
Abstract
In the United States, a considerable number of people diagnosed with HIV are not receiving HIV medical care due to some barriers. Using data from the Medical Monitoring Project survey of HIV medical care providers in Houston/Harris County, Texas, we assessed the HIV medical care providers’ perspectives of the system and patient barriers to HIV care experienced by people living with HIV/AIDS (PLWHA). The study findings indicate that of the 14 HIV care barriers identified, only 1 system barrier and 7 patient barriers were considered of significant (P ≤ .05) importance, with the proportion of HIV medical care providers’ agreement to these barriers ranging from 73.9% (cost of health care) to 100% (lack of social support systems and drug abuse problems). Providers’ perception of important system and patient barriers varied significantly (P ≤ .05) by profession, race/ethnicity, and years of experience in HIV care. To improve access to and for consistent engagement in HIV care, effective intervention programs are needed to address the barriers identified especially in the context of the new health care delivery system.
Introduction
At the end of 2010, 1.1 million people were living with HIV in the United States. 1 Advances in antiretroviral therapy (ART) have resulted in increased survival and a better quality of life for persons living with HIV. 2 However, effective use of ART and viral suppression requires entry into HIV medical care, retention in care, and adherence to ART regimens. 3 Earlier entry into and retention in HIV care has been shown to reduce the risk of developing HIV opportunistic illnesses, 4 increase survival rates, 5 improve access to supportive services, 6 and improve overall quality of life. 7
Over 20 000 people in the Houston metropolitan statistical area (MSA) are living with HIV and over 1000 persons are diagnosed each year. 8 Houston ranks 12th nationally among MSAs for HIV cases 9 and 1st in the state of Texas for number of people living with the disease. 10 In the Houston area, of the people living with HIV, an estimated 5855 (27%) are not in care. 10 Several recent studies have shown that approximately 50% of the individuals who are aware of their HIV serostatus and who have been linked to care continue to be actively engaged in care. 11 –14 The remaining half are in care intermittently; some will come for a few visits and then are lost for long periods of time, which is likely to affect ART adherence.
One goal of National HIV/AIDS Strategy (NHAS) for the United States is to increase the number of patients living with HIV who are in continuous care and regularly seeing a health care provider to 80%. 15 However, numerous barriers exist that can adversely affect care access. Several system and patient-related barriers to HIV medical care and treatment have been identified in the literature. Some of the barriers relate to the health care structure or system and include negative perceptions of the health care system, 16,17 longer wait time for appointments, 18 lack of flexibility in clinic hours to accommodate work schedules, 19 unmet needs for child care, 19,20 lack of access to a provider with expertise in treating HIV, 3 strained patient–provider relationship, 21,22 patient concerns about privacy, 23,24 mandatory insurance coverage, 25,26 and multiple funding sources with variable eligibility criteria, 3 which causes many individuals to shift in and out of eligibility for HIV care. At the patient level, some of the barriers that prevent persons with HIV from utilizing HIV medical care include mental health issues and drug addictions, 27 –30 negative health beliefs about getting care, 31 perception about medical coverage, 25,26 HIV stigma, 3,16 limited social support, 26,32 unstable housing, 33,34 transportation, 20 incarceration, undocumented immigrant status, 2 and avoidance and denial of HIV status. 23,24,28 All of these issues influence entry, engagement, and retention in HIV care. The subject of accessing adequate HIV care and improvement in health outcomes for persons with HIV has become even more important, given NHAS goals. 15 It is important to identify effective prevention strategies that eliminate barriers and facilitate entry into and utilization of HIV medical care for persons living with HIV. 35
The HIV medical care providers are considered a critical link between the health care system and the patient. Consequently, they are in a unique position to not only observe the health care system barriers that patients face in accessing HIV medical care but also have the tendency to develop perspectives with regard to the individual-level barriers that prevent their patients from benefiting from the medical resources at their disposal. Although previous studies have examined the perceptions of barriers to care from the patient’s perspective, less is known about HIV medical care provider’s perceptions of barriers to care for their patients. The barriers identified by providers may truly represent the challenges faced by persons living with HIV who access care. We evaluate HIV medical care providers’ perceptions of the important barriers to care experienced by people living with HIV/AIDS in Houston/Harris County, Texas, and identify providers’ characteristics that may be associated with their perceptions.
Methods
Survey Design and Population
Data for this study were collected as part of the US Centers for Disease Control and Prevention’s (CDC’s) Medical Monitoring Project (MMP) Provider Survey, a survey administered to a nationally representative sample of HIV care providers who were selected to participate in MMP. Medical Monitoring Project is an ongoing surveillance system that collects information on the behavioral and clinical characteristics of adults ≥18 years of age receiving medical care for HIV infection in the United States and Puerto Rico. Information on MMP and the associated sampling method has been described previously 36 –38 ; and a detailed description of the MMP Provider Survey has been presented previously. 39,40
The Houston/Harris County component of the MMP Provider Survey data is presented in this study. The survey was conducted in Houston/Harris County from June through September 2009 in collaboration with the CDC. The survey population consisted of a subsample of HIV care providers from 13 outpatient facilities in Houston/Harris County that participated in the 2007 MMP data collection cycle. HIV care providers eligible for this survey included physicians, physician assistants, or nurse practitioners working in the MMP-sampled facilities/providers who have provided care to, ordered T-lymphocyte (CD4) or HIV viral load testing for, and/or prescribed antiretroviral medication to HIV-infected adults ≥18 years of age. Interns, residents, fellows, and others in training programs were not eligible. Providers who obtained CD4 counts and HIV viral loads only for referral purposes or provided ART refill prescriptions but did not play a more active role in managing their patients’ HIV infection were not eligible to participate in the survey.
Data Collection and Measures
A total of 51 questionnaire packets were mailed to eligible HIV care providers within the 13 participating facilities in the Houston project area. The total design method 41,42 was used to follow-up with nonresponders. The process involved following up with nonresponders after 1 week and at 3 and 7 weeks following the initial mailing. Twenty-three HIV providers completed the survey at a response rate of 45%. The survey took approximately 20 minutes to complete, and participants were offered a small monetary incentive in the form of a gift card.
The survey instrument consisted of 35 main items and assessed the HIV care providers’ demographic and medical practice characteristics. Based on the literature, 16 –32,43 a total of 14 barriers were identified as significant barriers to gaining access to HIV care by persons living with HIV. Seven were system barriers related to clinic characteristics or services and include: lack of child care at facility/clinic (LCF), inconvenient facility/clinic hours (IFH) and location (IFL), lack of translation services (LTS), cost of HIV care (CHC), no insurance coverage (NIC), and length of time to schedule appointments (LSA). Seven were patient-related barriers and include: transportation problems (TRP), culturally based health beliefs and behaviors (CHB), inability of patients to understand medical instructions (IMI), lack of social support systems (LSS), mental health problems (MHP), drug abuse problems (DAP), and alcohol abuse problems (AAP).
To determine how HIV medical care providers perceived these barriers experienced by their patients, they were asked to “indicate the important barriers experienced by HIV-infected persons in obtaining HIV care at your facility/clinic.” These items were measured on a 4-point scale as 1 (not important), 2 (slightly important), 3 (moderately important), or 4 (very important). Independent variables assessed were the race/ethnicity of HIV medical care providers, facility type, gender of provider, provider’s profession (eg, physician, physician assistant, or nurse practitioner), age of provider, provider’s years of experience, number of patients seen by provider per month, self-assessed knowledge of HIV care and treatment, medical specialty, professional certification, and language used in providing medical care to patients.
Data Management and Statistical Analysis
Prior to analyses, the data obtained were subjected to various levels of management including categorization of quantitative variables and recategorization of existing qualitative variables, where applicable. Participating providers/facilities were grouped into “public” or “private.” Provider age was classified into 2 groups as 36 to 45 and ≥46 years. The number of patients to whom the HIV care providers provided care per month was categorized as 1 to 50 patients (low), 51 to 100 patients (medium), and >100 patients (high).
The outcomes of interest were the perceptions by HIV medical care providers of the system and patient barriers to care faced by patients in their practice as measured by the 7 system and 7 patient-related barriers. Each of the barriers was originally evaluated using a 4-point Likert-type scale, as 1 = not important; 2 = slightly important; 3 = moderately important; and 4 = very important. However, for purposes of data analysis, the original categories not important and slightly important were combined into 1 category with a value of 0. Similarly, the original categories moderately important and very important were combined into 1 category with a value of 1. Therefore, the barriers were collapsed into dichotomous (0, 1) variables with a value of 1 corresponding to a belief that a barrier was important and 0 to a belief that it was not important. All subsequent analyses used this binary coding to represent the system and patient barriers to HIV care.
We used the chi-square test to determine whether the proportional distribution of the HIV medical care providers’ characteristics differed significantly. We also used the chi-square test to evaluate the HIV medical care providers’ perception of the level of importance of each of the 14 identified system and patient barriers. Based on the outcomes of the preliminary analysis, we conducted bivariate analysis to determine which providers’ characteristics (HIV medical care providers’ profession, race/ethnicity, and years of experience in HIV care) were associated with the important system and patient barriers to HIV care. Because of the size of the subgroups, HIV medical care providers’ race/ethnicity and years of experience in HIV care were further regrouped as follows: race/ethnicity (white, non-Hispanic or Latino versus minority races-comprising blacks or African Americans, non-Hispanic or Latino; Hispanics/Latinos (ethnicity), Asians, non-Hispanic or Latino; Native Hawaiian or Other Pacific Islander, non-Hispanic or Latino; and American Indian or Alaska Native, non-Hispanic or Latino) and years of experience in HIV care (<10 versus 10+ years), to obtain dichotomous categories of predictor variables. We conducted multivariate logistic regression analyses to model HIV medical care providers’ perception of system and patient barriers as important and to simultaneously adjust for any potential confounders due to bias. Estimates of P value, adjusted odds ratio (AOR), 95% confidence interval (CI), and coefficient of determination (r2) were obtained as outputs. Furthermore, Spearman correlation analysis was used to determine the form of associations that exist among the system and patient barriers identified as important. All tests performed were 2 tailed, with a P value of .05 used as the statistical significance level. Data management and statistical analyses were conducted using SAS statistical software version 9.2 (SAS Institute, Cary, North Carolina).
Ethical Considerations
Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (NCHHSTP) has determined that MMP is public health surveillance and is considered a nonresearch activity used for disease control program or policy purposes. Given the nonresearch determination, it is not subject to human subjects regulations including federal institutional review board (IRB). As an amendment to MMP, the MMP Provider Survey is covered under the same nonresearch determination. No local IRB was required for the Houston project area. All data collection was Health Insurance Portability and Accountability Act (HIPAA) compliant.
Results
The sociodemographic and medical practice characteristics of HIV care providers in the study population are shown in Table 1. The majority of the HIV care providers were physicians (73.9%), with 26.1% representing other HIV care professional (physician assistants and nurse practitioners). Most worked in publicly funded settings (56.5%) such as community health centers and 43.5% worked in private practice. The mean age of the HIV care providers who completed the survey was 46.7 (standard deviation [SD] = 7.39) years, with 47.8% 36 to 45 years and 52.2% ≥46 years. Slightly over half of the providers were white (52.2%). Black and Hispanic providers were equally represented (17.4% in both groups). Almost all (91.3%) HIV care providers had 6 years or more of clinical experience, with an average of 11.7 (SD: ±6.63) years of practice for the entire sample. The overall gender distribution of HIV medical care providers was 52.2% male and 47.8% female. Although all providers considered themselves to be knowledgeable in HIV treatment, 60.9% of them self-identified as board-certified infectious disease physicians. English language (47.8%) and a combination of English and other languages (52.1%) were used for providing HIV-related medical care to patients. Significant proportional differences were noted among participants by profession (P = .022), race/ethnicity (P = .027), and years of experience in HIV care (P = .032).
Sociodemographic and Medical Practice Characteristics of HIV Care Providers in Study Population.

Abbreviations: SD, standard deviation; χ2, chi-square; df, degree of freedom.
aPercentages may not add up exactly to 100% due to rounding.
bOther include American Indian or Alaska Native, non-Hispanic or Latino; Native Hawaiian or other Pacific Islander, non-Hispanic or Latino; and Asian, non-Hispanic or Latino.
cLanguage(s) used in providing HIV-related medical care to patients.
dSignificant level: P < .05.
Table 2 presents HIV medical care providers’ perceptions of system and patient barriers to HIV care among people living with HIV/AIDS (PLWHA) in Houston/Harris County, Texas. Of the 14 barriers identified, only 1 of the system barrier and all (7) of the patient barriers were statistically significant (P ≤ .05) in terms of importance, with the proportion of HIV medical care providers’ agreement to those ranging from 73.9% (CHC) to 100% (LSS and DAP). Although a large proportion of the providers perceived several system-related barriers such as IFH and location, lack of insurance coverage, LSA, LTS, and child care at facility/clinic as important, these factors failed to attain statistical significance (P > .05) when compared to providers who considered these barriers as unimportant. Conversely, the majority of providers had high agreement on the importance of the following barriers: TRP (87.0%), CHB of patients (82.6%), inability of patients to understand medical instructions (87.0%), and mental health and AAP (91.3%, respectively).
HIV Medical Care Providers’ Perceptions of System and Patient Barriers to HIV Care in Houston/Harris County, Texas.

Abbreviation: χ2, chi-square.
a df, degree of freedom = 1.
bResponse was constant, and no test statistic was computed.
cSignificant level: P < .05.
dSignificant level: P < .01.
eSignificant level: P < .001.
Bivariate analyses of the important system and patient barriers to HIV care by providers’ profession, race/ethnicity, and years of experience are given in Table 3. Providers identified the CHC as the single most important system barrier with significant proportional variations in agreement noted by profession (P = .029), race/ethnicity (P = .045), and years of experience in HIV care (P = .011). Significant differences existed in the proportion of providers who considered these patient barriers as important across the independent factors (Table 3). The majority of the HIV medical care providers who were physicians, whites, and those with 6 to 10 years’ experience tended to view these barriers as important to HIV care among PLWHA compared to other subgroups. Although CHB of patients, IMI, and MHP were identified as important patient barriers, those were not significantly associated with the HIV medical providers’ profession (P = .108; P = .074) and years of experience in HIV care (P = .066). The LSS and DAP were the 2 patient-related barriers that all the HIV medical care providers unanimously agreed (100%) are important barriers to HIV care among patients in Houston/Harris County, Texas.
Bivariate Analysis of Important System and Patient Barriers to HIV Care by Providers’ Profession, Race/Ethnicity and Years of Experience in HIV Care.a

Abbreviations: CHC, cost of HIV care; TRP, transportation problem; CHB, culturally based health beliefs and behaviors of patient; IMI, inability of patient to understand medical instructions; LSS, lack of social support systems; MHP, mental health problems; DAP, drug abuse problems; AAP, alcohol abuse problems.
aBased on HIV care providers who considered the identified system- and patient-level barriers to HIV care to be important; proportions are calculated within each barrier.
bResponse was constant, with all respondents identifying this barrier as important, and so, no test statistic was computed.
cOther include American Indian or Alaska Native, non-Hispanic or Latino; Native Hawaiian or other Pacific Islander, non-Hispanic or Latino; and Asian, non-Hispanic or Latino.
dSignificant level: P < .05.
eSignificant level: P < .01.
The results of the multivariable analysis are presented in Table 4. The coefficient of determination (r2) of the different models ranged from 0.18 (CHC) to 0.53 (IMI). Although the covariates in the model were poor determinants of CHC (r2 = .18), physicians and practitioners who had less than 10 years’ experience in HIV care were approximately 2 (AOR = 2.16; 95% CI: 0.24–19.27) and 3 times (AOR = 2.78; 95% CI: 0.35–22.32) more likely than others to perceive this barrier as important, respectively. HIV medical care providers who were whites were 25% more likely than those who were of minority races to perceive CHC as important system barrier (AOR = 1.25; 95% CI: 0.18–8.64). HIV care providers who were white were approximately 7 times more likely than the minority races (AOR = 6.60; 95% CI: 0.44–7.96) to consider CHB of patient as important barrier. Physicians and HIV care providers who were white were both 4 times (AOR = 4.00; 95% CI: 0.23–27.48) more likely than their respective reference groups (other health care professional and minority races) to consider transportation (TRP) as barrier to HIV care (r2 = .43). The independent variables in the model for IMI predicted 53% of the outcome, with whites being significantly (P < .01) more likely than other races (AOR = 1.38; 95% CI: 0.96–1.98); and providers with <10 years of HIV care experience being 3 times more likely than those with 10+ years’ experience to perceive this factor as important barrier to HIV care, respectively. HIV medical care providers who were physicians were about 4 times (AOR = 3.82; 95% CI: 0.14–10.41) more likely than other HIV care professionals to consider both MHP and AAP as important barriers to HIV care among HIV-positive patients in Houston/Harris County, Texas. Similarly, providers with <10 years of HIV care experience were 57% (AOR = 1.57; 95% CI: 0.61–14.53) more likely than the reference subpopulation (10+ years) to perceive both MHP and AAP as important barriers. Thus, providers’ profession, race/ethnicity, and years of HIV care experience significantly predicted 34% of both MHP and AAP in the models. However, the wide CIs for some of the odds ratio estimates call for caution in their interpretations.
Multivariate Logistic Regression Model Assessing the Odds of Perception of System and Patient Barriers as Important by HIV Medical Care Providers.

Abbreviations: CHC, cost of HIV care; TRP, transportation problem; CHB, culturally based health beliefs and behaviors of patient; IMI, inability of patient to understand medical instructions; MHP, mental health problems; AAP, alcohol abuse problems; ref, referent; AOR, adjusted odds ratio; CI, confidence interval.
aMinority races include blacks or African Americans, non-Hispanic or Latino; Native Hawaiian or Other Pacific Islander, non-Hispanic or Latino; American Indian or Alaska Native, non-Hispanic or Latino; Asian, non-Hispanic or Latino; and Hispanic or Latino.
bSignificant level: P < .05.
cSignificant level: P < .01.
dSignificant level: P < .001.
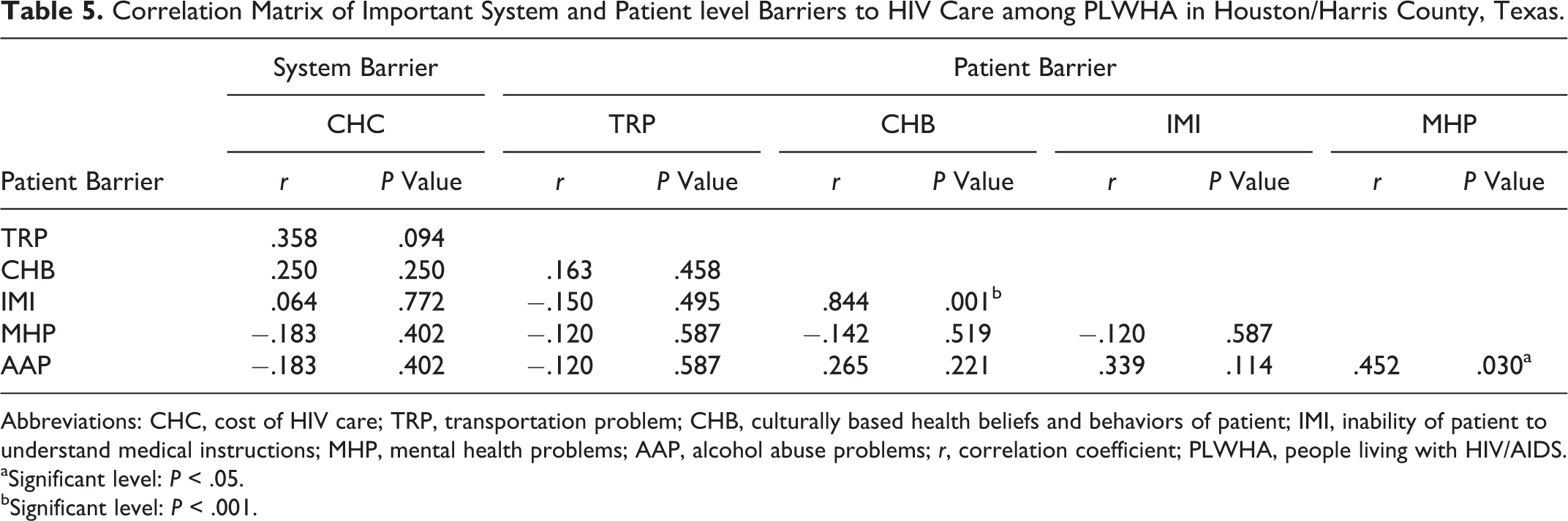
Table 5 shows the correlation matrix of important system and patient levels barriers to appropriate HIV care among PLWHA. Although both negative and positive correlations existed across the barriers, they were mainly not statistically significant (P > .05). However, significantly high and moderate positive relationships were observed between CHB and IMI (r = .844, P = .001) and between AAP and MHP (r = .452, P = .030), respectively. Transportation issues were negatively and significantly correlated with the number of patients seen at HIV medical care providers’ clinics during a typical month (r = −.480, P = .020; result not presented).
Correlation Matrix of Important System and Patient level Barriers to HIV Care among PLWHA in Houston/Harris County, Texas.
Abbreviations: CHC, cost of HIV care; TRP, transportation problem; CHB, culturally based health beliefs and behaviors of patient; IMI, inability of patient to understand medical instructions; MHP, mental health problems; AAP, alcohol abuse problems; r, correlation coefficient; PLWHA, people living with HIV/AIDS.
aSignificant level: P < .05.
bSignificant level: P < .001.
Discussion
HIV care and treatment involves a commitment to ongoing visits with health care providers, CD4 and viral load testing and prescription of ART. With recommended care and treatment, patients can reduce their viral load, protect their health, enjoy a long and healthy life, and reduce the potential of transmitting the virus to others. 2 –7 Our study identified one system and seven patient-related barriers important to HIV care. The sociodemographic and medical practice characteristic of providers in the current study has been previously described in detail by Mgbere et al. 40 This study noted that race/ethnicity of the providers as well as profession of the care providers and years of experience in HIV care were influential factors that determined the perception of barriers experienced by patients in obtaining HIV care in Houston/Harris County. Although the racial/ethnic demographic of HIV care providers has changed little, 30 the demographic of persons living with HIV has changed from predominantly white MSM population to increasing racial/ethnic minorities patient populations. 30,40 This study reports that in general providers who were of minority races were less likely than white providers to perceive most of the identified barriers as important. However, within-gender effect of the associations between providers’ race/ethnicity and barriers perception status was not statistically significant.
Almost three-fourths of the providers cited the CHC as the most important system barrier hindering patients from receiving adequate HIV care and also putting strain on the systems that serve them. Over time, the expenditures for HIV care, including public expenditures, have risen significantly and largely reflect growing numbers of people living with HIV in need of services and increasing health care costs, particularly for prescription drugs. For instance, the average annual CHC in the ART era was estimated to be US$19 912 (in 2006 dollars; US$23 000 in 2010 dollars) 44 and may be higher for those with more advanced HIV disease. The most recently published estimate of lifetime HIV treatment costs was US$367 134 (in 2009 dollars; US$379 668 in 2010 dollars). 45 Many people with HIV in care belong to low income group, with an estimated 46% having incomes less than US$10 000 a year and most (63%) being unemployed. 46 Because of these reasons, most people living with HIV/AIDS, in Houston/Harris County, Texas rely heavily on the public sector for their care.
We noted that several known system barriers such as IFH and location, lack of insurance coverage, LSA, LTS, and child care at the facility/clinic were identified as unimportant barriers to HIV care among patients. This may be associated with the fact that several of these support services are currently provided in many public and selected private clinics and local AIDS service organizations through the Ryan White HIV/AIDS Program, CDC, and Texas Department of State Health Services funds. 10 In contrast to our findings, several studies from the patient perspective have identified issues such as office waiting time, waiting lists, and difficulty scheduling care appointments, 18 IFH and location, 19,47 limited availability of child care at HIV clinics, 19,20 and lack of translational services, 30 as barriers to HIV care.
Lack of insurance coverage was not perceived by our study participants as an important barrier to care due, perhaps, to the various coverage mechanisms available to HIV-positive patients such as Medicaid, Medicare, and private insurance, and the Ryan White CARE Act, the Veterans Health Administration, and community health centers. 48 Those who are uninsured and underinsured also rely on an array of other safety net providers for care, including private free clinics. Although, many people qualify for public assistance programs; staying eligible for support remains a constant balancing act that has been exacerbated by patients’ misperception that health insurance coverage is necessary. 25,26,48
Our study identified TRP as an important patient barrier to HIV care among patients in Houston/Harris County, Texas. This finding is consistent with other reports. 20,30,47 It is also a reflection of the general public’s top concern and continuous call for improved mass transit system as the best way to address Houston metropolitan transportation issues. 49 Most underserved patients tend to rely on the current system to get to their care visits. However, this system has not been able to keep up with the city’s population growth and likely leads to missed appointments and/or postponement of care visits for patients. Increase in Houston/Harris County population has been partially attributed to hurricane Katrina in 2005, following the mass relocation of people from New Orleans to Houston/Harris County, Texas.
We found in our study that both CHB and IMI were identified as important barriers to HIV care and that these barriers were also positively correlated to each other. Encounters between HIV care providers and patients from different social or cultural backgrounds are becoming increasingly common in Houston/Harris County. This follows the transformation of the city into one of the most ethnically and culturally diverse cities in America. 49 For instance, many recent immigrants have limited proficiency in English, which presents challenges for the local health systems. Consequently, patients may have different thresholds for seeking care or expectations about their care, and unfamiliar beliefs that may influence whether or not they adhere to providers’ recommendations. 50 Recent reports suggest racial/ethnic minorities may have difficulty accessing appropriate, timely, high-quality care due to language barriers, and they may have differing perspectives on health and medical care. 51 Although clinicians strive to improve health outcomes and increase quality of life for every patient, some clinicians may lack the information to understand how culture influences clinical encounters and the skills to effectively bridge potential differences, 52 which are precursors of limited access to HIV care services and poor health outcomes. Culturally competent care requires health care providers to have knowledge of and comfort with cultures and beliefs that may be different from their own. Such knowledge may help shape providers values, beliefs, and behaviors and allow them to successfully guide immigrant populations through their unique challenges and the complex health care systems to obtain needed HIV care.
Mental health and AAP were perceived by more than 90% of the participating providers as major barriers to HIV care among people living with HIV/AIDS in Houston/Harris County. These findings are similar to those obtained in previous studies, 23,28,29,32,47 where poor mental health and substance abuse were reported to limit patients’ abilities to adhere to the continuum of HIV care. Given that as many as 50% of HIV-positive patients also have a psychiatric diagnosis and/or a substance use disorder, 53 there is a continued need for intervention programs aimed at encouraging patients to use available mental health and substance use treatment services. Studies show that decreasing alcohol use among HIV-positive patients not only reduces the medical and psychiatric consequences associated with alcohol consumption but also decreases other drug use and HIV transmission. 54
HIV care providers in our study also unanimously identified lack of social support and substance abuse as the major patient-related barriers to HIV care in Houston/Harris County, Texas. Social supports often have multiple levels of positive impact on patients and may motivate them to take the necessary steps to seek appropriate health care. Studies have shown that family, friends, and relatives are important sources of social support who can influence patient well-being and quality of life, 55,56 improve physical and psychological health outcomes, increase motivation for treatment, 57 promote self-care behavior, 55 and also prevention of transmission of HIV infection. 58 Similarly, HIV-positive patients using drugs or alcohol are less likely to be adherent to ART or responsive to health care appointments. They may also engage in impulsive and risky sexual behavior such as unprotected sex, which can transmit HIV infection to their partners. Since patients often have trust in their providers, it may be necessary for physicians to capitalize on this relationship to deliver prevention messages during encounters with HIV-positive patients who are using drugs, including referrals to substance use treatment services and support networks.
Overall, our study suggests that HIV care barriers in Houston/Harris County, Texas were generally perceived by providers to be mostly personal (patient-level) rather than structural-level barriers. The 2012 Houston EMA HIV/AIDS treatment cascade 10 indicates that of the 21 567 individuals diagnosed with HIV, 27% were not linked to care within 6 to 12 months of diagnosis, and about 49% were not engaged in regular HIV care. These outcomes are similar to those reported at the national level by Gardner et al. 11 Failure to initiate timely HIV care after diagnosis and incomplete engagement in HIV care are common in the United States. Poor engagement in care has been associated with poor health outcomes, including the largest proportion of HIV-infected individuals with detectable viremia 11,12 and increased mortality 5,28 Similar to individuals with undiagnosed infection, HIV-infected individuals not engaged in care pose a greater risk of ongoing HIV transmission to others in the community. 59 Although, monitoring of both linkage to care and retention in care is very complex, it is important that any intervention initiative developed for PLWHA be patient centered and be carried out in collaboration with the HIV care providers, local health authority, and the community-based organizations (CBOs), providing HIV support services.
Study Limitations
There are some limitations associated with our study. First, the participation rate of 45% was considered low but is, however, higher than the 42% obtained for similar study at the national level. 36 Second, although we evaluated the perceptions of HIV medical care providers regarding the barriers to appropriate HIV care for people living with HIV/AIDS in Houston/Harris County, it is possible that some practitioners may have used their own patients as referents when answering some of the barrier questions. Third, it would have been very valuable to compare patients’ reports from the same practices with the provider survey; however, the study design did not permit data collection from patients. Despite these limitations, this study is the only known investigation that has attempted to evaluate the relationship between characteristics of HIV medical care providers and their perceptions of system and patient barriers to HIV care faced by PLWHA in Houston/Harris County, Texas. The findings of this study contribute significantly to the understanding of this less explored area of access to appropriate HIV care, especially in the context of the evolving new health care delivery system.
Conclusion
In pursuance of the NHAS goal of reducing or eliminating existing barriers to HIV care, 15 our study serves as the first step in the process by attempting to assess HIV care providers’ perspectives of potential system and patient-level barriers to HIV care in Houston/Harris County, Texas. Findings from our study indicate that multiple patient-level barriers and a single-system barrier were identified as major hindrances to HIV care utilization. This suggests that effective intervention efforts to address these barriers should be multilevel and patient centered and be jointly developed by HIV care providers, local health authority, and the CBOs. This approach could offer unique perspectives on how individual- and community-level behavior change may be effective in promoting access and sustained engagement in care and improved health outcomes of people living with HIV/AIDS. Since mental health, drug, and AAP were also identified by HIV care providers as barriers affecting patients’ access to HIV care, it may be important for providers to monitor patients regularly for signs of these problems and to immediately initiate interventions as necessary. Intervention programs linking primary medical care with treatment for abuse of alcohol and other drugs, HIV risk-reduction education, and psychiatric care have proven successful. 16,60 Also, it may be possible for underserved or disadvantaged HIV-positive patients to overcome behaviorally based barriers hindering access to care and retention, if the competing demands such as poverty, unemployment, housing need, and so on can be addressed by policy makers. Keeping HIV-infected patients connected to care should be a major health care and public health priority, especially as engagement in HIV care is increasingly recognized as a critical step in patient outcomes. 11 –14 In addition, multifaceted research on best practices to link and retain HIV-infected individuals in care is needed.
Footnotes
Acknowledgements
The authors would like to thank the HIV medical care providers who participated in this study, the MMP staff in Houston project area, the Centers for Disease Control and Prevention, and the Houston Department of Health and Human Services for various levels of support received during the data collection period.
Authors’ Note
OM contributed to the conception and design of study, conducted the data analysis and interpretation of the results, prepared the initial draft of the article, and participated in critical review of article; SK, TB, MR-B, MS, and JA interpreted the study findings and participated in the critical review of article for important intellectual contents concerning their respective areas of specialty; RA, EE, and ER played advisory roles in all aspects of the study and participated in the critical review of article; and all authors read and approved the final version of the article. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention. The CDC conceived the project, developed project-associated materials including data collection instrument, and provided oversight on the survey implementation in Houston/Harris County, Texas, and other participating sites.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Medical Monitoring Project (MMP) Providers’ Survey was supported by Centers for Disease Control and Prevention (CDC) under cooperative agreement number PS09-937.