
Abstract
Background:
The current US HIV treatment guidelines support initiation of antiretroviral therapy (ART) for persons with HIV for personal health benefits and prevention of HIV transmission. However, high levels of adherence to ART are critical to maximize individual and public health benefits. We examined the nonclinical barriers to ART initiation for clinically eligible individuals and the provider- and patient-related factors associated with these barriers among HIV-infected patients in Houston/Harris County, Texas.
Methods:
We analyzed data obtained from a probability sample of HIV medical care providers (HMCPs) in 13 outpatient facilities in Houston/Harris County, Texas surveyed between June and September 2009. We used an inductive thematic approach to code HMCP responses to an open-ended question that asked the main reasons why providers may delay initiating ART for clinically eligible patients.
Results:
The reasons cited by providers for delaying ART for clinically eligible patients were adherence (42.5%; 95% confidence interval [CI]: 28.5-57.8), acceptance (30%; 95% CI: 18.1-45.4), and structural concerns (27.5%; 95% CI: 16.1-42.8), with significant variations (P < .0001) noted across patients’ race/ethnicity and transmission category. HIV medical care providers with 6 to 10 years’ experience in HIV care and those providing medical care for more than 100 patients monthly were about 4 times (adjusted odds ratio [aOR]: 3.80; 95% CI: 1.20-5.92; P = .039) and 10 times (aOR: 10.36; 95% CI: 1.42-22.70; P = .019) more likely to state adherence and acceptance concerns, respectively, as reasons for delaying ART for clinically eligible patients.
Conclusion:
Our findings highlight the fact that clinical guidelines are only a starting point for medical decision-making process and that patients themselves play an important role. HMCP access to referrals for other medical issues, support services, and treatment education may help improve adherence and patient readiness for ART, thereby avoiding systemic delays.
Introduction
The availability of an increasing number of antiretroviral agents and the rapid evolution of new information have revolutionized the treatment and management of HIV and introduced substantial complexity into treatment regimens for persons infected with HIV. 1 Early initiation of antiretroviral therapy (ART) has been shown to improve long-term CD4 count recovery and immune restoration. 2 –4 Retention in HIV care has been documented to reduce the risk of developing HIV opportunistic illnesses, increase survival rates, improve access to supportive services, and improve overall quality of life. 5 –8 Although several studies have highlighted the prevalence, trends, and disparities in ART use, 9 –12 only a few have attempted to specifically address the reasons why providers delay ART initiation for clinically eligible patients. 13 –16
As of March 2012, the US Department of Health and Human Services HIV treatment guidelines recommend ART for all HIV-infected individuals, regardless of CD4 count, to reduce the morbidity and mortality associated with HIV infection and to prevent HIV transmission. 17 –19 However, despite the positive impact of these guidelines on medical care for people living with HIV (PLWH), it urges providers to consider a patient’s comorbid conditions, willingness, and readiness to initiate therapy, 18 as well as address patient barriers to adherence to avoid treatment failure and viral resistance. 20,21 On a case-by-case basis, providers may choose to defer ART initiation based on clinical and/or psychosocial factors such as substance use, mental health, comorbidities, and patient unreadiness. 16 –19 Some studies suggest that providers may delay recommending ART to eligible patients because of concerns that patients will be unable to benefit from or adhere to ART. 13 –16
Among more than 20 000 individuals living with HIV in Houston/Harris County, Texas, 27% are estimated to be out of care, while an estimated 3324 (37%) individuals previously under medical care are out of care. 22 In a recent study, 23 we identified several patient-level barriers to HIV care in Houston/Harris County, some of which may help inform providers’ decisions to delay ART initiation for clinically eligible patients. Of equal importance to providers’ decision-making with respect to ART initiation are provider-level demographics and practice characteristics. 13,16
Whereas only few research studies have examined the extent to which HIV treatment guidelines are systematically followed by clinicians who treat PLWH, 24,25 some studies indicate significant variations in treatment patterns and practices based on years of experience, number of HIV-infected patients under care, provider demographics, and having sufficient time or ancillary support to provide counseling services. 13,16,24 Thus, the new expanded ART eligibility guidelines, 17 –19 coupled with increased HIV testing and linkage to and engagement in care, will likely increase the size of the population of PLWH and consequently expand the number of patients for whom providers will consider initiating ART. 16 Modeling studies suggest that expanded use of ART may lower incidence and, eventually, prevalence of HIV on a community or population level. 26
After HIV diagnosis, a timely initiation of ART for clinically eligible patients is an important first step in the continuum of care. However, understanding the important factors that may be associated with providers’ decision to delay ART for clinically eligible patients may enhance improved retention in pre-ART care, reduce HIV-associated morbidity, and help design strategies that will motivate early treatment initiation for purposes of achieving ART’s therapeutic and preventative benefits. Similarly, characterizing HIV care providers who care for patients experiencing specific barriers to ART initiation may inform targeted provider education and training that will provide resources and the support needed to extend the benefits of ART to all of their clinically eligible patients. 16 This study examined the types of nonclinical barriers to ART initiation for clinically eligible individuals and the patient- and provider-related factors associated with these barriers among PLWH in Houston/Harris County, Texas.
Methods
Survey Design and Participants
Data for this study were collected as part of the Centers for Disease Control and Prevention’s (CDC) Medical Monitoring Project (MMP) Provider Survey. The survey was administered to a nationally representative sample of HIV medical care providers (HMCPs) who were selected to participate in MMP. The MMP is a complex cross-sectional survey design conducted in 23 US states and territories in which persons diagnosed with HIV (aged 18 years and older) are selected to participate. Further details on MMP and the associated sampling method have been described previously, 27,28 and detailed description of the MMP Provider Survey can be found in the study by Mgbere et al 24 and Frankel et al. 29
The Houston/Harris County, Texas component of the MMP Provider Survey data was used for the current study. The survey was conducted in Houston/Harris County, Texas from June through September 2009 in collaboration with the CDC. The survey participants consisted of a probability sample of HMCPs from 13 outpatient facilities who agreed to participate in the survey. The HMCPs eligible for this survey included physicians, physician assistants, and nurse practitioners working in one of the MMP-sampled facilities and who provided care, ordered CD4 count or HIV RNA viral load testing, and/or prescribed antiretroviral medication to HIV-infected individuals ≥18 years of age. Interns, residents, fellows, and others in training programs were not eligible to participate in the survey. Providers who obtained CD4 counts and HIV RNA viral loads only for referral purposes or provided ART refill prescriptions but did not play a more active role in managing their patients’ HIV infection were also not eligible to participate in the survey.
Recruitment and Data Collection
Prior to data collection, facilities participating in MMP were contacted for the names and contact information of eligible providers within each facility. A unique identification number was assigned to each provider based on a list of sequential ID numbers for each facility. Using the identification numbers, personalized recruitment packets were mailed to eligible HIV care providers within the 13 participating facilities in the Houston/Harris County project area. The recruitment packets comprised of a recruitment letter describing the purpose of the survey, information on how to access the survey online using the provider’s unique identification number, a paper copy of the survey with a postage-paid return envelope, and a small monetary incentive in the form of a gift card.
A total of 51 personalized recruitment packets were mailed to eligible HIV care providers within the 13 participating facilities in the Houston/Harris County project area. A modified version of the Dillman total design method 30,31 was used to follow-up with nonresponders. The process involved following up with nonresponders after the first, third, and seventh week following the initial mailing. Twenty-three HMCPs completed the survey, representing a response rate of 45%. The survey instrument consisted of 35 main items that assessed the HIV care providers’ demographic and medical practice characteristics, patient characteristics, HIV care and treatment, referral practices, HIV risk reduction counseling practices, and perceptions of patients’ barriers to HIV care. The survey required approximately 20 minutes to complete.
Analytic Measures
Dependent measures
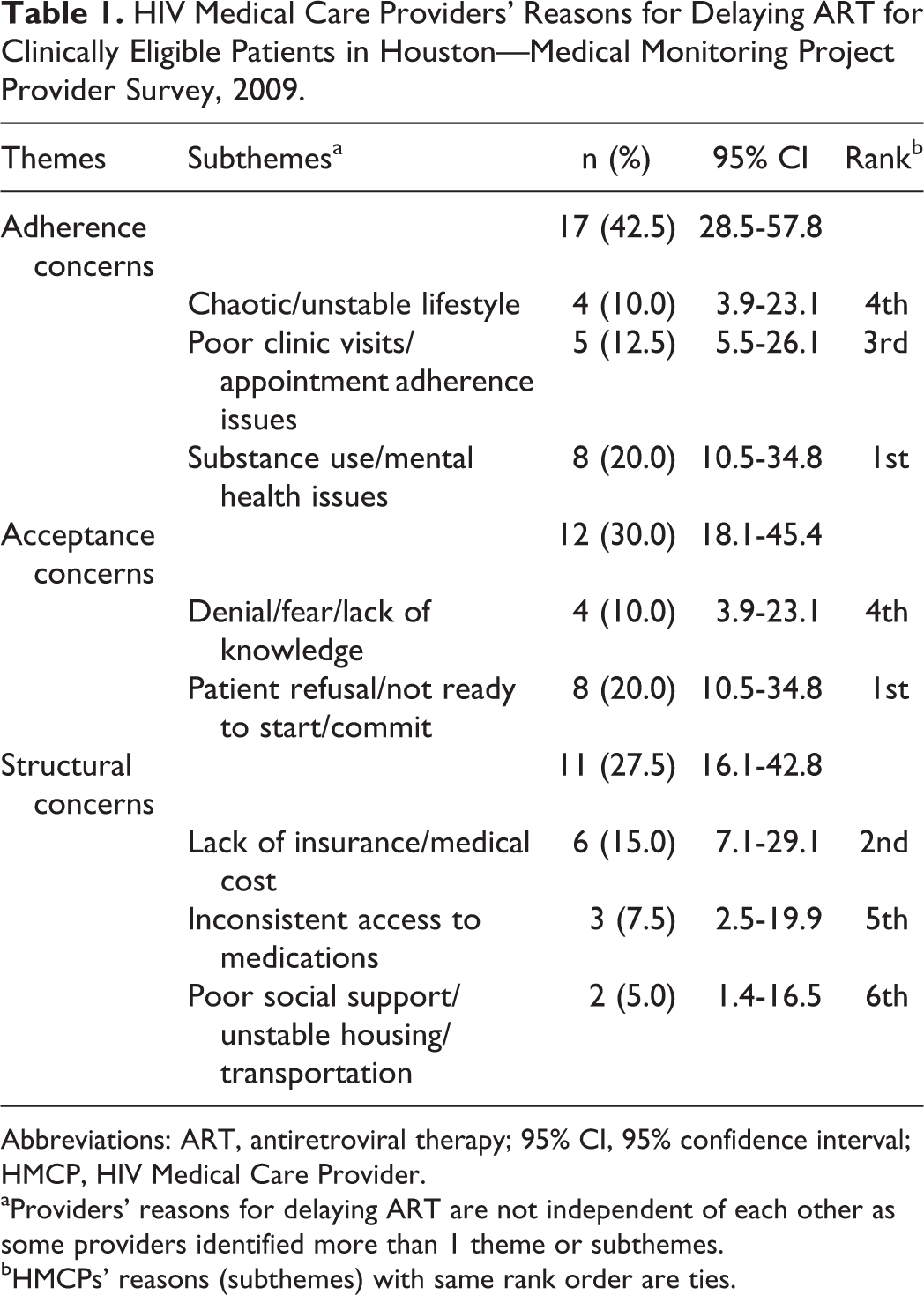
The main outcome variable was based on the HMCPs’ response to an open-ended question which asked: “For patients who are clinically eligible for ART, what are the main reasons that you might delay initiating ART?” The intent of the question was to assess nonclinical reasons for delaying ART. Therefore, clinical eligibility for ART was not defined for the providers when the study was conducted, as there would have been disagreement on when to prescribe ART. 16 Our study was conducted in 2009 prior to the new treatment guidelines that recommend ART for all HIV-infected individuals regardless of CD4 count. 17 –19 Using responses to the question, we conducted an inductive thematic analysis. 32 First, a standardized iterative process 33 was used by the researchers to develop a codebook with thematic codes for nonclinical reasons, informed by literature on barriers to ART initiation. 10 –16 To ensure reliability, 3 of the researchers independently coded the responses. Data obtained were reviewed and discrepancies were identified and reconciled after deliberations, and where necessary, coding criteria were modified by consensus. Three main themes (adherence, acceptance, and structural concerns) and 8 subthemes (substance use/mental health issues, patient refusal/not ready to start/commit, lack of insurance/medical cost, poor clinic visits/appointment adherence issues, denial/fear/lack of knowledge, chaos/unstable lifestyle, inconsistent access to medications, and poor social support/unstable housing/transportation) were identified based on the work of Beer et al 16 (Table 1). The proportions of patients’ subpopulations affected by the different reasons cited by HMCPs for delaying ART for clinically eligible patients were computed as products of the resultant themes fraction and the subpopulations of patients they provided care for per month in their facility.
HIV Medical Care Providers’ Reasons for Delaying ART for Clinically Eligible Patients in Houston—Medical Monitoring Project Provider Survey, 2009.
Abbreviations: ART, antiretroviral therapy; 95% CI, 95% confidence interval; HMCP, HIV Medical Care Provider.
aProviders’ reasons for delaying ART are not independent of each other as some providers identified more than 1 theme or subthemes.
bHMCPs’ reasons (subthemes) with same rank order are ties.
Independent measures
The independent measures used in this study include providers’ demographics (profession, age category, gender, race/ethnicity, infectious disease board certification status, years caring for HIV-infected patients, language of communication), medical practice characteristics (number of HIV-positive patients providing care to per month, self-rated knowledge of HIV care, sufficiency of time for patient care, referral for ART initiation), and patient characteristics (race/ethnicity and transmission category). These characteristics have been described in detail in related studies. 23,24
Data Analysis
The themes and subthemes were initially subjected to descriptive statistics. Using the themes (adherence, acceptance, and structural concerns) that represent the nonclinical barriers to ART initiation for clinically eligible patients, patient race/ethnicity, and transmission category, we conducted an unbalanced factorial analysis of variance designed to determine differences across these characteristics. This produced covariate-adjusted means (least square means) for the main effects and associated interaction effects that were compared using Tukey honest significant difference post hoc test.
Furthermore, we conducted χ2 tests of independent associations across provider demographic and medical practice characteristics by the themes. Following the outcome of this analysis, providers’ factors independently associated with reasons for delaying ART for clinically eligible patients were assessed using multivariable logistic regression. The provider demographic and medical practice characteristics within each theme were selected a priori, if they were statistically significant at P < .15 in the univariate analysis and included as predictors in the multivariable logistic regression models by themes (adherence, acceptance, and structural concerns). Therefore, the number of predictor variables that met the entry criteria varied slightly within each model. This process allowed for simultaneous adjustments of any potential confounders due to bias and produced estimates of P values, adjusted odds ratios (aORs), and 95% confidence intervals (95% CIs) by the themes. The models’ fitness was determined using the McFadden’ pseudo R 2 and maximum likelihood ratio test. All tests performed were 2 tailed, with a probability value of .05 used as the statistical significance level. Data management and statistical analyses were conducted using SAS statistical software version 9.4 (SAS Institute, Cary, North Carolina).
Ethical Considerations
The MMP was determined by the National Center for HIV, Viral Hepatitis, STD, and TB Prevention’s Office of the Associate Director for Science at the CDC to be a nonresearch, public health surveillance activity used for disease control program or policy purposes. As such, MMP is not subject to human subjects’ regulations, including federal institutional review board approval. As an amendment to MMP, the MMP Provider Survey was covered under the same nonresearch determination. All data collection was Health Insurance Portability and Accountability Act compliant.
Results
Characteristics of HMCPs
The demographic and medical practice characteristics of the survey participants in the current study have been presented in detail previously. 23,24 In summary, the majority of the HMCPs were physicians (73.9%), with 26.1% of them representing physician assistants and nurse practitioners. Most worked in publicly funded settings (56.5%) such as community health centers and 43.5% worked in private practice. The mean age of the HMCPs who completed the survey was 46.7 (standard deviation [SD] = 7.39) years. More than half of the providers were white (52.2%) while Black/African American and Hispanic/Latino providers were equally represented (17.4% in both groups). Most participants (91.3%) had 6 years or more of clinical experience, with an average of 11.7 (SD: ±6.63) years of practice. The overall gender distribution showed that males were majority (52.2%). Although all providers considered themselves to be knowledgeable in HIV treatment, only 60.9% self-identified as board-certified infectious disease physicians. English (47.8%) and a combination of English and other languages (52.1%) were used to provide HIV-related medical care to patients.
Reasons for Delaying ART Initiation
The reasons given by HMCPs for delaying ART in clinically eligible patients fell under 3 main themes and 8 subthemes and are presented in Table 1. Many of the reasons were related to adherence concerns (42.5%; 95% CI: 28.5-57.8). This was followed by patients’ acceptance concerns (30%; 95% CI: 18.1-45.4) and structural concerns (27.5%; 95% CI: 16.1-42.8). Within adherence concerns, substance use/mental health issues (20.0%) was the most common reason why providers may delay ART for clinically eligible patients in Houston, followed by poor clinic visits/appointment adherence issues (12.5%). The least common barrier was chaotic/unstable lifestyle (10.0%). Barriers identified within acceptance concerns included patient refusal/lack of readiness to start or commit to ART (20.0%) and patient being in denial/fear/lack of knowledge (10.0%). Of the proportion of providers who identified structural-related concerns as the reasons for delaying ART, 15% cited lack of insurance/medical cost as the main nonclinical barrier followed by inconsistent access to medications (7.5%) and poor social support/unstable housing/transportation (5.0%).
The overall ranking of the reasons for delaying ART initiation for clinically eligible HIV-positive patients in Houston indicates that substance use/mental health issues and patient refusal or lack of readiness to start or commit to therapy were ranked first, lack of insurance/medical cost was ranked second, and poor clinic visits/appointment adherence issues were ranked third. Poor social support/unstable housing/transportation was the least common reason (ranked sixth) cited by providers for delaying ART initiation for clinically eligible patients.
Comparison of Reasons for Delaying ART Initiation across Themes and Patient Characteristics
Table 2 presents the mean proportions of patient subpopulations associated with reasons stated by HMCPs for delaying ART for clinically eligible patients. Our study noted significant (P < .0001) differences across the main factors and the associated interaction effects. Overall, access to ART was deferred for 10.3% (95% CI: 8.9-11.6) of patients who were clinically eligible due to adherence concerns compared to 6% (95% CI: 4.7-8.0) of deferrals that were associated with acceptance and structural concerns. More Blacks/African Americans (15.3%) than Hispanics/Latinos (9.4%) and Whites (9.3%) experienced delayed ART initiations due to nonclinical barriers (P < .0001). Similarly, men who have sex with men (MSM) were most impacted (17.5%) by delays, followed by women (12.4%), while injection drug users (IDU; 3.8%) and transgender/transsexual (1.5%) patients were generally less affected by the barriers to ART initiation.
Mean Proportion of Patient Subpopulations Associated with Reasons Cited by HMCP for Delaying ART for Clinically Eligible Patients in Houston, Texas—Medical Monitoring Project Provider Survey, 2009.a

Abbreviations: ACC, acceptance concerns; ADC, adherence concerns; ART, antiretroviral therapy; df, degree of freedom; HMCP, HIV Medical Care Provider; MSM, men who have sex with men; STC, structural concerns; TG/TS, transgender/transsexual.
aWithin characteristic, mean proportions (%) for level with different superscript letters (g, h, j, l, n, o) are significantly different at P < .05.
bSummary is based on 2 independent analytical models built.
cMeans are least square means adjusted for covariates in the general linear model.
dSignificant level of P < .001.
eSignificant level of P < .0001.
fProviders’ reasons for delaying ART were not independent of each other as some providers identified more than one theme or subthemes.
iHispanics/Latinos were not distinguished by country of origin.
kOther include American Indian or Alaska Native and Native Hawaiian or Other Pacific Islander.
mDistinction was not made on the mode of transmission for women.
However, interaction effects between the themes and race/ethnicity (P = .0001) showed that Blacks/African Americans (19.7%) had more adherence issue-related delays than Hispanics/Latinos (11.2%) and Whites (10.6%). Similar trends were recorded for the proportion of patients for which ART initiations were delayed by providers due to acceptance and structural concerns (Table 2). Men who have sex with men experienced more adherence-related (25.8%) and structural-related (16.7%) delays in ART initiation compared to women whose delays were more associated with adherence and acceptance concerns (13.8%) and structural concerns (10.6%). The IDU experienced more adherence-related barriers (8.3%) to ART initiation than acceptance (1.8%) and structural (1.3%) barriers.
Factors Associated with Reasons for Delaying ART Initiation
The association between reasons for delaying ART and HMCPs’ demographic, practice, and medical care characteristics is presented in Table 3. We recorded significant variations by race/ethnicity (P = .001), years caring for HIV-infected patients (P = .051), and referral of patients for ART initiation (P = .002) among providers who cited adherence concerns as one of the reasons for delaying ART for clinically eligible HIV-infected patients. Multivariable modeling of adherence concerns (R 2 = .53; P = .001) revealed that providers who had 6 to 10 years’ experience caring for HIV-infected patients were about 4 times (aOR: 3.80, 95% CI: 1.20-5.92; P = .039) more likely than those with 1 to 5 years’ experience to encounter adherence concerns as reason for delaying ART initiation. On the other hand, providers of Hispanic origin were 97% (aOR: 0.03, 95% CI: 0.00-0.37; P = .004) less likely than white HMCPs to cite adherence concerns as reasons for delaying ART initiation among their clinically eligible patients.
HIV Medical Care Providers’ Demographic, Practice, and Medical Care Characteristics Associated with Reasons for Delaying ART for Clinically Eligible Patients in Houston, Texas—Medical Monitoring Project Provider Survey, 2009.a

Abbreviations: aOR, adjusted odds ratio; ART, antiretroviral therapy; 95% CI, 95% confidence interval; df, degree of freedom; R 2, coefficient of determination.
aSignificant estimates and P values are bolded.
bWithin a given characteristic, the percentages may not add up to exactly 100 due to rounding.
cSignificant level of P < .05.
dSignificant level of P < .01.
eSignificant level of P < .001.
fOnly factors that met the entry criteria of P < .15 in the univariate analysis were included in the multivariable logistic regression model.
gRespond level for the characteristic was not associated with the theme.
hOthers include American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander and Asian.
iLanguage(s) used by providers in providing HIV-related medical care to patients; other languages include French, German, Urdu, and so on.
Physicians who provided care for over 100 patients monthly (66.7%) and reported having sufficient time to provide HIV care to their patient (83.3%) were significantly associated with citing acceptance concerns as reason for the delay in ART initiation for clinically eligible patients. When the 3 characteristics that met the inclusion criteria were subjected to multivariable modeling, the results indicate that providers who provided medical care for more than 100 patients monthly were 10 times (aOR: 10.36, 95% CI: 1.42-22.7; P = .019) more likely than the referent (1-50 patients/month) to encounter acceptance concerns in their practice as reason for delaying ART initiation (R 2 = .24; P = .039).
Furthermore, our analysis noted significant variations in structural concerns associated with providers’ professions (P = .035) and referrals for ART initiation (P = .035). The majority of providers (81.8%) reported that they delayed ART due to structural barriers including lack of insurance/medical cost, inconsistent access to medications, and poor support system/unstable housing/transportation. However, multivariable modeling of this theme indicated that none of the providers’ demographic, practice, and medical care characteristics were significant predictors (R 2 = .03; P = .682) of structural concerns cited as reason for delaying ART in clinically eligible HIV-positive patients in Houston (Table 3).
Discussion
Antiretroviral therapy for the treatment of HIV infection has improved steadily over the past decade, offering more potent and effective medication, dosing convenience, and better-tolerated combinations. 34 Similarly, the US treatment guidelines have evolved over the years and now recommend ART for all HIV-infected individuals regardless of CD4 count. 17 –19 Despite this, providers may delay recommending ART to clinically eligible patients because of concerns that patients will be unable to benefit from or adhere to ART. 35 –37 Our study identified adherence, acceptance, and structural concerns as the 3 main nonclinical impediments that would cause providers in Houston, Texas to delay ART initiation for clinically eligible patients. Approximately 43% of the providers in our study identified adherence concerns associated with a chaotic/unstable lifestyle, appointment adherence, substance abuse, and mental health issues as reasons for delaying ART. Similarly, at the national level, more than two-thirds of providers cited concerns about patient adherence as reasons to delay ART initiation. 16,35 This is consistent with the current guidelines, which strongly recommend that barriers to patient adherence be addressed before prescribing ART, and on an ongoing basis after ART initiation, 17 –19 to avoid treatment failure and viral resistance. 20–21 Achieving adherence to ART is a critical determinant of long-term health outcome in HIV-infected patients. Although an increasing number of interventions have proven effective in improving adherence to ART, 38,39 the challenge for treatment teams is to select the techniques that best fit each patient and patient population, based on available resources and the treatment setting. 18 Our study revealed that clinically eligible patients who were black/African American experienced more systemic delays in the initiation of ART than Whites and Hispanics/Latinos. Generally, it’s been reported that Blacks/African Americans and Hispanics often decline ART because they believe they lack the necessary skills to adhere to ART regimens. 40,41 Despite patients’ attitudes, it is important that HMCPs continue to educate them on the potential individual and public health benefits of ART and the importance of adherence.
Our study noted that providers who cited adherence concerns varied by race/ethnicity, experience, and ART referral status, while multivariable analysis indicated that Hispanic/Latino providers were less likely to encounter adherence barriers as reasons to delay ART initiation. In contrast, providers with greater HIV care experience (6-10 years) were more likely than those with less than 5 years’ experience to delay ART due to adherence concerns. This finding is consistent with an earlier study that states that clinician experience and practice setting, rather than degree type, are important correlates of ART prescribing behavior. 42 Previous studies suggest that providers are less likely to prescribe ART in some key populations that include people who inject drugs, 42,43 released prisoners, and those lacking social support 43 or if they believe that addiction or homelessness contribute to social instability and will interfere with ART adherence. 14,16 However, current practicing providers may be more willing to prescribe ART to patients about whom they have adherence, acceptance, or structural concerns compared to the providers that we surveyed in 2009. This follows the change in treatment guidelines that recommends ART for all individuals with HIV, regardless of CD4 T lymphocyte cell count, to reduce the morbidity and mortality associated with HIV infection and to prevent HIV transmission. 17 –19 Studies conducted between 2013 and 2014 have shown increased change in attitudes toward universal prescribing of ART among HIV clinicians, with estimates of 71% reported from the MMP Provider Survey in the United States 44 and 87% from the survey of infectious disease physicians in the US and Canadian Emerging Infections Network. 45
About 30% of the providers in Houston cited acceptance concerns related to patients’ denial, fear and lack of ART knowledge, refusal, and lack of readiness to commit to regimen as reasons to delay ART initiation. Our findings support earlier reports where patients’ lack of readiness to commit to a complex regimen, fear of side effects, low levels of HIV knowledge, and largely negative attitudes toward ART have impeded their acceptance and the providers’ decision to initiate ART. 16,35 –37,46,47 Consequently, there seems to be a number of attitudes and beliefs associated with greater readiness, including higher levels of trust in one’s provider, self-efficacy, outcome expectancies, perceived personal need for ART, and positive perceived internal norms (how one feels about others taking ART). 47 These suggest that attitudes toward ART are complex and multifaceted, and that to improve readiness for ART and ART uptake, individual and social characteristics and the various aspects of ART beliefs must be considered together. 35,36,47 Among patients who are receiving HIV care, lower acceptance of ART has been associated with concerns about side effects, mistrust of medications and health-care providers, perceived effect of medications on quality of life, and a preference for alternative medicine and self-care. 34 –37,42,46 –48 Although additional work may be helpful to understand what motivates patients to take ART, particularly when they are healthy, 16 there is lack of evidence that readiness predicts future adherence. 48
Structural barriers are aspects of the larger external environment that limit individuals’ options. 49 None of the provider and practice characteristics were significant predictors of structural concerns cited by them, despite the association of the theme with provider profession and referral status for delayed ART initiation. However, lack of insurance/medical cost, inconsistent access to medication, and poor social support/unstable housing/transportation were cited as the common structural concerns for delaying ART initiation for clinically eligible patients. Past research has similarly identified structural barriers that impede optimal engagement in HIV care as difficulties they experience in navigating the health-care system and lack of insurance 50 and financial and transportation challenges. 51 Theoretically, these barriers work together synergistically to reduce motivation to engage in HIV care and/or initiate ART. Freeman and others in their study articulated the deep, complex, and systemic structural underpinnings of psychosocial barriers to ART and their impact on individual-level health decisions and behaviors among PLWH. 49
Limitations and Strengths of Study
The findings from our study should be interpreted with several important limitations in mind. Firstly, the study was based on data obtained before the US HIV treatment guidelines were updated in March 2012 17 –19 and before the HIV Prevention Trial Network 052 trial work was first published, 52 showing the prevention of transmission as a benefit to ART use (a potential population-level benefit beyond the individual-level benefit for both HIV-infected persons and their uninfected sexual partners) and the advent of more tolerable single-tablet regimens. Whereas providers’ practices and awareness have evolved since the new guidelines leading to initiation of ART for a higher proportion of their patients, it does not necessarily preclude providers from considering patient adherence or acceptance when making these decisions. 16 –19 Secondly, while the practitioner survey participation rate of 45% was considered low and may not be representative of the providers in Houston/Harris County, Texas, it was, however, higher than the 42% to 43% obtained for other HIV care provider-related surveys at the national level. 16,25,42 Thirdly, although probability proportional to size sampling method was used to select participating facilities, it was not possible to weight the providers’ self-reported responses to the survey questions because of the small sample size. Thus, our findings may not be generalizable to all HIV care providers in Houston/Harris County, Texas. Finally, the reasons cited by providers in our study were commonly reported, 16 implying that these issues are common, although possibly affecting few patients, since most patients sampled through MMP were prescribed ART. 53
Despite these limitations, our study has some important strengths. Our sample was drawn from a population-based frame that includes providers from several medical facilities with diverse provider demographics and practice characteristics, thus giving us confidence in our findings. Unlike previous studies, 16,42,48 our study provides proportional estimates of the clinically eligible patients in each subpopulation impacted by providers’ concerns for delaying ART initiation in addition to ranking of the subthemes. The current study also provides evidence that providers’ decisions to withhold ART varied significantly by patient race/ethnicity and major risk category. This information could be used to develop targeted interventions to improve patients’ readiness for ART and ART uptake. Findings from this study suggest that educating providers and monitoring their prescribing behaviors, to align clinical practice with the current US HIV treatment guidelines, could lead to higher rates of ART coverage for clinically eligible HIV-infected patients and subsequent reduction in the spread of HIV infection.
Conclusions
Findings from our study indicate that reasons given by HMCPs for delaying ART initiation were consistent with standard treatment guidelines, 17 –19 with significant variations noted along racial/ethnic and major risk category lines—a clear reflection of the gaps in engagement along the HIV care continuum. 43,49,54 Although treatment guidelines can identify some parameters of high-quality care, they cannot be substituted for sound clinical judgment. 18 Consequently, our findings underscore the importance of strengthening monitoring and timely intervention to address patient- and structural-level barriers that may cause systemic delays in ART initiation. According to Beer et al, 16 these barriers may become even more prevalent due to current universal ART prescription with resultant increase in the number of patients with less motivation to take ART and decreased structural barriers to medication coverage following transformation of the US health care system. Hence, multilevel strategies to address patient barriers to taking ART are most likely to be effective.
The findings that provider and practice characteristics were associated with reasons for delaying ART initiation provide important information that can be used to direct appropriate training and education for providers to address specific barriers among their patients. These resources should also target the treatment of substance abuse and mental illness to improve patients’ readiness for ART initiation and commitment to adherence. Providers should be encouraged to offer individualized treatment with patient involvement in decision-making to address the major nonclinical barriers identified in the current study. Following the change in US HIV treatment guidelines and the evolving provider practices, the findings of this study can be used to establish a baseline for the assessment of future potential disparities in systemic delays in ART initiation for clinically eligible patients. These results support the use of ART treatment as part of public health strategy to reduce the spread of HIV infection.
Footnotes
Authors’ Note
O.M. conceived and designed the study, conducted the data analysis, interpreted the results, prepared the initial draft manuscript, and participated in the critical review and revision of the article. M.R.-B., K.J.V., M.M., F.T., N.B., and J.W. interpreted the study findings and participated in the critical review of the article for important intellectual content concerning their respective areas of specialty. R.A. and E.J.E. played advisory roles in all aspects of the study and participated in the critical review of the article. All authors read and approved the final version of the article for publication. The CDC conceived the provider survey in 2009 as part of the Medical Monitoring Project, developed associated materials including data collection instrument, and provided oversight on the survey implementation in Houston/Harris County, Texas and other participating sites. The findings and conclusions of this article are solely the responsibility of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention or the Houston Health Department.
Acknowledgments
The authors would like to thank the HMCPs who participated in this survey, the MMP staff, and members of the Community Advisory Board and Provider Advisory Board in Houston project area; the Houston Health Department; and members of the Clinical Outcomes Team in CDC’s Behavioral and Clinical Surveillance Branch of the Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Medical monitoring Project (MMP) 2009 Providers’ Survey was supported by the Centers for Disease Control and Prevention (CDC) under the Cooperative agreement number PS09-937.