
Abstract
The study describes the HIV care providers’ sociodemographic and medical practice characteristics and the health care services offered to patients during medical care encounters in Houston/Harris County, Texas. We used data from the pilot cycle of the Centers for Disease Control and Prevention Medical Monitoring Project Provider Survey conducted in June to September 2009. The average age and HIV care experience of the providers were 46.7 and 11.7 years, respectively, and they provided care to an average of 113 patients monthly. The average proportion of HIV-infected patients seen per month by race/ethnicity was 43.3% for blacks, 28.5% for whites, 26.6% for Hispanics, 1.3% for Asians, and 0.6% for other races. A total of 67% of providers offered HIV testing to all patients 13 to 64 years of age. Most HIV care providers (73.9%) reported that patients in their practices sought HIV care only after experiencing symptoms. Understanding the HIV care delivery system from providers’ perspectives may help enhance support services, patients’ ongoing care and retention, leading to improved health outcomes.
Keywords
Introduction
By the end of 2012, an estimated 21 405 persons were living with HIV infection in the Houston metropolitan statistical area (MSA). 1 The Houston MSA accounts for more than 30% of reported cases of HIV infection in the state of Texas 2 and ranks 12th nationally among MSAs for persons living with HIV infection. 3 Advances in antiretroviral therapy (ART) and medical care have led to increased survival for patients living with HIV, 4 –8 resulting in an increased number of patients requiring care. Treatment of HIV disease involves making complex decisions about ART, coordinating medical care, managing comorbid conditions, and linking patients to supportive services. As the medical needs of patients with HIV have evolved, so have the demands placed on their providers and the health care workforce to provide high-quality care. This has led to a high volume of patients being referred for management of comorbidities and providers possibly having less time to discuss transmission risk reduction interventions with patients. 9
There are more HIV providers retiring or leaving practice than there are new ones entering the field. A 2011 Institute of Medicine report raised concern about a lack of experience among HIV providers and cited a paucity of data about the training and qualifications of providers. 10 Current HIV treatment guidelines indicate that ART be considered for all patients, regardless of CD4 count. 11 Although scientific evidence supporting ART in the prevention of HIV has helped to expand the public health approach to include serious consideration of the clinical and preventive benefits of treatment for individuals and their communities, 7,12 –14 much remains unknown about the current HIV care delivery system and the ability to deliver such benefits. A system for monitoring adoption and implementation of HIV treatment guidelines by providers, clinical interventions to prevent transmission, and overall evaluation of public health focus is lacking.
A number of organizations, including the US Centers for Disease Control and Prevention (CDC), have suggested that evolving productivity standards that support quality care by HIV clinicians should reflect the complexity and intensity of HIV care and allow providers adequate time to monitor and manage the patient’s medical care needs and provide oversight of comorbidity management. 13 ,15 The growing and complex trajectory of HIV and its related disease burden has raised new challenges for health care providers and systems. 16
The patient–provider relationship is privileged and complex. In today’s health care system, where delivery involves numerous interfaces as clinicians manage patient care, the patient–provider relationship has proven to be central to effective primary care and chronic disease management. 17 –19 An ongoing and consistent relationship between patients living with HIV and their providers helps to establish open communication and trust and has been associated with better medication adherence rates, patients’ acceptance of treatment, and support service recommendations. 20 –22 Patients who report that their physicians exhibit patient-centered communication behaviors are significantly more satisfied with their care 23 –25 and report greater improvement in general medical conditions. 24
Ascertaining information about clinicians who provide HIV care, providers’ perceptions of patients, and the factors that influence their care decisions is not commonly done. We describe HIV care providers’ sociodemographic and medical practice characteristics, the type of health care services offered to patients, and provider–patient interactions during medical care encounters in Houston/Harris County, Texas.
Methods
Survey Design and Population
Data for this study were collected as part of CDC’s Medical Monitoring Project (MMP) Provider Survey. This survey was administered to a nationally representative sample of HIV care providers who were selected to participate in MMP. The MMP is an ongoing surveillance system conducted in 17 states and 6 cities/counties. It collects information on the behavioral and clinical characteristics of persons’ ≥18 years of age receiving medical care for HIV infection in the United States and Puerto Rico. The MMP methods have been described previously. 26 –28 Briefly, the MMP involves a 3-stage sampling design. The first stage was the selection of 26 areas based on AIDS prevalence in the United States (as of 2002), using probability proportional to size sampling. In the second stage, MMP staff developed a listing of facilities for their individual project areas. Facilities were eligible to be included if they were known to provide outpatient HIV care (defined as prescribing ART or ordering CD4 or HIV viral load tests) to patients ≥18 years of age for the purposes of managing the patient’s HIV disease. Facilities were sampled to account for a representative sample of clinics and facilities with small, medium, and large estimated patient loads. In the third stage, patients who received care at the sampled facilities during a specified time period were selected.
Methods for the MMP provider survey at the national level have been previously described in detail. 29 In Houston/Harris County project area, 20 facilities were originally selected from a sampling frame comprising 54 facilities to participate in MMP during the 2007 to 2008 data collection cycle. Of this number, only 13 (65%) facilities agreed to participate in the project and formed the basis for the provider survey conducted from June through September 2009. We present data from the Houston/Harris County component of the MMP Provider Survey. HIV care providers eligible for this survey included physicians, physician assistants, or nurse practitioners at the MMP-sampled facilities/providers who have provided care to, ordered CD4 or HIV viral load testing for, and/or prescribed ART to HIV-infected adults ≥18 years of age. Interns, residents, fellows, and others in the training programs were not eligible.
The survey included questions about providers’ demographics, medical practice characteristics, and self-assessed knowledge about HIV. Furthermore, the instrument assessed the HIV care providers’ patients demographics, estimated patient loads, the numbers that they provide care for, adherence to CDC’s HIV testing recommendations for routine testing, type of health care services offered to patients, health topics and preventive measures discussed by HIV care providers with established HIV/AIDS patients and those new to HIV care, and the providers’ perception of barriers to care among HIV-infected patients.
Data Collection
Prior to data collection, facilities participating in MMP were initially contacted for the names and contact information of eligible providers. A unique identification number was assigned to each provider based on a list of sequential ID numbers for each facility. Using the identification numbers, personalized recruitment packets containing a recruitment letter describing the purpose of the survey, information on how to access the survey online using the provider’s unique identification number, a paper copy of the survey with a postage-paid return envelope, and a small monetary incentive in the form of gift card were sent to the sampled HIV care providers. The survey required approximately 20 minutes to complete. A total of 51 questionnaire packets were mailed to eligible HIV care providers within the 13 participating facilities in the Houston project area. The Total Design Method 30,31 was used to follow-up on nonresponders. Reminder postcards were sent to all sampled providers 1 week after the initial mailing, and a replacement survey, a copy of the original recruitment letter, and a letter for nonresponders were sent to all providers who had not completed the survey at 3 and 7 weeks following the initial mailing.
Ethical Considerations
The US Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, Sexually Transmitted Disease (STD), and Tuberculosis (TB) Prevention has determined that MMP is public health surveillance and is considered a nonresearch activity used for disease control program or policy purposes. Given the nonresearch determination, it is not subject to human participants’ regulations including federal institutional review board (IRB). As an amendment to MMP, the MMP Provider Survey is covered under the same nonresearch determination. No local IRB was required for the Houston project area.
Analyses
The participating providers were grouped into “public” or “private.” Age of provider was classified as 36 to 44 years, 45 to 54 years, and 55 and above years. The providers’ year of entry into HIV care practice was categorized as 1981 to 1990 (first generation), 1991 to 2000 (second generation), and 2001 to 2010 (third generation). The number of patients that the HIV care providers provided care to per month were categorized as 1 to 50 patients (low), 51 to 100 patients (medium), and >100 patients (high). Several questions had a Likert-type response set of 1 = strongly agree, 2 = somewhat agree, 3 = neither agree nor disagree, 4 = somewhat disagree, and 5 = strongly disagree. These responses were collapsed into 3 main categories as agree (1 and 2), neither agree nor disagree (3), and disagree (4 and 5). Similarly, the 5-point item’s response (1 = Always discuss, 2 = frequently discuss, 3 = sometimes discuss, 4 = almost never discuss, and 5 = never discuss) to the health topics and preventive measures discussed by HIV care providers with patients were collapsed into 3 categories as always discuss (1), sometimes discuss (2 and 3), and almost never discuss (4). The option never discuss was not used by any of the study participants.
The t-test statistic was used to compare quantitative measures such as the patient demographics, time spent during provider visits, and missed appointments by facility type (public and private) with resultant group means and 95% confidence interval (CI) of the means. Chi-square statistic was used to assess the bivariate associations of HIV care providers’ responses to questions on the type of services they offered to HIV/AIDS patients, the use of referral services and drug benefit programs, and the health topics and preventive measures they discussed or adopted for patients new to HIV care and the established ones. All tests were 2 tailed, with probability value of .05 used as the statistical significance level. Data management and statistical analyses were performed using SAS statistical software version 9.3 (SAS Institute, Cary, North Carolina).
Results
Characteristics of HIV Care Providers
Surveys were returned by 23 (45%) of the 51 providers. Table 1 presents the characteristics of HIV care providers in the study sample. The majority of the HIV care providers were physicians (73.9%), and 26.1% were physician assistants and nurse practitioners. Slightly over half (52.2%) were males and 47.8% were females. The average age of study participants was 46.7 years, with the highest proportion (47.8%) belonging to the age category 36 to 44 years. Over half (52.2%) were white, 17.4% were black, and 17.4% were Hispanic/Latino. The number of HIV-positive patients seen by the providers per month varied considerably at the clinics with 39.1% reportedly seeing more than 100 patients monthly. Most providers had 6 years or more of clinical experience (91.3%), with an average of 11.7 years of practice for the entire sample. Although all participating providers considered themselves to be knowledgeable in HIV treatment, 60.9% of them self-identified as board-certified infectious disease physicians. About 47.8% of the respondents indicated that they used only the English language to provide care to patients infected with HIV. Although 39.1% of providers reported using both English and Spanish in their practice, 13.0% used English and other languages such as Chinese, French, or German.
Characteristics of HIV Care Providers in the Study Sample—Houston, Medical Monitoring Project Provider Survey, 2009.

Abbreviation: SD, standard deviation.
aPercentages may not add up exactly to 100% due to rounding.
bBased on HIV care providers delivering care to both HIV-negative and -positive patients (n = 17).
cLanguages used in providing HIV-related medical care to patients.
Patients’ Demographic Characteristics
Providers’ self-reported demographic characteristics of patients living with HIV seen at both public and private facilities in an average month are shown in Table 2. A total of 43.3% were black, 28.5% were white, 26.6% were Hispanic/Latino, and 1.3% was Asian. Black patients were significantly more likely to be seen at public facilities, and white patients were significantly more likely to be seen at private facilities (P ≤ .05). Mean proportions of other subgroups of HIV-positive patients who received care in Houston/Harris County facilities include 36.4% women, 4.1% transgender, 10.6% injection drug users, and 53.3% men who have sex with men (MSM). More MSM (35% points more, P < .001) were seen by providers in private practice rather than those in public clinics.
Providers’ Self-Report of Demographic Characteristics of Patients Living with HIV in Publica and Privateb Facilities in an Average Month—Houston, Medical Monitoring Project Provider Survey, 2009.c

Abbreviations: MSM, men who have sex with men (as percentage proportion of male HIV cases); ns, not significant.
an = 13.
bn = 10.
cWithin characteristic, means for private and public facilities are significantly different at P ≤ .05.
dMean percentages across race/ethnicity characteristic may not add up exactly to 100% due to rounding.
e P < .001.
f P < .05.
g P > .05.
Medical Practice Characteristics
Providers reported that the average number of HIV-positive patients that they deliver care to during an average month was 112.6 (95% CI: 78.4-146.8; Table 3). The average percentage of patients living with HIV who missed their scheduled appointments during an average clinic week was 20.3% (95% CI: 14.6-25.9), with no significant (P > .05) difference reported between private and public facilities. Similarly, time spent by the providers with new patients during clinic visits averaged 42.2 (95% CI: 36.8-47.5) minutes, with significant (P < .05) variations noted between private and public clinics (38.5 versus 47.0 minutes), respectively. However, less time (18.8 minutes; 95% CI: 16.5-21.2) was spent on average by HIV care providers with established patients.
Providers’ Self-Report of Health Care Provision to HIV-Positive and -Negative Patients during an Average Week/Month—Houston, Medical Monitoring Project Provider Survey, 2009.a

Abbreviation: ns, not significant.
aWithin a service/activity, means for private and public facilities are significantly different at P < .05.
bFacility type: public (n = 13); private (n = 10).
c P > .05.
d P < .05.
eBased on HIV care providers delivering care to both HIV-negative and -positive patients (n = 17).
A total of 17 (73.9%) of the 23 providers in the sample provided care to both HIV-positive and -negative patients. On the average, 147.7 (95% CI: 47.3-248.0) HIV-negative patients received care during a month. HIV clinicians in private practice provided medical care to more HIV-negative patients than those in public clinics (231.3 versus 73.3; P < .05). Sixty-seven percent of providers whose practice included HIV-negative patients stated that they offered screening to their patients aged 13 to 64 years, while 26.6% only screened those patients who reported engaging in high-risk behaviors. A small proportion of providers (6.6%) had planned to start offering HIV screening to all of their patients (data not shown).
The proportion of HIV-negative patients who missed their scheduled appointments on an average clinic week was 13.7% (95% CI: 8.9-18.4), with no significant variations observed between private and public providers. Of the 11 identified sources of information used by providers to support their medical practice, only 3 of those were considered major sources. These include the US Public Health Service (USPHS) and/or Infectious Diseases Society of America (IDSA) antiretroviral (ARV) guidelines (96%), medical journals/textbooks (83%), and Internet sources (70%).
HIV Providers’ Perspectives on Care Services
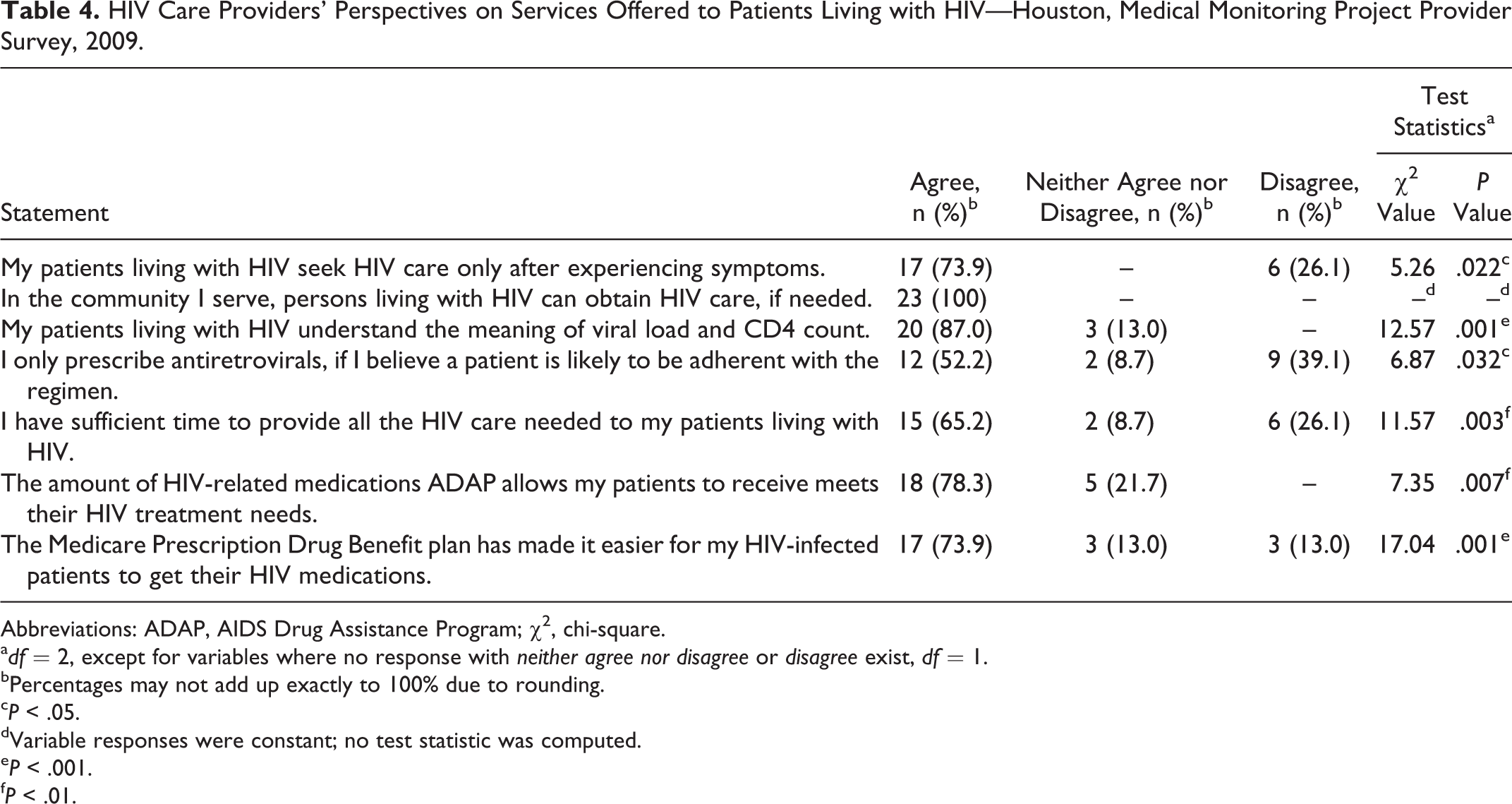
The majority of HIV care providers in Houston/Harris County (73.9%, P < .05) agreed that patients living with HIV seek HIV care only after experiencing symptoms. However, all (100%) participating providers agreed that HIV care is readily available in their respective communities. HIV care providers also reported (87.0%, P < .001) that their patients are involved in their care and do understand the meaning and basic interpretations of both HIV viral load and CD4 counts. Slightly over half (52.2%, P < .05) of the providers prescribe ART only to those patients who are likely to be adherent, and 65.2% of HIV care providers agreed (P < .01) that they have sufficient time to provide all the HIV care needed by patients. A large proportion of providers (78.3%, P < .01) reported that the amount of HIV-related medications approved by Texas AIDS Drug Assistance Program (ADAP) allows their patients to meet their HIV treatment needs. Similarly, 73.9% (P < .001) of HIV care providers in Houston/Harris County reported that the Medicare Prescription Drug Benefit plan has made it easier for their patients to get HIV medications (Table 4).
HIV Care Providers’ Perspectives on Services Offered to Patients Living with HIV—Houston, Medical Monitoring Project Provider Survey, 2009.
Abbreviations: ADAP, AIDS Drug Assistance Program; χ2, chi-square.
a df = 2, except for variables where no response with neither agree nor disagree or disagree exist, df = 1.
bPercentages may not add up exactly to 100% due to rounding.
c P < .05.
dVariable responses were constant; no test statistic was computed.
e P < .001.
f P < .01.
Drug Benefit Programs and Referral Services
A total of 91.3% (P < .001) of HIV care providers in Houston/Harris County assented that they provide care to patients living with HIV who receive ADAP and those enrolled in the Medicare Prescription Drug Benefit plan (Table 5). Although not statistically significant, approximately 56.5% and 65.2% of providers indicated that they have sufficient time to provide all HIV-related information needed by new and established patients, respectively. The majority of providers reported that they have never referred patients living with HIV to other physicians with specialized knowledge for initial HIV evaluation, initiating and changing ART, interpreting viral load or other test results, and choosing opportunistic infection prophylactic treatment. The range of agreement by the providers for nonreferral of these services to other physicians with specialized knowledge ranged from 78.3% to 91.3% (P ≤ .01).
HIV Care Providers’ Use of Drug Benefit Programs and Their Opinion on Provision of HIV-Related Information to PLWH in Houston/Harris County—Houston, Medical Monitoring Project Provider Survey, 2009.

Abbreviations: ns, not significant; χ2, chi-square.
a df = 1.
b P < .001.
c P > .05.
HIV Care Provider–Patient Interactions
Table 6 presents the list of health topics and preventive measures discussed by HIV care providers with their new and established patients during clinic visits. There were 20 items identified as commonly discussed topics and preventive measures; the frequency at which many of these items were discussed differed significantly (P < .05) between new and established patients. Statistical significance (P ≤ .05) was attained in 9 of the items for patients new to HIV care compared to 13 items in established HIV-positive patients. The majority of providers indicated that they always discussed the following topics with patients new to HIV care: “adherence with ARV regimen (91.3%),” “adherence to opportunistic infection prophylaxis (78.3%),” “how to take medicines (82.6%),” and “medical-related side effects (82.6%).” Less than half (47.8%) of the HIV care providers always discussed family/social support with their new patients. With established patients, the majority of the HIV care providers tended to discuss only 12 of the 13 topics/preventive measures, sometimes, with their proportions ranging from 26.1% (adherence with ART regimen) to 73.9% (substance abuse and tuberculosis disease risk; Table 6). A small proportion of HIV care providers (≤13.0% for new patients and ≤26.1% for established patients; P ≤ .05) indicated that they almost never discussed some of the health topics or preventive measures. Seven items that attained statistical significance (P ≤ .05) and were always discussed with both new and established patients by HIV care providers included “adherence with ART regimens (91.3% and 73.9%),” “how to take medicines (82.6% and 30.4%),” “availability of partner counseling services (21.7% and 8.7%),” “substance abuse (34.8% and 17.4%),” “tuberculosis disease risk (52.2% and 17.4%),” “family/social support (47.8% and 21.7%),” and “mental health problems, including depression (43.5% and 17.4%).” Two topics of major importance that HIV care providers only sometimes discussed with established patients were condom use (69.6%, P < .001) and disclosure of HIV status to their partners (65.2%, P < .01).
Health Topics and Preventive Measures Discussed by HIV Care Providers with Patients New to HIV Care and Established HIV-Positive Patients—Houston, Medical Monitoring Project Provider Survey, 2009.a

Abbreviations: ART, antiretroviral therapy; ns, not significant; OI, opportunistic infection; χ2, chi-square.
aWithin patient groups (new to HIV care versus established) percentages may not add up exactly to 100% due to rounding.
bA patient new to HIV care refers to someone who has not previously obtained HIV care and not a patient new to one’s practice.
cEstablished patient refers to someone who has been seen at a facility/practice on at least 1 prior occasion for HIV care.
d df = 2, except for variables where no response with almost never discuss existed, df = 1.
e P < .001.
f P < .05.
g P < .01.
h P > .05.
i P < .0001.
Discussion
The increased prevalence of persons living with HIV is resulting in an increased demand for primary health care services and shortages of the HIV medical workforce. The findings indicate that slightly over half of the HIV care providers were of age 45 or older, with more than 10 years of HIV care experience, suggesting that most started practicing between 1981 and 2000. According to the Health Resources and Services Administration (HRSA), more than a third of US physicians in practice are aged 55 or older and are likely to retire in the next 10 to 15 years. 32 There is an estimated current shortage of 7000 primary care physicians in underserved areas. 32 Because more HIV providers are leaving their practice without a sufficient pool of new providers to take their place, 10,33 this may result in provider providers shortage that could impact the quality of care received by persons living with HIV. Almost 40% of the providers in our sample reported that they see at least 100 HIV-positive patients per month. Although not statistically significant, an increased number of patients seen at these clinics were associated with providers’ increased years of practice experience. Increase in HIV caseloads ranging from 25% to 90% have already been reported by many HIV physicians over the last couple of years. 32,34,35 In a national survey of physicians, size of HIV care practice has been more strongly associated with HIV-specific knowledge than with specialty training. 36,37 Although HIV care providers in our sample self-rated themselves as being either very or extremely knowledgeable in HIV care, we did not find any association between HIV-specific knowledge and number of patients they cared for in their clinics.
Approximately 60.9% of our study participants were board-certified infectious disease physicians. This proportion is similar to the 59% reported in national provider survey data. 29 However, the reality is that the management of HIV disease necessitates both specialty and primary care expertise. It has been estimated that primary care physicians comprise a large proportion of physicians who care for persons living with HIV. 32,37 Physicians of color, particularly blacks and Hispanics/Latinos, are greatly underrepresented among the HIV care providers in Houston/Harris County, Texas. Our study indicates that more than 70% of the patients cared for are minority, whereas over half of the providers in Houston/Harris County are white. The HIV Medical Association (HIVMA) similarly noted a severe shortage of minority physicians in the field of HIV. 38 To alleviate this problem, HRSA is currently developing resources for providers to enter HIV/AIDS care as well as strategies to extend the capacity of the existing health care workforce. 32
Houston is one of the most culturally and ethnically diverse cities in the United States. 39 We noted that slightly over half of the HIV care providers used languages other than English to administer care to their patients. Access to language-concordant physicians by patients has been effective in reducing reports of adverse medication effects and confusion with medication instructions. 40 This finding offers credence to having a system that will enhance the language proficiency of the health workforce and help to reduce language barriers to HIV care within the health care system.
A higher proportion (P < .05) of white than black patients visited private providers than public providers for HIV care. This finding may be associated with the diversities in unemployment, uninsurance, or underinsurance among minorities, especially blacks, 41 causing more HIV-infected individuals to rely on Ryan White HIV/AIDS Program-funded clinics and safety net HIV providers such as community health centers and public hospitals that offer free HIV care. The finding that a high proportion of MSM (53%) received HIV care may be an indication of the disproportionate burden borne by this subgroup in Houston/Harris County. 42
Slightly over two-thirds of HIV care providers in our sample offered HIV screening to all their patients aged 13 to 64 years. This figure is slightly higher than the 60% observed at the national level. 29 Several barriers to HIV screening among physicians such as insufficient time, burdensome consent process, lack of knowledge/training, lack of patient acceptance, pretest counseling requirements, competing priorities, and inadequate reimbursement have been identified by Burke et al. 43 McNaghten et al 29 found that younger physicians were more likely than their older counterparts to offer HIV testing to their patients, and they attributed this to training on HIV testing, diagnosis, and treatment. This may explain in part our finding, since majority of our participants were relatively older and experienced HIV care providers. Implementation of routine HIV testing by health care providers presents an opportunity to diagnose HIV early in the course of disease, link infected persons to care and treatment and encourage reduction in risky sexual behaviors and prevent new infections. 29,44,45 For these reasons, the National HIV/AIDS Strategy has focused public health efforts on the HIV care continuum, from diagnosis to linkage to care and ART. 46
HIV care providers in our study reported that on average, one-fifth of HIV-positive patients missed their scheduled clinic appointments. Our finding supports earlier study outcomes where 20% to 40% of recently diagnosed patients missed outpatient clinic appointments. 47,48 Patients with regular clinic visits are more likely to receive comprehensive care including preventive care, reducing the frequency of hospitalizations and emergency department visits, and decreasing overall health care expenditures. 47 We also noted that private HIV care providers spent more time with patients new to care than do those in the public settings. This finding may be related to the fact that most public clinics use an integrated care model, where coordinated access to subspecialty care needs and services are available, thus providers can address immediate clinical needs in less time.
Our study revealed that about 74% of HIV care providers reported that majority of people living with HIV seek HIV care only after experiencing symptoms, leading to late diagnosis and treatment. Among those initially diagnosed with HIV infection during 2009, one-third was diagnosed with AIDS within 12 months, indicating they were likely infected for many years without knowing it. 49 Late diagnosis contributes to mortality and morbidity and suggests missed prevention opportunities. 50,51 The most commonly cited reason for delaying care among HIV-positive patients in Houston/Harris County was fear (42%) followed by denial (35%) and not feeling sick (34%). 42 Delayed entry into care and intermittent care can lead to poor clinical outcomes, development of drug-resistant virus, and transmission of HIV to others. 52 Retaining HIV-infected patients in medical care at regular intervals have been shown to be linked to positive health outcomes. 53
No referrals were made for identified medical services by the majority of HIV care providers in our study. This may be an indication of greater HIV experience and expertise as their practice years averaged 11.7 years, with 61% of the providers identifying as board-certified infectious disease physicians. It was interesting to note that all of the participating HIV care providers in the Houston/Harris County reported that persons living with HIV can easily obtain care. This finding supports the Houston Area Ryan White Planning Council needs assessment survey outcomes in which patients were asked about their experience accessing available Ryan White HIV/AIDS Program core medical services. 42 In this survey, 74%, 68%, and 63% of patients identified the top 3 services as primary medical care visits, HIV medications, and case management, respectively, and asserted that these services were all very easy obtain.
Most (91.3%) of the providers in our study reported that they provide care to patients who receive ADAP and those enrolled in the Medicare Prescription Drug Benefit plan and that these programs significantly (P ≤ .01) provide for patients’ treatment and medication needs. Since 1992, HRSA through the Ryan White Grant Administration has awarded and administered over US$300 million in funding to health and social service agencies in the Houston Eligible Metropolitan Area (EMA). 54 The flexibility afforded by Ryan White funding in filling the coverage gaps has been critical to helping many persons living with HIV find medical care homes in the Houston EMA.
HIV medical care providers stated that they “always discussed” certain health topics and preventive measures with patients new to HIV care and only “sometimes” or “almost never discussed” them with established patients. The most discussed topics with both groups were “adherence to ART,” “how to take medicines,” “ART side effects,” and “family/social support.” Although the topics discussed likely differ from one patient to another depending on the scenarios and associated health needs, shared decision making can increase patient engagement in care, help reduce HIV transmission risk and improve ART adherence. 55
Given the IDSA/HIVMA HIV primary care guidelines, 16 for achieving HIV viral suppression, and the current emphasis of treatment as prevention, adherence to ART has become even more critical. Our study recorded a much higher proportion of HIV care providers (91.3%) who consistently discussed adherence to ART regimen with patients new to HIV care who were prescribed ART compared to 87% of MMP providers reported at the national level. 56 However, the proportions of HIV care providers who reported consistent discussion of preventive care with new and established HIV-positive patients in the 3 integrated areas (HIV transmission risk reduction, partner counseling services, and discussions of STD risk), 15 in our study were low to moderate. Thus, there is cause for concern, given the emphasis on prevention activities for HIV-infected persons reflected in the National HIV/AIDS Strategy for the United States, 46 and the central role of HIV care providers in this effort. For instance, care providers who agreed to consistently discussing partner counseling services with new and established patients were only 21% and 8%. Referral to partner counseling services is crucial for preventing new infections in sex partners who are not infected and for ensuring that infected partners promptly receive HIV care. 56 In summary, the ultimate aim of incorporating HIV prevention into the medical care of people living with HIV is to implement a safer sex program that will instill self-protective and partner-protective motivations for reducing risk behaviors over time.
It is important to assess providers’ prevention counseling practices and determine how best to promote these practices in order to reduce high-risk behaviors among persons living with HIV. Our current study indicates that a significant proportion of HIV care providers may benefit from additional trainings. Consequently, training on brief risk screening methods that do not require much of providers’ time and brief risk-reduction interventions can enhance comfort, skills, and motivation of providers. 57 The AIDS Education and Training Centers, 58 which operate nationwide, provide excellent education and training programs for health care providers treating persons living with HIV/AIDS and can be instrumental for this purpose.
Study Limitations
This analysis has some limitations. First, the participation rate of 45% may be considered low; however, our sample included mostly physicians who typically have lower survey response rates compared to persons who are not physicians. 59 Second, the HIV care providers who responded to the survey made up a relatively small sample and may not be representative of the providers in Houston/Harris County, Texas. Third, although probability proportional to size sampling method was used to select participating facilities, it was not possible to weight the providers’ self-reported responses to the survey questions because of the small sample size. Fourth, providers’ practices and awareness may have evolved since the data were collected. Despite these limitations, the information obtained from this survey provides a comprehensive picture of HIV care providers’ perspectives that are not available through routine public health surveillance activities.
Conclusions
The majority of the HIV medical workforce in Houston/Harris County is composed of HIV clinicians who entered the field in the early years of the epidemic. As these clinicians retire without replacements, the HIV care system may face a crisis in care capacity. 38 This study suggests that concerted efforts may be needed by government, professional health care schools, and organizations to recruit, educate, and retain clinicians in the field. Since Houston/Harris County is culturally and ethnically diverse with minorities comprising a greater proportion of the overall population, there is absolute need for more diverse, multilingual, and culturally competent HIV care providers workforce to cope with the increasing demand for health care services in the community. In addition, the high proportion of persons being diagnosed with AIDS within 12 months of HIV diagnosis suggests that increased access to both routine and targeted HIV testing is needed to ensure early diagnosis of HIV and subsequent reduction in the proportion of people unaware of their HIV status. Adherence to USPHS screening guidelines by HIV care providers, facilitation of primary care linkage, and the development of a consistent set of measures to examine retention in care are critical first steps for improving the health of persons living with HIV.
Footnotes
Authors’ Note
OM conceived and designed the study, conducted the data analysis and interpretation of the results, prepared the initial draft of the article, and participated in critical review of article; SK, TB, MR-B, and JMB interpreted the study findings and participated in the critical review of the article for important intellectual contents concerning their respective areas of specialty; RA and EJE played advisory roles in all aspects of the study and participated in the critical review of the article. All authors read and approved the final version of the article for publication. The CDC conceived the project, developed project-associated materials including data collection instrument, and provided oversight on the survey implementation in Houston/Harris County, Texas, and other participating sites. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention.
Acknowledgments
The authors would like to thank the HIV medical care providers in Houston/Harris County who participated in this survey; the MMP staff, and members of the Community Advisory Board and Provider Advisory Board in Houston project area; the Houston Department of Health and Human Services and members of the Clinical Outcomes Team in CDC’s Behavioral and Clinical Surveillance Branch of the Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Medical Monitoring Project (MMP) 2009 Providers’ Survey was supported by the Centers for Disease Control and Prevention (CDC) under the Cooperative agreement number PS09-937.