
Abstract
This study evaluates the frequency and determinants of preventive care counseling by HIV medical care providers (HMCPs) during encounters with newly diagnosed and established HIV-infected patients. Data used were from a probability sample of HMCPs in Houston/Harris County, Texas, surveyed in 2009. Overall, HMCPs offered more preventive care counseling to newly diagnosed than the established patients (adjusted odds ratio [AOR] = 7.28; 95% confidence interval [CI] = 2.86-16.80). They were more likely to counsel newly diagnosed patients than the established ones on medication and adherence (AOR = 14.70; 95% CI = 1.24-24.94), HIV risk reduction (AOR = 5.91; 95% CI = 0.48-7.13), and disease screening (AOR = 7.20; 95% CI = 0.72-11.81). HIV medical care providers who were less than 45 years of age, infectious disease specialists, and had less than 30 minutes of encounter time were less likely to counsel patients regardless of the status. Our findings suggest the need for HMCPs to improve their preventive care counseling efforts, in order to help patients build skills for adopting and maintaining safe behavior that could assist in reducing the risk of HIV transmission.
Introduction
Despite increased prevalence of antiretroviral therapy (ART) use, HIV incidence has remained high in many communities, suggesting that prevention programs targeting only HIV-negative persons may be inadequate to curb the epidemic and emphasizing the need to address HIV prevention among HIV-positive persons. 1 A reference to HIV epidemiology profile in Houston/Harris County, Texas, indicates that between 2007 and 2012, an annual estimated HIV incidence of 1159 new cases (28.5/100 000 population) per year has been reported, 2 with an estimated 21 405 persons living with HIV infection in the Houston metropolitan statistical area (MSA) as of 2012. 3 The Houston MSA accounts for more than 30% of reported cases of HIV infection in the state of Texas 4 and ranks 12th in the nation among MSAs for persons living with HIV infection. 5
As people with HIV are living longer and healthier lives, their prevention needs are increasingly becoming prominent in studies and discussions of HIV prevention. These needs led to the incorporation of national prevention strategies into the medical care settings of person living with HIV. 6 Essential elements of the guidelines stipulate that HIV-infected patients should be screened for HIV-risk behaviors at least annually and should receive behavioral interventions at least twice annually.
Relatively little is known about the risk-reduction education practices of HIV care providers with their HIV-positive patients. Earlier studies showed that primary care physicians do not routinely assess or carry out HIV intervention on their patients regarding their risks for HIV infection. 7 –12 Data obtained from physicians in 4 US cities suggest that less than optimal HIV prevention counseling was being provided to both new and established patients. 9 In some of these studies, between 25% and 30% of HIV-positive patients reported that they have never discussed safer sex with their health care providers. 10,11 These findings corroborate with the outcome of a recent Medical Monitoring Project (MMP) study, where fewer than half of the patients were reported to have received prevention counseling from their health care providers during the preceding year. 13 These low percentages, especially among men who have sex with men, who account for most new HIV infections in the United States, 14 indicate a need for health care providers to deliver HIV prevention counseling services more consistently. Although many persons with HIV may modify their behavior to reduce their risk for transmitting HIV after learning about their infection, some still require ongoing prevention counseling services to change their risk behavior or to maintain the change. 15
Studies examining the efficacy of medical provider counseling have shown reductions in sexual risk behavior among specific groups of HIV-infected patients. 16 –18 Rudy et al 12 noted that low counseling by providers was associated with patient’s poor care-seeking behavior and reduced motivation to seek care. HIV care providers can greatly reduce patients’ risks for transmission of HIV to others by performing a brief screening for HIV transmission risk behaviors; communicating prevention messages; discussing sexual and drug-use behavior; positively reinforcing changes to safer behavior; referring patients for services such as substance abuse treatment; facilitating partner notification, counseling, and testing; and identifying and treating other sexually transmitted diseases (STDs). 6,19,20 By engaging patients in open discussions about the risks of HIV transmission, their current risk behaviors, and factors associated with increased risk, providers can begin to tailor risk-reduction strategies based on patients’ needs and desires. Given the multitude of health issues facing HIV-positive patients, many providers often feel that they have no time to engage patients in discussions about high-risk behavior. 9,21 Additionally, provider attitudes, particularly fatalism, 22 inconsistent behavioral counseling skills, 23 funding for staffing, and providers’ understanding of their roles and responsibility 21 have all been identified as barriers to providing HIV prevention counseling in clinical care settings.
Nevertheless, patient and community health depend on patient risk behaviors, which therefore must be assessed over the duration of the patient–provider relationship. Clinicians providing medical care to HIV-infected persons can play a key role in helping their patients reduce risk behaviors and maintain safer sex practices. They can do so with a modest level of effort, even in constrained practice settings. Medical visits provide a vital opportunity to reinforce HIV prevention messages, discuss sexual and drug-related risk behaviors, diagnose and treat other STDs, review the importance of medication adherence, and foster open communication between provider and patient. 24 To our knowledge, there is only one study 9 that has attempted to evaluate provider–reported practices and delivery of prevention counseling to both newly diagnosed and established HIV-positive patients in HIV medical care settings using separate indicators. The use of many separate indicators to assess preventive care counseling has made it difficult to determine the overall quality of care delivered to patients and providers’ actual performance in priority preventive care areas.
Our current research effort builds on the foundation of Metsch et al 9 and aims to evaluate the preventive care counseling by HIV medical care providers (HMCPs) using both single indicators and composite measures. Specifically, this study will assess the frequency and determinants of preventive care counseling by HMCPs in Houston/Harris County, Texas, during encounters with newly diagnosed and established HIV-positive patients.
Methods
Survey Participants
The survey participants consisted of medical care providers from 13 HIV care facilities in Houston/Harris County, Texas, who participated in the US Centers for Disease Control and Prevention (CDC) MMP Providers’ Survey. The survey was conducted in Houston/Harris County, Texas, from June through September 2009.
Recruitment and Data Collection
HMCPs eligible for this survey included physicians, physician assistants, or nurse practitioners at the MMP sampled facilities/providers who have provided care to, ordered CD4 or HIV viral load testing for, and/or prescribed ART to HIV-infected adults ≥18 years of age. Physicians who were interns, residents, fellows, and others in training programs were not eligible. Also, providers who obtained CD4 counts and HIV viral loads only for referral purposes or provided antiretroviral (ARV) refill prescriptions but did not play a more active role in managing their patients’ HIV infection were excluded from the sample.
Information on MMP sampling methodology has been described previously 25 –27 ; and a detailed description of the MMP providers’ survey procedures can be found in McNaghten et al 28 and Mgbere et al. 29 Prior to data collection, MMP-participating facilities were initially contacted for the names and contact information of eligible providers. A unique identification number was assigned to each provider based on a list of sequential ID numbers for each facility. Using the identification numbers, personalized recruitment packets containing a recruitment letter describing the purpose of the survey, information on how to access the survey online using the provider’s unique identification number, a paper copy of the survey with a postage-paid return envelope, and a small monetary incentive in the form of gift card were sent to the sampled HIV care providers. The survey required approximately 20 minutes to complete.
A total of 51 questionnaire packets were mailed to eligible HIV care providers within the 13 participating facilities in the Houston project area. A modified version of total design method 30,31 was used to follow-up on nonresponders. Reminder postcards were sent to all sampled providers 1 week after the initial mailing, and a replacement survey, a copy of the original recruitment letter, and a letter for nonresponders were sent to all providers who had not completed the survey at 3 and 7 weeks following the initial mailing. A total of 23 HIV providers completed the survey, resulting in a response rate of 45%.
Measures and Development of Preventive Care Counseling Indices
The survey instrument that consisted of 35 main items assessed the HIV care providers’ demographic and medical practice characteristics, including their perceptions of patient characteristics, attitudes and beliefs, barriers to providing optimal care, preventive care counseling practices, and familiarity and comfort with using current HIV/AIDS treatment guidelines. All independent variables used in this study were dichotomized to improve the accuracy and efficiency of estimates and composed of the following: patients’ status (newly diagnosed versus established), HIV care providers’ profession (physician versus other HIV care professionals), infectious disease board certification status (yes/no), provider age (<45 versus 45+ years), race/ethnicity (white, not Hispanic or Latino versus other races [minorities]—composed of blacks or African Americans, not Hispanic or Latino; Hispanics/Latinos [ethnicity], Asians, not Hispanic or Latino; Native Hawaiian or Other Pacific Islander, not Hispanic or Latino; American Indian or Alaska Native, not Hispanic or Latino), years of experience in HIV care (<10 versus 10+ years), patient encounter time (<30 versus 30+ minutes), sufficiency of encounter time with patients (yes/no), language of communication (English only versus English + other languages); and number of HIV-positive patients receiving care for in a month (<100 versus 100+).
The outcome variable of interest was the preventive care counseling practices of participating providers. HIV care providers were asked to indicate how often they counseled their patients using 20 identified preventive care measures/topics. The measures/topics covered items related to medication and adherence, risk-reduction counseling, mental health and substance use, disease screenings, and social and family support services. The frequency at which each provider counseled their patients using these items was coded on a 5-point Likert-type scale as always discuss, frequently discuss, sometimes discuss, almost never discuss, and never discuss. The questions were asked separately for newly diagnosed and established HIV-positive patients. For the purpose of analysis, the responses were collapsed into 2 main categories as always discuss (comprising always discuss and frequently discuss) and sometimes discuss (comprising sometimes discuss and almost never discuss). These 2 categories formed the basis for determining the frequency of delivery of preventive care counseling by HMCPs.
Using the scoring scheme that ranged from 4 (always discuss) to 1 (almost never discuss), the 20 preventive care counseling measures/topics were recoded and used to develop 6 composite counseling indices (CCIs) of performance such that a higher score indicated a provider’s likelihood to engage in preventive care counseling activities, while a lower score represented less likelihood to engage in preventive care counseling activities. The indicator variables were not transformed since they all had a common unit of measurement. However, to indicate their relative importance, differential weights based on conceptual rationale
32
were applied as follows: 0.250 for medication and adherence, risk reduction, mental health, and substance use indicators and 0.125 for disease screenings and support services. The weights summed up to 1.0. The weights were then multiplied by the actual performance values for each indicator and then summed to produce the composite score or index. In its simplest form, the CCIs take a linear form as follows:

The composite counseling units are represented by the following indices. Medication and adherence index used a 5-item scale that includes adherence with ARV regimen, adherence with opportunistic infection prophylaxis, how to take medicines, medicine-related side effects, and drug–drug interactions. Composite score ranged from 2.75 to 5.00, with a Cronbach α of .88 (95% confidence interval [CI] = 0.82-0.93). Risk-reduction counseling index, which measures HIV transmission risk-related counseling activities by providers, used 6-items, namely, risk reduction regarding HIV transmission, condom use, pregnancy or potential pregnancy with female patients, availability of partner counseling services, disclosure of HIV status to their partners, and pregnancy or potential pregnancy with female patients not on ART. Index values ranged from 2.25 to 6.00, with item’s internal consistency of .90 (95% CI = 0.84-0.94). Disease screening index was assessed using a 5-item scale that includes screening for sexually transmitted disease, hepatitis, tuberculosis, hepatitis (A and B) vaccination, and discussion about tuberculosis disease risk. The score ranged from 0.75 to 2.50, with acceptable reliability coefficient (Cronbach α = .91; 95% CI = 0.86-0.94). Mental health and substance use counseling index was evaluated using 2-item scale (mental health problems, including depression and substance use). Composite score for this subvariable ranged from 0.50 to 2.00, with Cronbach α of .80 (95% CI = 0.67-0.88). A 2-item scale made up the social and family support index (wellness—nutrition, exercise, etc, and family/social support), with a composite score range of 0.38 to 1.00 and Cronbach α coefficient of .64 (95% CI = 0.41-0.79). The overall preventive care counseling index of the study participants was made up of 5 subcomposite scales (20-item scale), with a score range of 7.50 to 16.50. This composite scale had good internal reliability, with a Cronbach α coefficient of .79 (95% CI = 0.68-0.87).
Statistical Analysis
To determine the independent associations between the frequency of delivery of preventive care counseling by HMCPs to newly diagnosed and established HIV-positive patients, chi-square test was conducted for the 20 identified preventive care measures and activities. Subsequently, the multi-items 6 CCIs developed were tested for internal consistency using Cronbach α coefficient. The general linear model univariate analysis of variance was initially used to assess the differences within the levels of each independent variable (demographic and medical care characteristics) on the 6 CCIs based on the mean values (and standard deviations) obtained for each dichotomized independent variable.
Following the outcome of this analysis, the independent variables were selected a priori and used as predictors in the multivariate logistic regression models, if they were statistically significant at P < .20 in the univariate analysis of variance. Covariates were tested for multicollinearity and were not considered a problem. A binary measure was defined for each index using the mean score as follows: mean score and above were given a measure of “1” (counseling patients/having more tendency to counsel patients) and those below the mean were given a measure of “0” (not counseling patients/having less tendency to counsel patients). The identified predictor variables, which varied for each index, were entered into the multivariate logistic regression models based on the binary preventive care counseling measures. This process allowed for simultaneous adjustment of any potential confounders due to bias and produced estimates of P value, adjusted odds ratio (AOR), and 95% CI. Model statistics for each index was evaluated using the pseudo R2 (Nagelkerke) and maximum likelihood ratio tests. First, the models were built for the overall sample, and later, the data were split into 2 subgroups to build overall preventive care counseling model for newly diagnosed and established HIV-positive patients. All tests performed were 2 tailed, with a probability value of .05 used as the statistical significance level. Data management and statistical analyses were conducted using SAS statistical software version 9.3 (SAS Institute, Cary, North Carolina).
Human Participant Protection
The US Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention has determined that MMP is public health surveillance and is considered a nonresearch activity used for disease control program or policy purposes. Given the nonresearch determination, it is not subject to human participants’ regulations including federal institutional review board (IRB). As an amendment to MMP, the MMP Provider Survey is covered under the same nonresearch determination. No local IRB was required for the Houston project area.
Results
Characteristics of HMCPs
The demographic and medical practice characteristics of participating
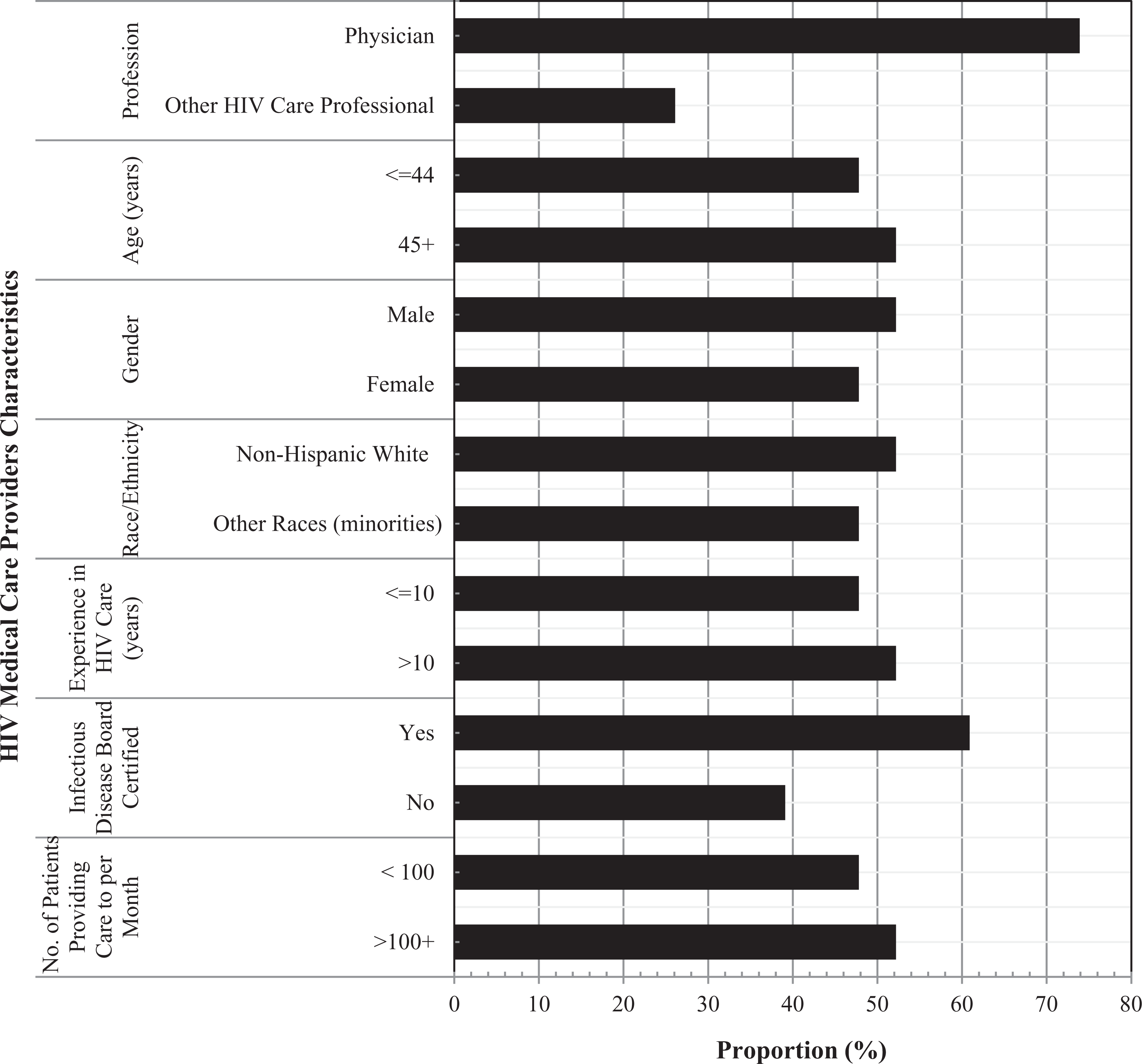
Characteristics of participating HMCPs.
Frequency of Delivery of Preventive Care Counseling
The frequency of delivery of preventive care counseling by HMCPs to newly diagnosed and established HIV-positive patients is presented in Table 1. In general, we noted significant variations in the provision of counseling services to the 2 groups of patients, with the majority of providers tending to always provide such services to newly diagnosed patients than to established ones. Preventive care counseling services were generally provided to established patients sometimes with the proportion of providers’ agreement ranging from 56.5% to 87.0% (P ≤ .05). Over 60% of HMCPs tend to always counsel newly diagnosed patients on HIV risk reduction and condom use compared to only 17.4% and 30.4% of them who agreed to always counseling the established patients for these measures. Also, more providers agreed to screening newly diagnosed patients for STDs always compared to the established ones (52.2% versus 13.0%; P < .01).
Frequency of Delivery of Preventive Care Counseling by HIV Medical Care Providers to Newly Diagnosed and Established HIV-Infected Patients.

Abbreviations: ART, antiretroviral therapy; OI, opportunistic infection.
aNewly diagnosed refers to a patient new to HIV care, someone who has not previously obtained HIV care, and not a patient new to one’s practice.
bEstablished patient refers to someone who has been seen at a facility/practice at least 1 prior occasion for HIV care.
cCompares the frequency of preventive care counseling on designated measures between newly diagnosed and established HIV-infected patients.
dIncludes participants whose response was almost never discussed.
eBetween HIV care group, df = 3.
fSignificant level P < .05.
gSignificant level P < .01.
hSignificant level P < .001.
Influence of Medical Care and Demographic Characteristics on Preventive Care Counseling
Table 2 presents the mean preventive care counseling domain-specific indices and standard deviations by medical care and demographic characteristics. The HMCPs recorded significantly higher mean preventive care CCIs for newly diagnosed patients compared to established ones, for overall (13.88 ± 1.75 versus 11.65 ± 2.26; P < .001), medication and adherence (4.61 ± 0.46 versus 3.91 ± 0.74; P < .001), risk reduction (4.89 ± 0.85 versus 4.00 ± 1.03; P < .01), and disease screening (2.03 ± 0.38 versus 1.66 ± 0.48; P < .01). Our findings also indicate that providers who were not board certified in infectious disease received significantly (P < .05) higher scores than those who were certified for the overall, risk-reduction and disease screening indices. Providers who were 45 years and older counseled their patients on HIV risk reduction more than those who were younger (4.76 ± 1.08 versus 4.10 ± 0.88; P < .05). Similarly, providers who had 30 minutes and more encounter time with their patients counseled them more frequently on HIV medication and adherence (P < .05) and risk reduction (P < .01) compared to those whose encounter time was less than 30 minutes. None of the characteristics considered in our study had any significant influence (P > .05) on mental health and substance use and support service CCIs.
Univariate Analysis of Variance Assessing the Effect of HMCPs Demographic and Medical Care Characteristics on Preventive Care CCIs of HIV-Positive Patients.

Abbreviation: SD, standard deviation.
aSignificant level P < .001.
bSignificant level P < .01.
cFactors within the preventive care CCIs that met P < .20 entry criteria for inclusion in the multivariate logistic regression models in Table 3.
dSignificant level P < .05.
Determinants of Preventive Care Counseling
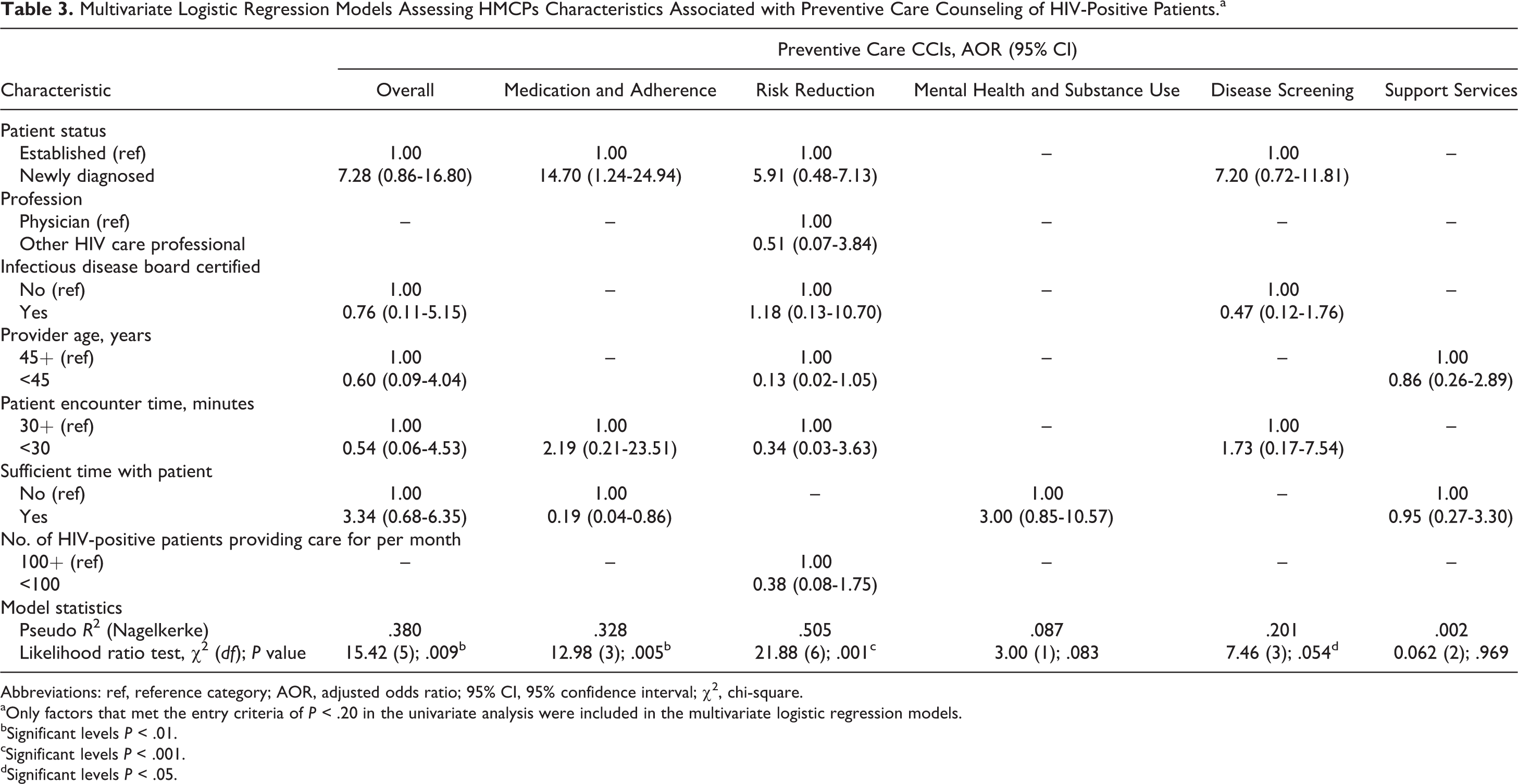
The multivariate logistic regression models assessing providers’ demographic and medical care characteristics associated with preventive care CCIs of HIV-positive patients are displayed in Table 3. Our results indicate that approximately 38% of the overall preventive care counseling index variation could be explained by patient status, providers’ infectious disease board certification status, age, encounter time, and sufficiency of time spent with patients during care visits. The newly diagnosed patients were 7 times (AOR = 7.28; 95% CI = 2.86-16.80) more likely than the established patients to be counseled by their providers. Those who believed that they had sufficient time to spend with their patients were 3 times (AOR = 3.34; 95% CI = 0.68-6.35) more likely to provide counseling services to their patients. In contrast, providers who were board certified in infectious disease, of age less than 45 years, and had encounter time less than 30 minutes were 24%, 40%, and 46% less likely to counsel patients, respectively. Providers were generally more likely to counsel newly diagnosed patients on medication and adherence (AOR = 14.70; 95% CI = 1.24-24.94), HIV risk reduction (AOR = 5.91; 95% CI = 0.48-7.13), and disease screening (AOR = 7.20; 95% CI = 0.72-11.81), compared to established ones. Six of the characteristics evaluated significantly (P < .001) determined 51% of the variation in HIV risk-reduction counseling index (Table 3). Providers who were board-certified infectious disease physicians were 18% (AOR = 1.18; 95% CI = 0.13-10.70) more likely to counsel patients on HIV risk reduction, while those who were nonphysicians were 49% less likely to counsel patients on HIV risk reduction. In contrast, we noted only 20% of the variation (R2 = .20; P < .05) in disease screening index was accounted for by providers’ infectious disease board certification status, patient encounter time, and patient status (newly diagnosed versus established).
Multivariate Logistic Regression Models Assessing HMCPs Characteristics Associated with Preventive Care Counseling of HIV-Positive Patients.a
Abbreviations: ref, reference category; AOR, adjusted odds ratio; 95% CI, 95% confidence interval; χ 2 , chi-square.
aOnly factors that met the entry criteria of P < .20 in the univariate analysis were included in the multivariate logistic regression models.
bSignificant levels P < .01.
cSignificant levels P < .001.
dSignificant levels P < .05.
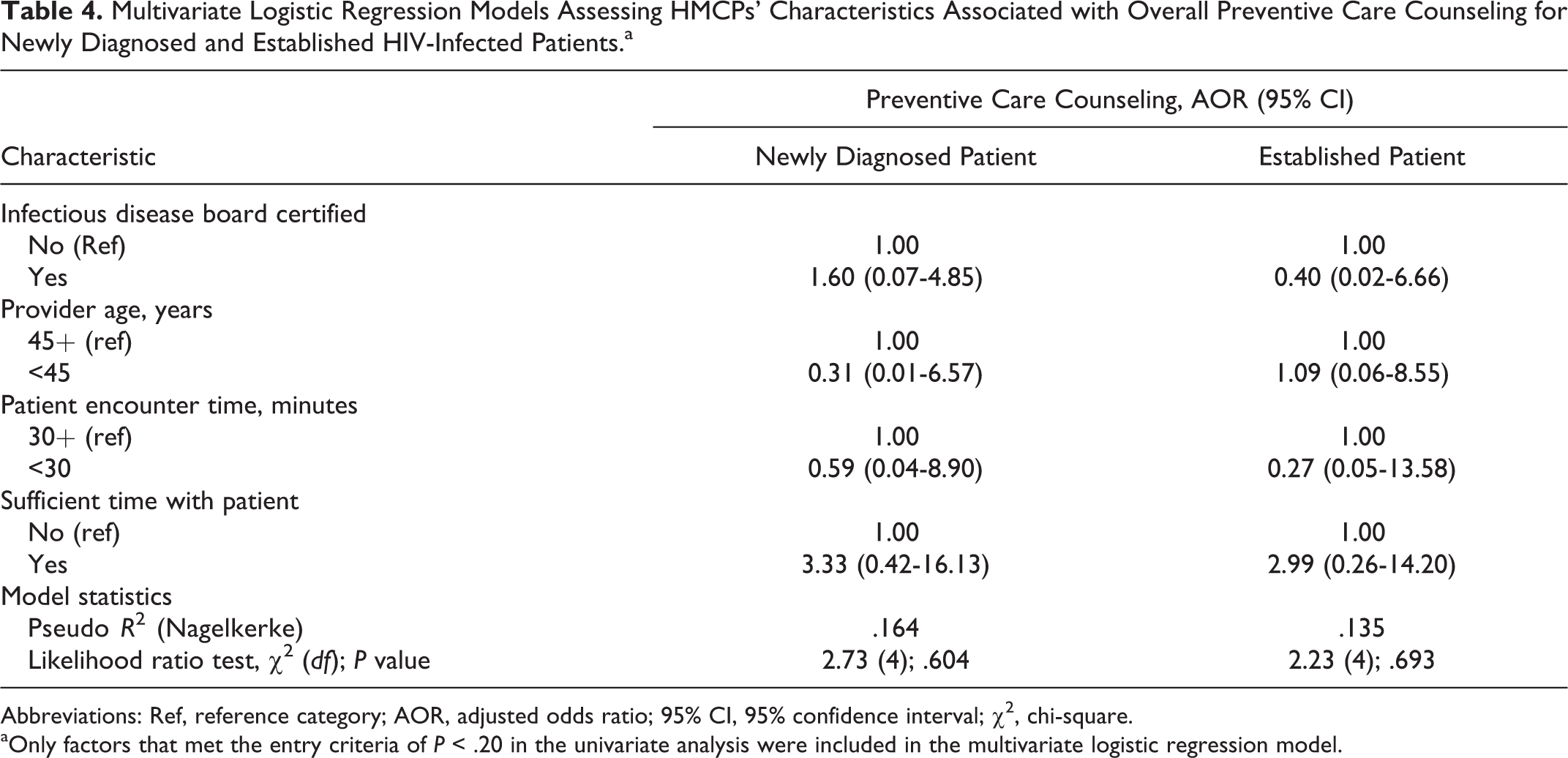
Table 4 presents the outcome of the by-group models of the independent factors for newly diagnosed and established patients. Providers who were infectious disease board certified were about twice (AOR = 1.60; 95% CI = 0.07-4.85) more likely to conduct preventive care counseling for newly diagnosed patients and 60% less likely to do so for established ones (AOR = 0.40; 95% CI = 0.02-6.66). The younger providers (<45 years) had an inclination to counseling established patients (AOR = 1.09; 95% CI = 0.06-8.55) compared to the newly diagnosed patients (AOR = 0.31; 95% CI = 0.01-6.57). Those who felt that they have sufficient time during care visits were 3 times more likely to counsel both newly diagnosed (AOR = 3.33; 95% CI = 0.42-16.13) and established patients (AOR = 2.99; 95% CI = 0.26-14.20). Although the independent variables made very little contributions (R2 = 16% versus 14%) to the outcome variable in the by-group analysis, the model’s fit was not statistically significant (P > .05).
Multivariate Logistic Regression Models Assessing HMCPs’ Characteristics Associated with Overall Preventive Care Counseling for Newly Diagnosed and Established HIV-Infected Patients.a
Abbreviations: Ref, reference category; AOR, adjusted odds ratio; 95% CI, 95% confidence interval; χ 2 , chi-square.
aOnly factors that met the entry criteria of P < .20 in the univariate analysis were included in the multivariate logistic regression model.
Discussion
Providing prevention interventions that reduce the risk of HIV transmission or acquisition of other STDs, in addition to HIV treatment and care for HIV-positive individuals are critical components of the US National HIV/AIDS Strategy. 33 Findings from our study indicate that more preventive care counseling was provided by HMCPs for newly diagnosed patients compared to the established patients. About 91% of HMCPs reported consistently discussing adherence to ART regimen with their newly diagnosed patients who were being prescribed ART. This proportion is higher than 88% 34 and 84% 35 reported by physicians for patients new to HIV care. Sixty-five percent of the HMCPs provided consistent HIV risk-reduction counseling to newly diagnosed compared to 30% that provided same service to the established patients. Although the use of condoms is known to reduce the risk of HIV infection, only 61% of the providers endorsed that they consistently counsel their newly diagnosed patients on condom use compared to 17% for established patients. Our finding suggests that less than optimal HIV risk-reduction counseling is being provided to established patients in Houston/Harris County and supports earlier reports. 9,13,35 –37
Only 13% of our participating providers reported consistently counseling established patients on STD risk reduction. This is particularly concerning because this activity is a preamble for determining high-risk sexual behaviors, possible exposure to other STDs, and the need for further testing of sexual partners. 34 Providers should strongly consider annual STD screening among all sexually active HIV-positive patients, and more frequently, if patients are at high risk for STD acquisition. Our finding points to the fact that a significant proportion of the HIV providers could benefit from additional training and education on screening HIV-infected patients for STDs. Lack of attention to HIV transmission behaviors during HIV care visits represents missed opportunity for delivery of prevention messages and, thus, have negative impact on prevention efforts. Although several barriers to provision of prevention counseling in clinical care settings have been identified, 9,21 –23 evidence-based guidelines recommend providing risk-reduction counseling to all HIV-infected patients during their routine clinic visits. 6,38,39
Higher domain-specific indices were recorded for newly diagnosed patients compared to established ones for overall, medication and adherence, risk reduction, and disease screening. When fitted into the multivariate regression models, these translated to HMCPs having higher odds of providing preventive care counseling to newly diagnosed patients than established patients based on the counseling domains. In general, provision of prevention care counseling by providers was determined by patients being newly diagnosed, and clinicians being nonboard certified in infectious disease, of age 45 years and above, having encounter time of 30 or more minutes, and considering the time spent with patients as sufficient. The finding that infectious disease specialists were less likely than other clinicians to provide preventive care counseling to their established patients is consistent with earlier report. 9 Physicians often try to address the multiple needs of their HIV-positive patients during a brief encounter. But time constraints tend to decrease infectious disease specialists’ focus on primary prevention. 9,21 Our findings, in part, may be associated with the fact that in some clinics, there may be dedicated health care professionals other than specialist or primary care provider responsible for the provision of preventive care services and/or case management. It is possible that some HMCPs may not see prevention as their responsibility and thus tend to focus on patient care rather than providing this important public health-related service. They believe that prevention counseling is better conducted by other allied health professionals. 40 Providers’ absence of perception of patients as being at risk, and lack of knowledge of risk behaviors, prevention or appropriate counseling techniques could also hamper preventive care counseling. 41 Medical care providers should recognize that risk is not static. As patients’ lives and circumstances change, so do their risk of transmitting HIV. Therefore, continuous screening and provision of risk-reduction counseling should occur at every care visit unless the client has medical needs that take precedence.
Providers who had less encounter time (<30 minutes) with patients tend to counsel their patients more on medication and adherence and disease screening. Based on strong association between encounter time and prevention counseling practices, Valverde et al 34 suggested the need for reassessment of current practices, including reimbursement policies that limit providers’ time with patients new to HIV medical care. Our study also noted that significant variations in HIV risk-reduction counseling were associated with providers’ infectious disease board certification status, age of providers, and encounter times in favor of newly diagnosed patients. Providers who were infectious disease board certified, of age less than 45 years, and had less than 30 minutes of encounter time and patients’ population less than 100 were less likely to provide HIV transmission risk-reduction counseling to their patients. This suggests that more work needs to be done to reach certain HIV care providers in Houston/Harris County, Texas. However, training on brief risk screening methods that do not require much of providers’ time and brief risk-reduction interventions can enhance comfort, skills, and motivation of providers. 36,42 AIDS Education and Training Centers 43 and California STD/HIV Prevention Training Center 44 have developed training curricula, guidelines, practical tools, and other materials that provide clinicians with the knowledge and skills to incorporate HIV prevention activities into clinical care. Although patients may not immediately change their behavior, receiving prevention messages from their health care providers could boost confidence and increase their receptiveness to subsequent prevention messages, which may help prevent high-risk behaviors that lead to HIV transmission.
None of the demographic and medical characteristics were significant determinants of provision of mental health and substance use and social and family support services counseling by providers. However, in another study based on the current data, 45 more than 90% of the participating providers reported that mental health and alcohol abuse problems and lack of social and family support were major barriers to patients’ abilities to adhere to the continuum of HIV care. Despite the fact that these patients are particularly in need of counseling services in these areas, it is of concern to note in our study that less than 50% of the providers provided consistent mental health and social support counseling to newly diagnosed and established patients. However, Metsch et al 9 noted that physicians who perceived their patients to have mental health and substance abuse problems had less time to address prevention issues. Mental health and substance use issues, emotional distress, and past sexual abuse have also been associated with risky behavior 46,47 and can have negative effects on medication adherence, viral load suppression, and HIV drug resistance. 48 –50 These reports highlight the need to help patients maintain their physical and mental health and dignity, and care visits provide vital opportunity to reinforce prevention messages.
Study Limitations
This study is subject to the following limitations. First, the participation rate of 45% was considered low but slightly higher than the 42% obtained at the national level. 28 However, these study samples included mostly physicians who typically have lower survey response rates compared to persons who are not physicians. Consequently, our sample may not be representative of all HMCPs in Houston/Harris County, Texas. Second, although probability proportional to size sampling method was used to select participating facilities, it was not possible to ‘weight’ the providers’ self-reported responses to the survey questions because of the small sample size, and, therefore, some estimates may be subject to nonresponse bias. In addition, the wide confidence intervals of some of the AORs call for caution in the result’s interpretation. Third, our data were based on self-report by providers and were not confirmed through patient interviews or clinical records and thus are also subject to recall and social desirability bias. Fourth, the differential weights applied to the composite prevention counseling indices were based on conceptual rationale 32 and not the comparative importance of the care process or counseling quality and contents. Fifth, providers’ practices and awareness may have evolved since the data were collected in 2009. Despite these limitations, the information obtained from this survey provides a comprehensive picture of HMCPs’ preventive care counseling practices in Houston/Harris County, Texas, that are not captured through routine public health surveillance activities. Our study outcomes would lay strong foundation for implementing a comprehensive HIV prevention strategy that underscores the role of care providers in reducing new infections in the community, and supports the National HIV/AIDS Strategy.
conclusion
The clinical setting provides a unique opportunity for HMCPs to deliver prevention messages, especially as patients believe they provide reliable sources of HIV prevention information. Our study indicates that the frequency of preventive care practices varied across the measures and were generally described as suboptimal, with newly diagnosed patients receiving more consistent counseling services than the established patients. Although evidence-based guidelines recommend providing risk-reduction counseling to all HIV-infected patients during their routine clinic visits, 6,38,39 our study findings indicate the need for HMCPs to intensify preventive care counseling efforts, especially among established HIV-infected patients. However, deficits in knowledge or skill, provider attitude, and organizational structures have been identified as barriers to counseling in the clinic settings. 51 The low and inconsistent preventive care counseling by some HMCPs points to the need for continuing medical education that focuses on HIV care and prevention topics. Myers et al 52 demonstrated that training for providers increased the delivery of prevention counseling and they suggested strategies that could be used in clinic settings. Some of those include strategies such as the establishment of formal written guidelines for delivering behavioral interventions and development of peer support among clinicians. Also, projects such as the CDC’s Prevention IS Care, 24 which emphasize integration of ongoing brief prevention counseling by health care providers into routine care, provide the necessary tools and trainings that may help to prevent transmission by persons living with HIV.
Furthermore, understanding factors that are associated with preventive care practices such as differences in the prevention needs of newly diagnosed and established patients and the local clinical environment would assist in developing appropriate training curricula for providers. Given the multitude of health issues facing HIV-positive patients, many HMCPs may not feel that they have time to engage patients in discussions about high-risk behavior. Patient and community health depends on patient risk behaviors, which must be assessed over the duration of the patient–provider relationship. This is critical in order to ensure that preventive behaviors are sustained in communities facing higher risk of HIV infection. 53 Since continued high-risk behavior among patients contribute to the failure of public health efforts to reduce HIV incidence, 46 providers should commit to regular discussion of sexual risk behavior with HIV-positive patients. This will help patients build skills for adopting and maintaining safe behavior, thereby reducing the risk of onward transmission of HIV.
Footnotes
Acknowledgments
The authors would like to thank the HMCPs who participated in this survey; the MMP staff, and members of the Community Advisory Board and Provider Advisory Board in Houston project area; the Houston Department of Health and Human Services; and members of the Clinical Outcomes Team in CDC’s Behavioral and Clinical Surveillance Branch of the Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention.
Authors’ Note
OM conceived and designed the study, conducted the data analysis, interpreted the results, prepared the initial draft of the article, and participated in the critical review of article. MR-B, TB, SK, MS, PS, and JA interpreted the study findings and participated in the critical review of the article for important intellectual contents concerning their respective areas of specialty. RA and EJE played advisory roles in all aspects of the study and participated in the critical review of the article. All authors read and approved the final version of the article for publication. The CDC conceived the project, developed project-associated materials including data collection instrument, and provided oversight on the survey implementation in Houston/Harris County, Texas, and other participating sites. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Medical monitoring Project (MMP) 2009 Providers’ Survey was supported by the Centers for Disease Control and Prevention (CDC) under the Cooperative agreement number PS09-937.