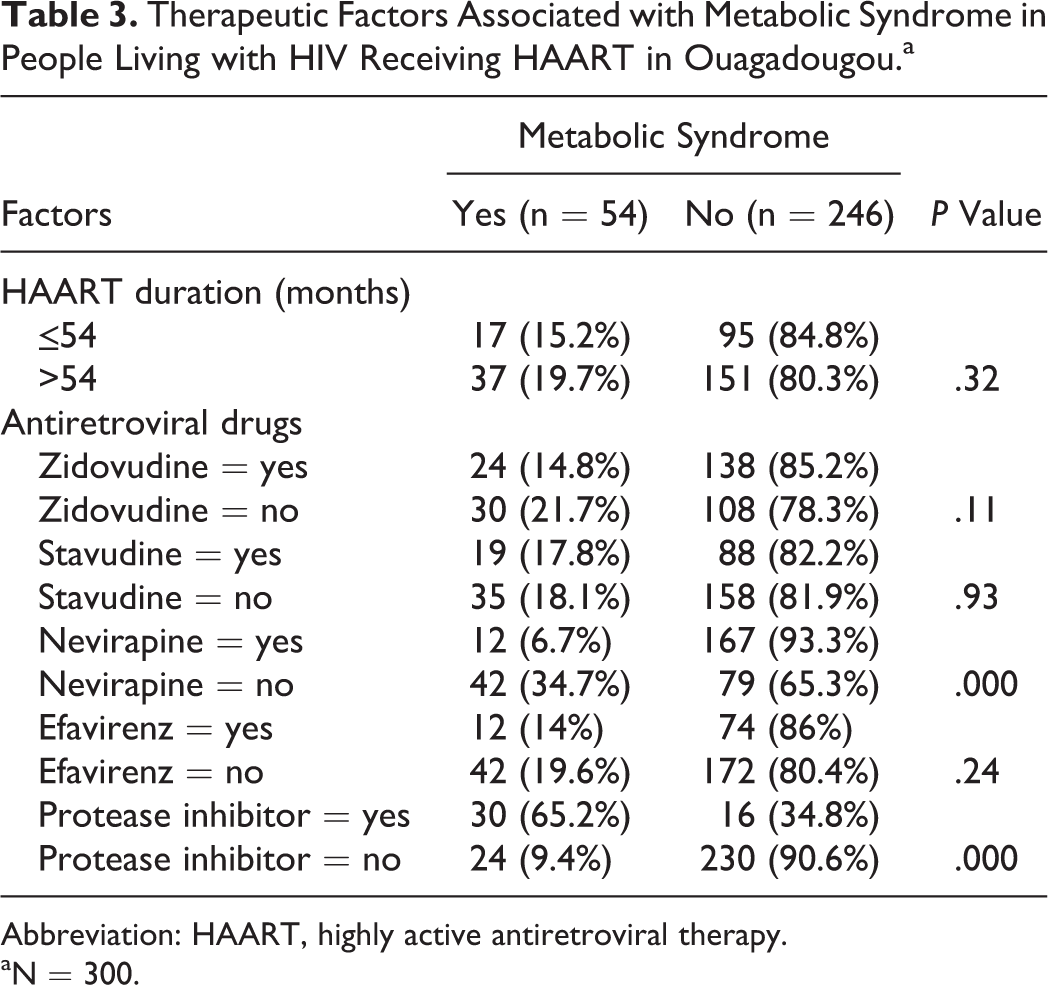
Abbreviation: HAART, highly active antiretroviral therapy.
aN = 300.
Discussion
The metabolic syndrome was diagnosed in 18% patients. Its main presentation consisted of high waist circumference plus low HDL-cholesterol plus high blood pressure. Its determining factors differed sometimes from those reported in the literature. The frequency of metabolic syndrome varies from 10% to 21% in patients receiving HAART in Africa, 5,10,11 and estimations are from 11.4% to 52.2% in Europe, 3,8,12 -15 20.6% to 25.5% in America, 1,16 and 26.2% in Taiwan. 9 This frequency is strongly related to a genetic susceptibility 1 and the diagnosis criteria (International Diabetes Federation [IDF], National Cholesterol Education Program-Adult Treatment Panel III [NCEP-ATPIII], American Heart Association/National Heart, Lung and Blood Institute [AHA/NHLBI], etc). In HIV-infected patients, the impact of ARV drugs in the pathogenesis of metabolic syndrome is sometimes questioned in studies reporting no difference in infected patients receiving HAART compared to treatment-naive patients. 10,17 Similarly, the role of the virus is discussed, and the incidence of metabolic syndrome doesn’t differ in HIV-infected patients compared to noninfected patients or the general population. 1,2,13,15,16,18 Despite these controversies, and because of HIV infection is a cardiovascular risk factor, metabolic syndrome should more preoccupy in HIV-infected patients.
In accordance with observations, low HDL-cholesterol was the main biological disorder of metabolic syndrome in patients. 1,14,19 Other authors report high triglycerides. 15 In addition to high waist circumference, low HDL-cholesterol plus abnormal blood pressure was the common phenotype of metabolic syndrome in our patients. This differs from studies suggesting the frequency of the phenotype high triglycerides plus abnormal blood glucose in patients receiving HAART compared to treatment-naive patients. 17 Other studies report the profiles of abnormal blood pressure plus high triglycerides and low HDL-cholesterol in treatment-naive patients 12 or the profiles of low HDL-cholesterol plus high triglycerides and a low incidence of abnormal blood glucose in HIV-infected patients compared to noninfected one. 16 Changes in clinical and biological standards depending on diagnosis criteria of the metabolic syndrome as well as the metabolic side effects of each HAART regimen could partly explain these differences.
Despite discordant conclusions about its determinants, 8,15,16 advanced age, female gender, and exposure to PIs are currently cited to be associated with the metabolic syndrome. 1 -3,7,9,11,13 It is also reported an association with a long exposure to ARV drugs. 1,5,10,13 But, beyond 54 months of treatment, our findings did not confirm this, strengthening observations on the early onset of metabolic disorders in African HIV-infected cohorts. 11,20 Conclusions sometimes differ on the role of initial immune deficiency. Unlike our findings, metabolic syndrome is variably associated in studies with low initial CD4 count 12 or high initial CD4 count. 1,10 Also, contrary to a Beninese’s study 11 and our observations, a Brazilian’s study didn’t report a relation between metabolic syndrome and lipodystrophy 1 ; an association was noted only in female in another study. 6 These discordant results could be supported by diagnosis criteria of lipodystrophy, which are sometimes based on subjective criteria (visual diagnosis) or on objective criteria (measurement of skinfold and imaging of fat tissue) and also by anthropometric differences in populations. Studies don’t usually address the role of physical activity in the pathogenesis of the metabolic syndrome in HIV-infected patients. We didn’t find an association in our patients. This was different from an Italian 12 and a Franco-Ivorian multicenter study 20 which report a high frequency of metabolic syndrome in sedentary lifestyle as well as a Brazilian study that found such an association among males. 21 However, because we didn’t evaluate the intensity of physical activity according to objective criteria, this represents a limit to compare our result to others. Also, our findings differ from studies reporting an association with overweight. 1,5,10,13,14 Any interpretation have to consider the proportion of central obesity in these overweight patients because this type of obesity is currently associated with metabolism syndrome. This has been shown in a study about obesity versus abdominal obesity in diabetic patients in Bobo-Dioulasso. 22
Conclusion
Modifiable components of metabolic syndrome should be monitored and controlled by a multidisciplinary care via physicians, nutritionists, psychologists, and other collaborators during the management of HIV-infected patients receiving ARV drugs. The cardiovascular risk must be evaluated and specific drugs to control metabolic anomalies should be taken into account in HIV/AIDS programs. A careful stratification of the risk and cardiovascular monitoring of patients under HAART is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.