
Abstract
Background:
In sub-Saharan Africa, few studies exist on elderly HIV-positive populations. Therefore, we aimed to examine the profiles of elderly people living with HIV (PLHIV) in Burkina Faso and their response to antiretroviral therapy (ART).
Methods:
We reviewed the monitoring and treatment of PLHIV over the age of 50 years and then compared with the monitoring and treatment of PLHIV under 50 years.
Results:
A total of 3367 patients were included. The median age of elderly people was 54.5 years and of young people was 34.9 years (P = .03). In both the groups, screening was performed following clinical suspicion (64.9% in elderly versus 56% in young people; P < .001). Cardiovascular risk factors were generally more significant in the elderly people. The risk of death while on ART was 2.3 times higher in elderly people (P < .001).
Conclusion:
HIV infection in older people occurs in those who already have some cardiovascular risk factors. Particular attention should be given to multidisciplinary care for the elderly individuals.
Introduction
Since the introduction of antiretroviral treatment (ART) in people living with HIV (PLHIV), the mortality rate related to HIV infection decreased dramatically. 1 As a result, the life expectancy for PLHIV increased, and in both developing and developed countries, the HIV-positive population is aging. 2
According to the World Health Organization (WHO), an HIV-positive person is considered to be “elderly” when she or he is at least 50 years of age or older. 1 Although the HIV pandemic primarily affects young adults aged 15 to 49 years, elderly people are also concerned. In the United States, 11% of all reported cases of AIDS, the syndrome which is caused by HIV, were people over the age of 50. 3 Based on French hospital databases, 23% HIV-infected individuals are over 50 years of age. They represent 18% of newly diagnosed HIV cases. 4
In sub-Saharan Africa, there are only few studies on elderly HIV-positive populations. 5,6 In Burkina Faso, 14 000 (16%) people over the age of 50 were living with HIV, in 2011. 7 In Burkina Faso, the prevalence of HIV infection in young patients aged 15 to 49 years and in those aged 50 years or older was estimated at 1% in 2011. 5 No previous studies have examined the profiles of elderly individuals and importance of age in HIV cohort treatments in Burkina Faso. Furthermore, the consequences of HIV infection on the response to ART before and after 50 years of age have never been studied. The objective of this article is to study the characteristics of elderly PLHIV in Burkina Faso and their response as well as the overall mortality under ART.
Patients and Methods
We carried out a retrospective cohort study. To be included in the study, participants had to be 15 years or older. We reviewed the monitoring and treatment of PLHIV over the age of 50 years and then compared them to the monitoring and treatment of PLHIV under 50 years.
This study was carried out between January 2007 and December 2011 at the hospital day clinic at the Souro Sanou University Hospital (CHUSS) in Bobo-Dioulasso, Burkina Faso’s second city. About 6792 people were being monitored at CHUSS at the time of the study. Patients were enrolled in the therapeutic cohort at the clinic based on the following criteria: be at least 15 years of age, test HIV positive, based on the diagnostic algorithm in place in Burkina Faso, and visit the day clinic at CHUSS for the first time during the period of the study.
To complete our retrospective cohort, we extracted variables from the computerized database at the day clinic. The variables studied were sociodemographic (screening age, gender, marital status, level of study, professional occupation, and residence), temporal (consultation deadline and circumstance of discovery), clinical (opportunistic infections, WHO stage, and body mass index [BMI]), and biological variables (HIV type, CD4 count, glycemia, creatininemia, cholesterol, triglyceridemia as well as those concerning patient’s therapy [ART combination] and monitoring [death, lost to follow-up, and transfer]). For beginning ART, the criteria outlined by WHO were used. 1 Similarly, WHO criteria were used for the introduction of cotrimoxazole as a prophylaxis; the prophylaxis was recommended, in the absence of contraindication, for patients with CD4 count ≤350 cells/mm3 or stage 2, 3, or 4 HIV infection, based on WHO criteria.
The data were analyzed using Epi info 3.5.1. and MedCalc 11.2.0.0 softwares. The characteristics of the study population were described by number, proportion with confidence intervals in ranges for qualitative variables and means, standard deviations, and interquartile ranges (IQR) for quantitative variables. The proportions were compared using Pearson chi-square test or Fisher exact test, where appropriate. Student t test was used to test equality of 2 means from independent samples; when conditions for application were not met, the Mann-Whitney nonparametric test or the Kruskal-Wallis test was used. Immunological efficiency (increase in CD4 count at more than 500 cells/mm3) and virology (detectability of viral load) were estimated at 6, 12, 24, and 48 months of ART. Survival at 6, 12, 24, and 48 months was examined using the Kaplan-Meier method. The survival curves of elderly and young people were compared using the log-rank test. The logistic regression (univariate and multivariate) made it possible to identify the predictors of death in each group regardless of the time of participation in the cohort. A value of P ≤ .05 was used the threshold for statistically significant differences.
Ethical Considerations
Ethical norms and national legislation were respected during the course of the study. We obtained research authorization from hospital officials. We ensured anonymity of participating patients and confidentiality of data used in the study.
Results
Profiles of Elderly PLWH
Sociodemographic and anthropometric characteristics
A total of 3367 patients were included in the study (Figure 1). The median age for HIV screening was 54.5 years (IQR: 52-57.4) in elderly people and 34.9 years (IQR: 29.6-40.9 years) in young people (P = .03). The sex ratio (M/F) was 1.2 in elderly PLHIV and 0.4 in young PLHIV (P < .001). Table 1 shows the sociodemographic characteristics of the patients.

Trends in pretreatment and antiretroviral (ARV) follow-up of patients by age group at screening.
Sociodemographic Characteristics at ART Initiation.
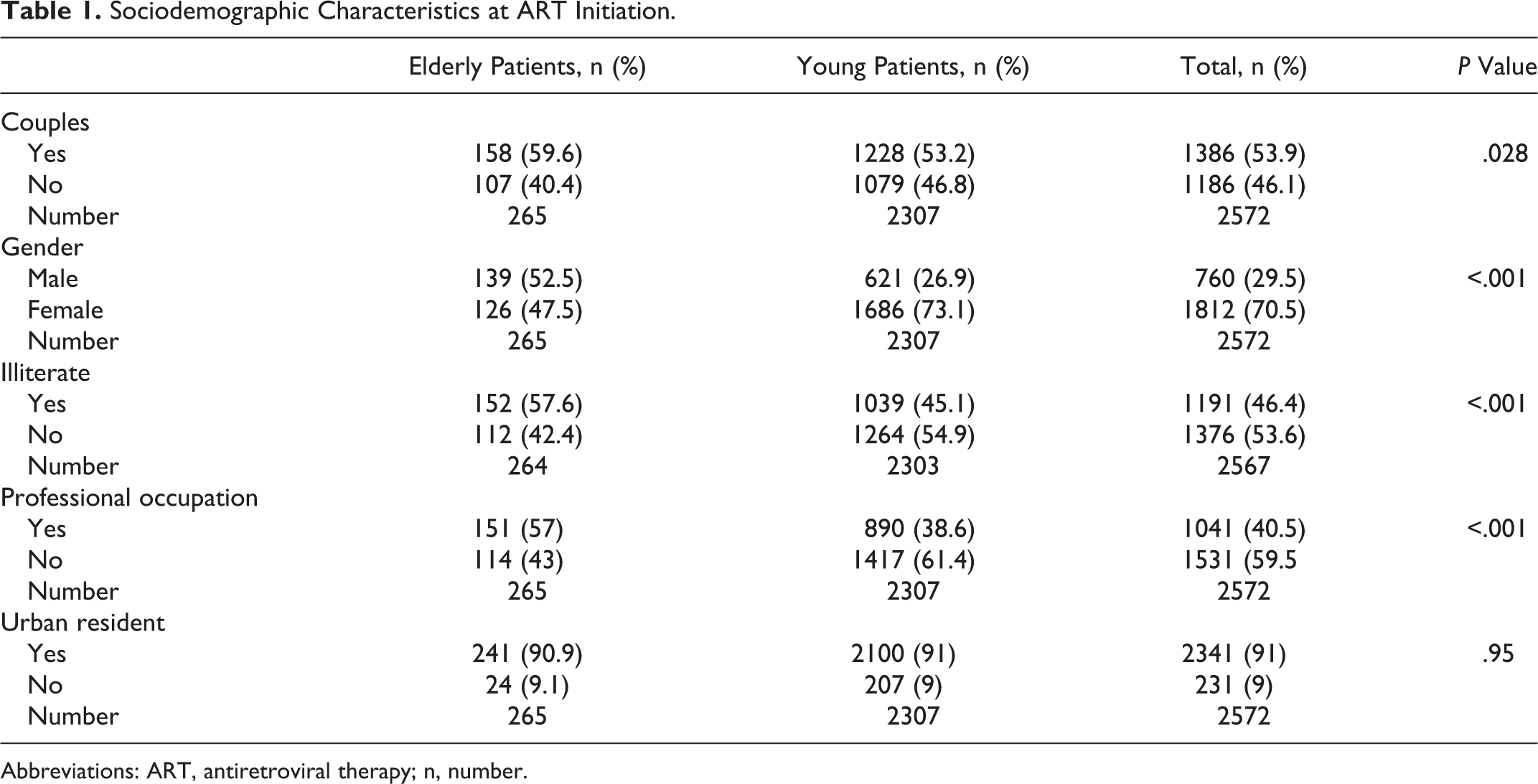
Abbreviations: ART, antiretroviral therapy; n, number.
Screening was performed following clinical suspicion in the 2 groups (64.9% in elderly people compared to 56% in young people; P < .001). HIV-1 was more common (90.9%) in both the groups. Median BMI was 19.8 kg/m2 in elderly people and 20.5 kg/m2 in young people (P = .03). Cardiovascular risk factors were generally more significant in elderly people than in young people: arterial hypertension (36.2% compared to 13.2%, P = .001), hyperglycemia (7.2% compared to 5.4%, P = .36), hypercholesterolemia (10.4% compared to 7.6%, P = .53), and hypertriglyceridemia (18.3% compared to 16%, P < .001). Hypercreatininemia was more common among elderly patients (7.1% compared to 3.3%, P = .02). More than half of both elderly (59.2%) and young (53.1%) patients were at an advanced stage of infection at the time of its discovery (P = .003).
Clinical and biological characteristics at ART initiation
In the study, 2572 (76.4%) patients began ART: 265 elderly PLHIV and 2307 young people. The median CD4 count was 174 cells/mm3 in elderly people, compared to 178 cells/mm3 in young people. The CD4 count was <350 cells/mm3 in 97.1% of elderly PLHIV and 89.6% in young PLHIV (P = .001). Table 2 shows the prevalence of clinical and biological anomalies at the introduction of ART. The median time of ART initiation was 31 days IQR18-84 and 41 days IQR21-166 for elderly and young PLHIV, respectively (P = .025). The use of frontline Protease inhibitor (IP) was more common in elderly PLHIV than young PLHIV (19.6% compared to 13.7%; P < .001). Table 3 shows initial therapeutic protocols.
Prevalence of Clinical and Biological Anomalies at ART Initiation.
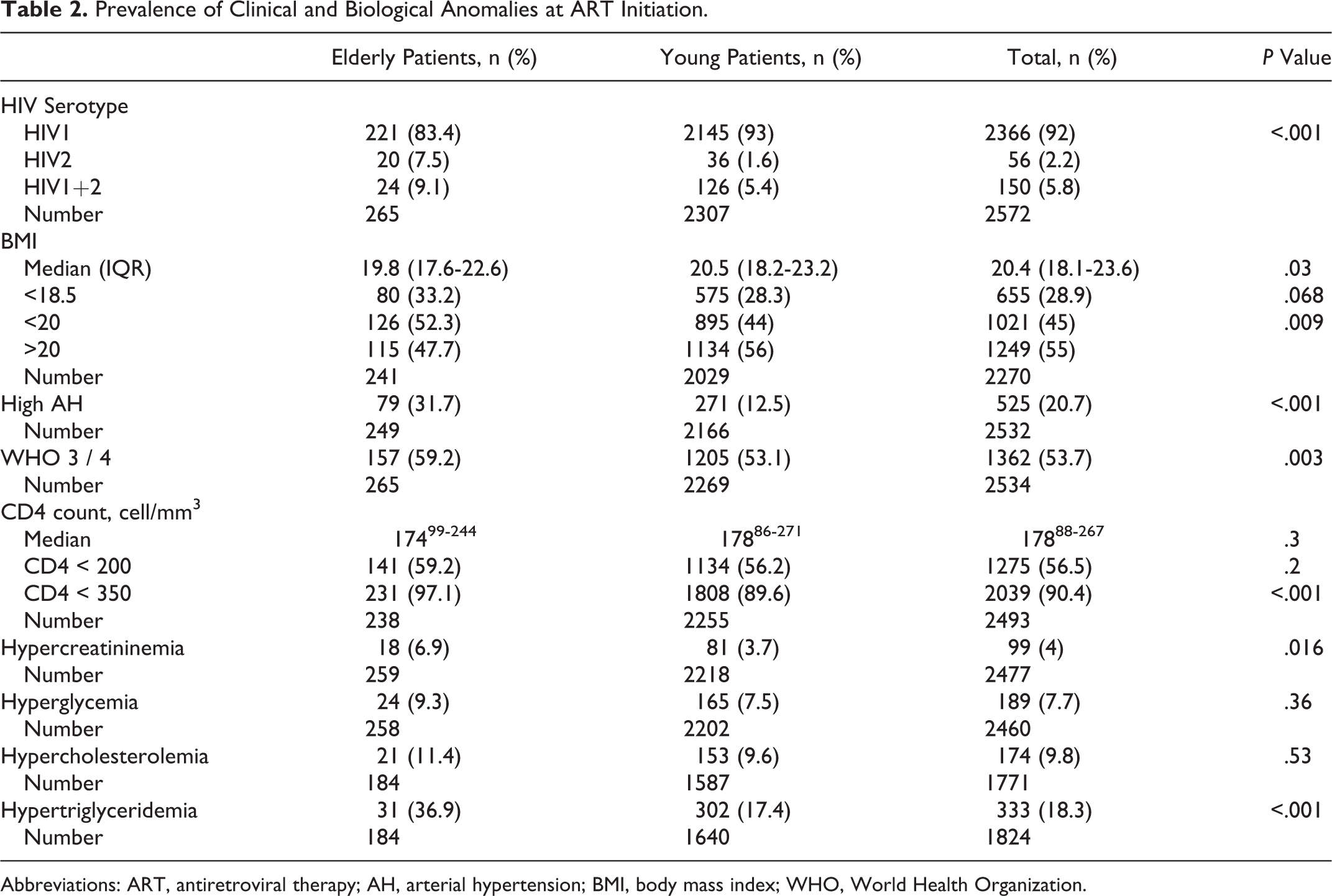
Abbreviations: ART, antiretroviral therapy; AH, arterial hypertension; BMI, body mass index; WHO, World Health Organization.
Initial Therapeutic Protocols and Schemas.

Abbreviations: ABC, abacavir; d4T, stavudine; EFV, efavirenz; IDV, indinavir; INTI, Integrase inhibitor; LPV, lopinavir; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-nucleoside-reverse transcriptase inhibitor; NVP, nevirapine; PI, protease inhibitor; ZDV, zidovidine; 3TC, lamividine.
Response to ART in Elderly PLWH
Under ART, the median rate of CD4 progression was 154 and 158 cells/mm3 in elderly PLHIV and young PLHIV, respectively. After 24 weeks (6 months), 95.5% (109 of 113) of elderly patients and 96.2% (1101 of 1144) of young patients had an undetectable viral load (P = .23). The median time for confirming an undetectable viral load was 23 and 24 months in elderly and young patients, respectively. Under ART, cardiovascular risk factors, such as arterial hypertension, hypertriglyceridemia, and hypercreatininemia, were significantly more frequent in elderly patients than young. Table 4 shows the incidence of clinical and biological events under treatment.
Incidence of Clinical and Biological Events under ART.

Abbreviations: AH, arterial hypertension; ART, antiretroviral therapy; pa, Patient year.
Two hundred ninety-five (11.4%) deaths were recorded under ART (295/2572), including 56 elderly patients (56/265 or 21%) and 239 young patients (239/2307 or 10.3%; P = .001). Survival under ART is illustrated in Figure 2.

Survival curve under antiretroviral therapy (ART).
Discussion
Elderly people represented 10.3% (346/3367) of new patients in our cohort. This frequency is variable throughout the world (11.4% in sub-Saharan Africa, 9.9% in Europe, 15% in the United States, and 27% in North America in similar cohorts 8 -10 ). The low rate of screening in elderly people and the short evolution time of their illness led to an underestimation of infection in the therapeutic cohort. Behavioral risk factors and lack of targeted HIV prevention campaigns for people over the age of 49 could have led to the increase in HIV infection in elderly people. 11 The absence of epidemiological monitoring of HIV infections in people over the age of 49 partially explains the lack of data and consideration in HIV response.
The median age for screening elderly patients was 54.5 years and for young patients 34.9 years (P < .001). More males were screened than females (P < .001). In Africa, HIV screening tends to be predominantly females in groups under the age of 50, though results are different between authors and countries. 9,12,13 Higher age at the time of screening seems to be a risk factor for morbidity and mortality. 9 The higher proportion of males after the age of 40 could be linked to a higher probability of late diagnosis or sexual activity, a risk factor for HIV infection. 7,14 In our series, elderly people were more likely to be illiterate (61.7% compared to 46%; P < .001), have professional careers (57.9% compared to 37.8%, P < 001), and reside in urban areas (91.4% compared to 87.9%, P = .05). Orchi et al in Italy also observed the same trends regarding education level and professional activity. 15
One hundred eighty-four elderly patients, or 54.6%, were at WHO stage 3 infection, compared to 50% of young patients. The difference was not statistically significant (P = .12). For patients in the study, screening was most often done at an advanced stage of infection. 8,16 -18
HIV-1 was the predominant serotype. Infection by HIV-1 and 2 was found in 3.1% and 5.9% of patients, respectively. HIV-2 infection was more frequent in elderly patients than in young patients (P < .001).
Elderly people (54.6%) and young people (50%) were more symptomatic (WHO stages 3 and 4) at the time of discovery of the infection (P = .12). In Africa, patients are generally diagnosed at an advanced stage of the illness. 16 -18 Some authors reports a significantly higher prevalence of WHO stage 4 infection among elderly people than young people. 19,20
In our cohort, the rate of CD4 count at screening was low, regardless of age at the time of screening: 18599-314 cells/mm3 in elderly PLHIV and 20590-357 cells/mm3 in young PLHIV (P = .36). Our results are different from some cohorts in the North, with a significant difference in CD4 count between elderly people (low) and young (higher). 10,21,22 The late diagnosis in the study could be the main cause.
Arterial hypertension, hypercreatininemia, and hypertriglyceridemia were the biggest risk factors in our patients at the initial examination. During the course of the study, in addition to cardiovascular risk factors cited, the rate of hyperglycemia was higher in elderly people than in young patients (P < .0001). Literature corroborates this observation: The frequency of cardiovascular risk factors (arterial hypertension, hyperglycemia, hypercholesterolemia, and hypertriglyceridemia) is higher in HIV-positive patients. 23 -29
During the course of the study, the increase in the incidence of certain factors such as hypercreatininemia in elderly patients under ART could be linked to the use of tenofovir (TDF) or traditional medicine. 30
A median increase in CD4 count was observed at 12 months in elderly PLHIV compared to 6 months in young people. A similar immunological progression was observed by other authors. 13 According to Chêne et al, the late immunological reconstitution after 6 months of treatment of PLHIV would have a more important negative prognostic value than CD4 count at initiation. 21
For those under ART, the risk of death was 2.3 (1.52-3.32) times higher in elderly patients than in young. Patient death was most frequent in the first 6 months of ART. The mortality in Collins et al cohort was 2.7 (1.8-4.08) times higher in elderly patients than young, after adjusting for confusion factors. 13 Body mass index <18 kg/m2, WHO stage 3 infection or Stage C from CDC, CD4 rate <200, hemoglobin rate <10 g/dL, and viral load >5 log10 are all factors associated with early death under ART. Age at the time of screening ≥50 years was also a predictive factor of early death under ART. 16 -18
Conclusion
HIV infection in elderly patients is a reality. It exists alongside cardiovascular risk factors, which become more frequent after infection. Late screening, advanced stage of infection at the time of screening, and inadequate immune response often decrease the long-term prognosis.
These results could have important implications in the management of HIV infection in elderly patients who should be targeted by appropriate public health interventions, such as screening and information about HIV, prevention of risk behaviors, and acquisition and progression of HIV infection. Particular attention should be paid to multidisciplinary treatment of elderly PLHIV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.