
Abstract
Background:
In sub-Saharan countries, HIV testing and treatment facilities are available, especially at subsidized rates for the past few years.
Methods:
A prospective and descriptive review was conducted at Yalgado Ouédraogo Teaching Hospital Internal Medicine department in Ouagadougou, using personal case report forms, between June 2009 and August 2010 in all newly diagnosed adults with positive HIV antibody.
Results:
The study participants consisted of 191 patients at a median age of 37 years (range, 18-65 years) and sex ratio (men/women): 0.66. In all, 110 (57.6%) patients were symptomatic. Fourteen patients were lost to follow-up. Of the 177 patients, 144 had CD4 count <350 cells/mm3 and all have been treated. At the ninth month, weight gain and immune restoration were significant (P < .01); only 79 of the 144 patients had viral load measurement, and 76 of the 79 were undetectable. Mortality rate of treated patients was 6.25%.
Conclusion:
Laboratory tests and highly active antiretroviral therapy make the management of patients easier, but a majority of them still presented late and were still lost to follow-up. Nevertheless, we have excellent treatment success.
Introduction
Recent epidemiological data show a continuous stream of new diagnoses of HIV infection. 1 The Joint United Nations Programme on HIV/AIDS (UNAIDS) estimated that there were 1.8 million newly diagnosed HIV-infected patients in the world, in 2009. 1 In Burkina Faso, the prevalence of HIV infection in the general population was 1.2% in 2009, with 6800 new infections. 1 Significant efforts have been made in recent years (awareness, screening, and access to antiretrovirals [ARVs] and monitoring through laboratory tests) in the fight against HIV/AIDS in Burkina Faso. Knowledge of the epidemiological, clinical, and immunological characteristics of patients treated in Burkina Faso after so many years of struggle is essential for the organization of medical care for HIV infection. The lack of data has led us to the present study whose objectives were to describe the social, epidemiological, and clinical features of newly HIV-infected patients managed in the Internal Medicine Department of Yalgado Ouédraogo Teaching Hospital (CHUYO) of Ouagadougou and changes after 9 months of follow-up.
Patients and Methods
This was a prospective and descriptive study which was conducted from June 1, 2009, to August 31, 2010, in the Internal Medicine department of CHUYO. The study included all HIV-infected patients (confirmed on a second sample using HIV enzyme-linked immunosorbent assay test) aged at least 15 years, not followed before, not receiving antiretroviral therapy (ART), and managed for the first time in the Internal Medicine department of CHUYO. These patients were followed for 9 months after inclusion. Patients who did not accept to participate in the study and those who received prior follow-up for HIV infection (transfers) were not included. A survey form containing sociodemographic, epidemiological, clinical, and laboratory variables was used for data collection for each patient. The tracking records in ambulatory and hospital records of patients constituted the data sources.
The parameters studied at the beginning of follow-up were age, sex, body mass index (BMI), the conditions of testing and time management (time between the discovery of HIV-positive status and first consultation supported), clinical symptoms, clinical stage according to the classifications of the US Centers for Disease Control and Prevention (CDC) Atlanta 1993 and the World Health Organization (WHO) 2006, opportunistic infections diagnosed, and the number of CD4 cells. During the follow-up, patients treated with ARVs were reviewed at the third, sixth, and ninth months to assess their overall clinical condition, adherence to treatment, and immune status. Untreated patients were reviewed at the sixth month to assess clinical and immune status. The BMI was estimated by the weight (kg) divided by height in square meters (m2). The values were classified into 4 groups according to the WHO criteria (BMI <18.5: underweight; 18.5 ≤ BMI ≤ 24.9: normal weight; 25 ≤ BMI ≤ 29.9: overweight and moderate obesity; BMI > 30: frank obesity). Noncompliance was defined as irregular use of ART during the past 4 days.
The diagnosis of certain diseases was difficult because of our technical limitations and financial inaccessibility of the patient to make some examinations. Thus, the conditions below were defined by the following criteria:
The diagnosis of pulmonary tuberculosis was confirmed by the presence of acid-fast bacilli in sputum; or on clinical, radiological, and therapeutic response when the smear was negative. The diagnosis of extrapulmonary tuberculosis was confirmed by the presence of granulomas on biopsy; Diagnosis of oropharyngeal candidiasis, prurigo, and skin herpes zoster was confirmed based on the clinical criteria; Pyogenic pneumonia was confirmed based on the clinical and radiological data and favorable nonspecific antibiotic therapy.
Immune deficiency was severe when the CD4 count was less than 200 cells/mm3 and moderate when the CD4 count was between 200 and 499 cells/mm3. A CD4 count equal to or higher than 500 cells/mm3 was considered to be normal. Patients were clearly informed about the study and the confidentiality of data was ensured. Free consent of the patients was required before inclusion in the study.
Data were analyzed using Epi info.3.5.1. The chi-square test was used for the comparison of proportions and the Fisher test for comparison of means.
Results
During the inclusion phase, 191 new HIV-infected patients were managed in our department. Among them, 14 did not return to the medical follow-up after the first consultation.
Characteristics of All Patients
The patients consisted of 76 males and 115 females, with a sex ratio of 0.66. The main characteristics of these patients are described in Table 1.
Features of All New Patients (n = 191).
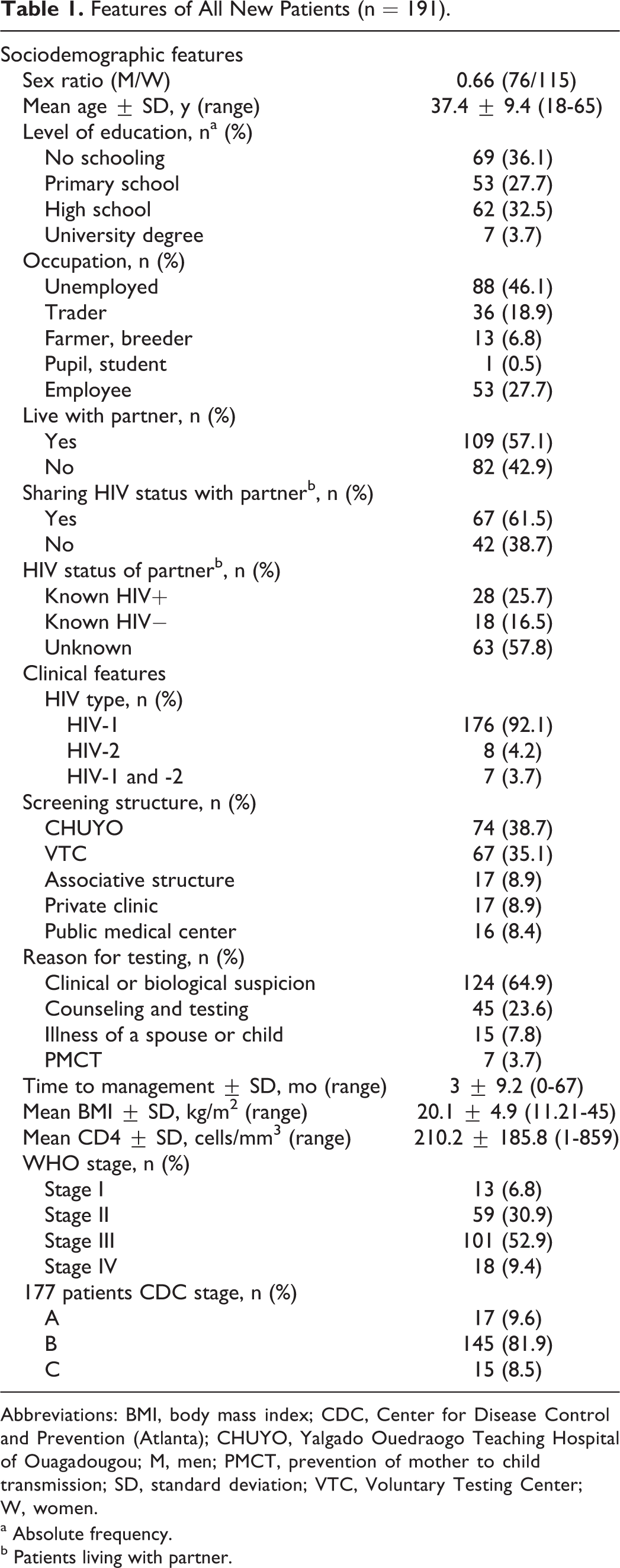
Abbreviations: BMI, body mass index; CDC, Center for Disease Control and Prevention (Atlanta); CHUYO, Yalgado Ouedraogo Teaching Hospital of Ouagadougou; M, men; PMCT, prevention of mother to child transmission; SD, standard deviation; VTC, Voluntary Testing Center; W, women.
a Absolute frequency.
b Patients living with partner.
Of all, 144 (75.4%) patients were of the age between 15 and 49 years. All patients were reported being heterosexual. Of the 124 patients diagnosed due to clinical suspicion, 44 (35.5%) patients had prolonged fever, 19 (15.4%) had prolonged diarrhea, 15 (12.1%) had dermatological and venereal (prurigo, genital herpes, herpes zoster) infections, and 12 (9.7%) had recurrent pulmonary infections.
In all, 141 (73.8%) patients attended our service during the month following their HIV screening and 35 (18.3%) after 6 months. The factors that delayed the consultation beyond 6 months were fear of stigma (48.6%, n = 17), denial (37.1%, n = 13), lack of information (8, 6%, n = 3), and religious reasons (5.7%, n = 2).
Of all, 69 (36.1%) patients were lean and 100 (52.4%) patients had a normal weight. In all, 110 patients were symptomatic at the first consultation. Candidiasis digestive concerned 37 (33.6%) patients, weight loss was reported in 35 (31.8%), and dermatologic and venereal symptoms were present in 21 (19.1%) patients.
In 177 patients, the CD4 count was performed. Table 2 shows the distribution of patients according to the CD4 count. Serology for hepatitis B virus (HBV) was performed in 20 patients. The HB antigen was positive in 4 patients. Serology for hepatitis C virus (HCV) was performed for 28 patients, and no patient had HCV antibody. Syphilis serology was performed in 15 patients and was negative in all.
CD4 Count in 177 Patients Infected with HIV during Their Initial Blood Analysis.

Comparison between Men and Women
Comparisons of patients by sex and sociodemographic profiles and clinical and immunologic characteristics are reported in Table 3. Among the patients living with a partner (n = 109), 37 women (64.9% of all women) and 28 men (53.9% of all men) did not share their HIV status with their partner (P = .24). In all, 18 (15.7%) women and 4 (5.3%) men had consulted more than 6 months after HIV screening (P = .03).
Comparison of Patients According to Sex and Sociodemographic, Clinical, and Immunological Features.

Abbreviation: CDC, Center for Disease Control and Prevention (Atlanta); SD, standard deviation; WHO, World Health Organization.
a The CDC classification was made only for patients with CD4 count.
Therapeutic Aspects
For a given patient, highly active antiretroviral therapy (HAART) was started when the CD4 count was less than 350 cells/mm3 or when the patient was classified as stage 3 or 4 according to the WHO classification. Among the patients who achieved the CD4 count (n = 177), 144 (81.4%) started receiving HAART after the initial laboratory test. The remaining 33 (18.6%) were not initially treated with ARV drugs, either because they were not eligible or because their condition does not allow it. The mean BMI of treated patients was 19.6 kg/m2 at the first consultation, and their mean CD4 count was 143.7 ± 108.5 cells/mm3. The mean CD4 count in untreated patients was 500.6 ± 174.3 cells/mm3 to baseline. Table 4 shows the distribution of patients according to the ARV treatment received.
Distribution of Patients According to the Received Antiretroviral Combination Therapy.

Abbreviations: HAART, highly active antiretroviral therapy; ZDV, zidovudine; 3TC, lamivudine; EFV, effavirenz; NVP, nevirapine; d4T, stavudine; LPV/r, lopinavir/ritonavir; FTC, emtricitabine; TDF, tenofovir.
Evolutionary Aspects
Untreated patients
Among the 33 untreated patients, 5 (15.15%) died during the follow-up period. Three of these deaths occurred in the month following the first consultation and their CD4 counts were 5, 15, and 1 cells/mm3, respectively. Other patients (28) were reviewed after 6 months. Among them, 3 had a CD4 count less than 350 cells/mm3 and therefore were started on HAART.
Treated patients
During the 9-month follow-up of our 144 patients, 7 experienced adverse reactions requiring a medicine switch: a skin reaction to nevirapine and 6 cases of severe anemia due to zidovudine (ZDV). In all, 10 patients were transferred to other HIV-infected patient management centers.
Noncompliance to HAART was found in 11 (7.6%) patients. The reasons included the lack of understanding the treatment (7 patients) and refusal (1 patient) to undergo the therapy.
In all, 9 (6.25%) patients died, including 6 in the first 3 months. The causes of death were chronic gastroenteritis (4 patients) and lung infections (3 patients); the cause was not found in 2 patients. Figure 1 shows the changes in the mean BMI and CD4 count of patients who were initiated on HAART and reviewed at their appointments. The lack of understanding of the follow-up procedures was the main reason for patients missing their follow-up appointment, and also the failure of laboratory measuring equipment between the third and the sixth month was a contributory factor.

Changes in mean body mass index (BMI) and the average CD4 count in patients treated with antiretroviral drugs, from the beginning to 9 months of treatment.
At 9 months of follow-up, viral load was available for 79 (54.9%) patients. It was undetectable (detection limit: 50 copies/mL) in 76 (96.2%) patients and detectable in 3 noncompliant patients with the respective values of 310, 200, and 277 242 copies/mL.
Discussion
This study has some data limitations; nevertheless, our results remain valid. The study is limited to an urban center; a selection bias could be present. New consultants in this service were not necessarily comparable with those in the rural areas. We also mention the possible recall bias on the data concerning the date of discovery of HIV status, and data on time to management should be analyzed with caution.
The female predominance and the younger age of our patients are typical data of the epidemiology of HIV infection in Burkina Faso and West Africa.1–5
Studies in Ouagadougou and Bobo-Dioulasso show that men have less recourse to health services, women are more concerned with screening and feel more vulnerable about the diagnosis, the motivations of men and women differ, and their experiences of screening and its consequences are different. 6 Early age at first sex among girls and the relative protection afforded by male circumcision are also factors that could explain the female predominance. 7 , 8
In Europe, North America, and Asia, there is a male preponderance, which is explained by the fact that the HIV epidemic in these countries evolved early among homosexual men.9–11
With an average age of 37 years, the majority of our patients were under 50 years. The HIV epidemic mainly affects the young and sexually active population in the world as evidenced by several studies in the world and the various reports of UNAIDS.1,2,5,9,12 –14
Men lived longer in a relationship (P = .01), more often held an occupation (P < .001), and were relatively more educated (P = .09) than women. The stomping ground of HIV remains social, professional, and emotional precariousness. 1 This study showed that HIV status was most often shared (61.5%) for patients living with a partner while in a Senegalese study, status was less frequently shared. 12 Approximately 1 of the 5 patients consulted more than 6 months after the screening, but the average consultation did not differ significantly by sex. Fear of stigma and denial are often reasons for a late consultation. The average consultation is usually later in countries with limited resources 12 , 13 than in developed countries.9,10
In general, the greater social inclusion of men is because populations in sub-Saharan Africa traditionally accept that the man acts for the family. For men, the exacerbation of values such as “capacity” and dignity often elicits a strong feeling of shame among those who perceive themselves as no longer meeting the social norms. 14 Thus, the disease and the demand for care are seen as signs of weakness. This could also explain the delay in screening and treatment for men.
Symptomatic status of patients is also reported in other developing countries, where the majority of patients are in stage B and C of the CDC classification or 3 and 4 of the WHO classification.3 –5,11 –14 Men were more clinically symptomatic than women (71% vs 57% in stages 3 and 4, P = .03) without statistically significant immunologic difference. In Cotonou, a study found a higher frequency of severe immune deficiency in men than in women because men usually present for screening later than women. 5
Among the clinical manifestations, gastrointestinal candidiasis, weight loss, and skin disorders were prominent. These events were also found in a conclusive stage and correlated with immunosuppressant stage in most studies.5,9,15 –17
The practice of screening for hepatitis virus coinfection was rare compared with what is done in Europe and Asia.9,11
Because of the late screening and management of patients, the CD4 count was still initially low. In our study, the CD4 count was relatively high compared with studies in tropical areas a few years ago.2,5,11 –13
In all, 4 of the 5 patients started ART. This access has been facilitated by the current free ARV therapies. In addition, current recommendations 18 encourage starting treatment when the CD4 count is less than 350 cells/mm3, whereas only half of the patients had a CD4 count less than 200 cells/mm3, the upper limit recommended a few years ago. 19
Treatment was prescribed according to current guidelines during the study period. 19 Therapeutic combinations containing ZDV and lamivudine were the most commonly prescribed (58.3%). Stavudine was always prescribed in our country for cost reasons, and access to other frontline medicine replacement was not possible. Tolerance and adherence to ARV drugs were good.
Despite free ARV drugs and laboratory tests the death rate prior to initiation of HAART was 15.5%, due to delay in treatment.
The progress of patients under treatment was favorable in terms of general health and immune status and was in accordance with the results of the studies from other developing countries.20,21 Indeed, there was a statistically significant difference between the mean BMI at month 0 (M0), 3, 6, and 9 (P = .004) and between the average rate of CD4 count reported in the same periods (P < .001). This demonstrates the effectiveness of treatment. In addition, 79 patients had achieved the HIV viral load, and it was detectable only in 3 of them. Only 1 patient met the criteria for virologic failure.
Nevertheless, we acknowledge our loss to follow-up despite free health care, laboratory tests, and medicine. Moreover, we did not see all our patients at every appointment.
Mortality remains high (6.25%). Opportunistic infections remain the leading cause of death.11 –13,20,22 The transformation of HIV infection from a lethal disease with eminent death to a chronic disease managed by HAART results in causes of death other than AIDS itself. 23 According to the UNAIDS, fewer people are dying of AIDS-related causes. 1
Conclusion
This study highlights several features of HIV infection in countries with limited resources: screening happening at an advanced stage of infection, as evidenced by the state and advanced immunosuppression symptoms of patients, and the delay by patients in requesting for infection management resulting in high mortality rates in these patients.
This study also confirms the effectiveness of ARV drug combinations used, which is evidenced by the clinical and immune restoration in most of the patients. Nevertheless, we acknowledge our losses to follow-up despite free health care provided to our patients.
Thus, intensified prevention and communication means must be instituted for early diagnosis and treatment, given that about 14.4 million years of life have been saved by the use of ART since 1996.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.