
Abstract
Serodiscussion—the mutual discussion of HIV statuses between sexual partners—can be viewed as an essential prerequisite for risk-reduction behaviors among men who have sex with men (MSM). The current study aimed to assess the prevalence of serodiscussion with one’s most recent sexual partner and its association with sexual behaviors with these partners. Broadcast advertisements were placed on a geosocial-networking smartphone application, encouraging users to complete an online survey. A total of 200 MSM completed the survey. Serodiscussion occurred in 43.5% of dyads, and it was most common in dyads where both partners were reported to be HIV positive, χ2(5) = 60.3, P < .001. Serodiscussion was associated with engagement in both condomless insertive, χ2(1) = 3.847, P = .046, and receptive anal intercourse, χ2(1) = 6.5, P = .011. However, there were no significant differences in how recently a respondent was tested for HIV, representing potentially high-risk scenarios.
Introduction
In the United Kingdom, gay, bisexual, and other men who have sex with men (MSM) accounted for an estimated 37 560 new HIV diagnoses between 1999 and 2013. The number of new diagnoses has risen steadily, reaching an estimated 3250 new infections in 2013, compared to an estimated 1440 new infections in 1999. 1 In 2013, MSM accounted for 80.9% of all new HIV diagnoses. Given that individual-level factors cannot sufficiently explain this increase in new infections, there has been a call to understand health and risk behaviors at multiple levels including the dyadic and network level, 2 such as the extent to which MSM discuss HIV statuses with their sexual partners before engaging in a sexual encounter, 3 hereafter referred to by serodiscussion, 4 and how this affects risk at the dyadic level.
Previously, Winter and colleagues have used the term serodiscussion to refer to “the mutual discussion of HIV status, whether positive or negative” (p. 525) prior to a sexual encounter. 4 It is important to analyze HIV status disclosure as a mutual practice as it is the status of both partners in a sexual partnership or dyad that is critical to adopting informed risk-reduction practices, and that the responsibility for discussing HIV status does not only rest with HIV-positive MSM. Serodiscussion can be viewed as an essential prerequisite for risk-reducing serosorting or seroadaptive behaviors and allows MSM to make informed decisions about their sexual behaviors. 5 Serosorting refers to the practice of seeking to engage in condomless anal intercourse with partners of the same HIV status. 6 Seroadaptation refers to the modification of sexual practices based on the perceived HIV serostatus of sexual partner, where an HIV-negative individual may take the insertive position in condomless anal intercourse with an HIV-positive individual to reduce the risk of transmission. 7
In theory, serosorting and seroadaptation are based on actual serostatus, but infrequent HIV testing, lack of HIV status disclosure, co-occurring sexually transmitted infections, and acute HIV infection with high viral load can impede any potential protective benefits of these practices. In effect, these risk-reduction strategies are based on perceived serostatus. 8 Results related to the effectiveness of serosorting are mixed. Mathematical models parameterized with behavioral data on sexual positioning and risk-reduction strategies among MSM in Sydney, Australia, suggest that serosorting in settings where HIV testing rates are low can be more than double the risk of HIV acquisition. 6 However, models parameterized with similar behavioral data among MSM in Seattle, Washington, suggest that, if serosorting were eliminated as a risk-reduction practice in this population, the HIV prevalence would increase from 16.0% to 24.5%. 9
Sexual encounters between MSM, especially those who are facilitated by the use geosocial-networking smartphone applications, may occur quickly with little discussion of each partner’s HIV status, most recent HIV test, and/or sexual history beforehand, so many may rely on often-incorrect perceptions of what types of people are HIV negative or HIV positive. Little is known about serodiscussion and subsequent risk behaviors among MSM in sexual dyads formed through geosocial-networking smartphone applications. As such, the current study aimed to assess the prevalence of serodiscussion with participants’ most recent sexual partners met through a smartphone application and its associations with sexual risk behaviors with these partners.
Methods
Sample Recruitment
In line with previous research conducted among MSM who use geosocial-networking smartphone applications to meet sexual partners, 10,11 broadcast advertisements were placed on a popular geosocial-networking smartphone application for MSM. In four 24-hour periods in January 2016, users were shown an advertisement with text encouraging them to click through the advertisement to complete a Web-based survey the first time they logged into the application in each of the 24-hour periods. Participants were told that completing the survey would enter them for a chance to win £50. At the end of the recruitment period, 1410 users had clicked through the advertisement and reached the landing page of the survey, and 202 users provided informed consent and completed the survey, representing an overall response rate of 14.3%. The survey included 47 items and took an average of 9.7 minutes (standard deviation [SD] = 5.7) for users to complete. All protocols were approved by the New York University Committee on Activities Involving Human Subjects prior to data collection.
Measures
Respondent and partner demographic characteristics
For both respondents and their most recent partner met through a smartphone application, age was measured continuously in years and then categorized as 18 to 24 years, 25 to 30 years, 31 to 40 years, 41 to 50 years, and 51 years and older. Age concordance was categorized as the partner being older than the respondent, the partner being the same age as the respondent, and the partner being younger than the respondent. For both respondents and their partners, ethnic group membership was categorized as white/white British, black/black British, Asian/Asian British, or mixed/multiple ethnic groups/another ethnic group. Ethnic group concordance was categorized as the partner belonging to the same ethnic group as the respondent or the partner belonging to a different ethnic group than the respondent.
Sexual behaviors and substance use
Respondents were asked whether they had engaged in anal intercourse in the insertive position or in the receptive position with their most recent partner and whether they had performed oral sex on their most recent partner or received oral sex from their most recent partner. Condom use during anal intercourse was dichotomized as condom use or condom nonuse for each position of anal intercourse. Respondents also indicated whether they or their partner had been using alcohol, used inhalant nitrites, used erectile dysfunction drugs, or used stimulant drugs.
Serodiscussion
Serodiscussion was assessed on 1 item based on the existing work assessing the mutual sharing of HIV statuses prior to sexual encounters of dyads of MSM 4 reading, “Did you and this partner share your HIV statuses with each other before you first had sex?” with 2 response options (yes/no).
HIV status and seroconcordance
The HIV status of the respondent was assessed via self-report and categorized as positive, negative, and unknown/never tested. The perceived or suspected HIV status of the partner was assessed via self-report with 7 response options (“I think their status is HIV negative,” “I think their status is HIV positive,” “This partner told me his or her status was HIV negative,” “This partner told me his or her status was HIV positive,” “Someone else told me his or her status was HIV negative,” “Someone else told me his or her status was HIV positive,” and “I do not know their HIV status”). For analytical purposes, these response options were collapsed into 3 categories (positive, negative, or unknown). Seroconcordance was categorized as seroconcordant HIV positive (both partners were reported to be HIV positive), seroconcordant HIV negative (both partners were reported to be HIV negative), serodiscordant (1 partner was reported to be HIV negative and the other partner was reported to be HIV positive), and unknown (the HIV status of 1 or both partners was reported to be unknown).
HIV testing patterns
HIV-negative and HIV-unknown respondents were asked how long it had been since their last HIV test, with 5 response options (less than 3 months, 3-6 months, 6-12 months, more than 12 months, or never tested for HIV). Lifetime HIV testing was categorized as having ever been tested for HIV or having never been tested for HIV. Given that the British HIV Association currently recommends that at-risk MSM should be screened for antibodies at least once per year, 12 recent HIV testing was defined as having been tested most recently within the preceding 12 months or having been tested most recently before the preceding 12 months.
Statistical Analyses
These analyses include 200 dyads, representing 200 survey respondents and their most recent sexual partners whom they met on a geosocial-networking smartphone application. Two (1.0%) participants were removed from the analytical sample as they did not provide any responses to items related to their most recent sexual partner. First, descriptive statistics were calculated for all variables. In line with previous studies of dyad-level data among MSM, 13 -16 associations among respondent demographics, demographic concordance within dyads, sexual behaviors, co-occurring substance use, serodiscussion, and seroconcordance were assessed using χ2 tests of independence. Differences in serodiscussion by HIV testing history and frequency among HIV-uninfected respondents (n = 177) were also assessed using χ2 tests of independence. Statistical significance was determined at P < .05. All analyses were conducted using IBM SPSS version 22.0 (IBM Corporation, Armonk, New York) in February 2016.
Results
Respondent and Partner Demographic Characteristics
The demographic characteristics of respondents and their partners are displayed in Table 1. Participants ranged in age from 18 to 68 years, with an average age of 35.96 years (SD = 11.23), where 39.0% of respondents were 30 years or younger. Most (71.5%) identified their ethnic group as white or white British; 5.5% identified their ethnic group as black or black British, 8.0% identified their ethnic group as Asian or Asian British, and 14.0% identified their ethnic group as mixed, with multiple ethnic groups, or some other ethnic group.
Respondent (n = 200) and Partner (n = 200) Demographics.
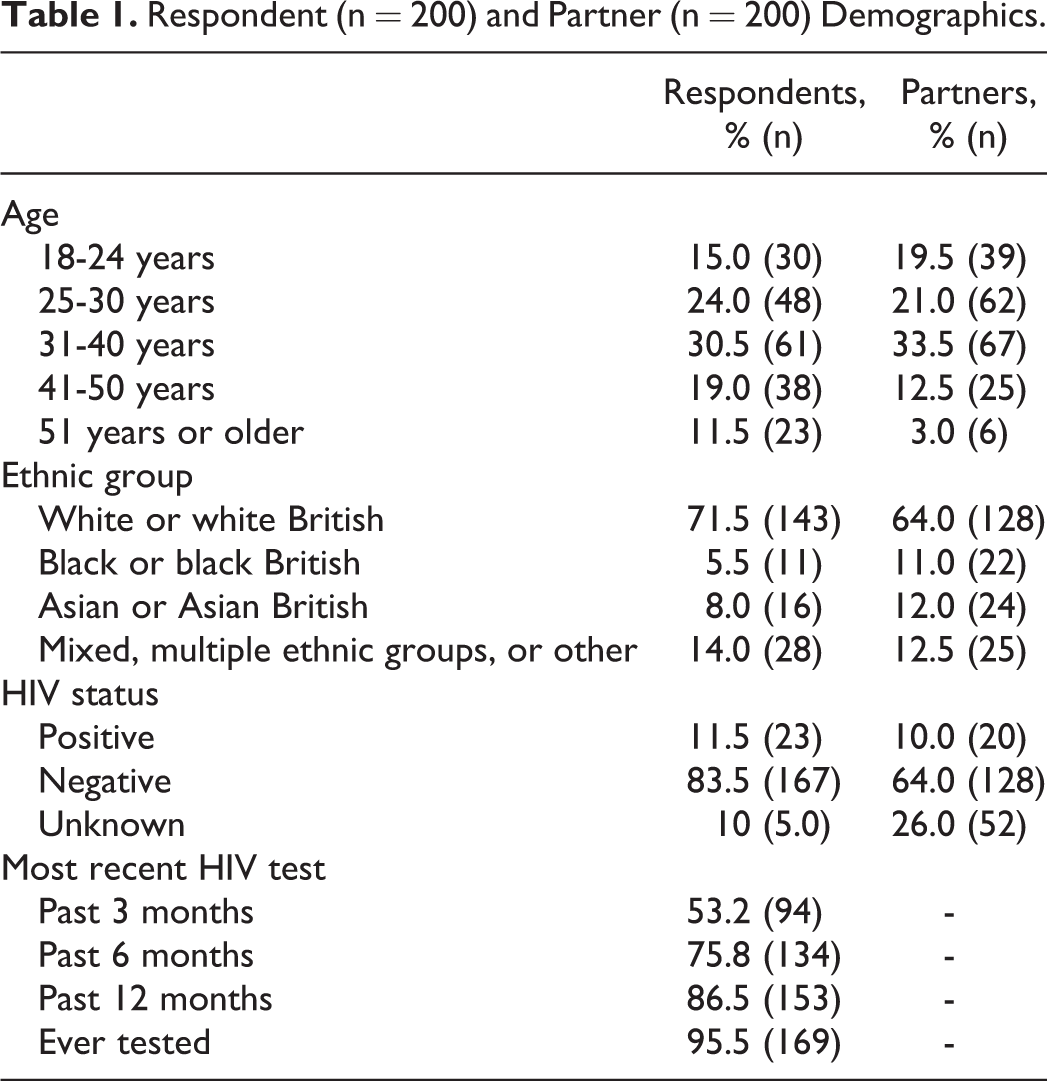
With regard to age, 56.3% of respondents were older than their partners, 37.7% were younger than their partners, and 6.0% were of the same age as their partners. About half (54.5%) of respondents belonged to the same ethnic group as their partner. Partnering with an individual of the same ethnic group was most common among white respondents (65.0%) and black respondents (54.5%), compared to Asian respondents (31.3%) and mixed respondents or respondents belonging to other ethnic groups (17.9%), χ2(3) = 25.1, P < .001. Most (83.5%) reported their HIV status as HIV negative, 11.5% reported their status as HIV positive, and 5.0% reported their status as unknown or having never been tested for HIV.
Sexual Behaviors and Substance Use
About two-thirds of respondents reported having received oral sex from their partner (67.0%) and having performed oral sex on their partner (66.5%). About half engaged in anal intercourse as the insertive partner (46.0%) and as the receptive partner (45.5%). About one-fifth of respondents had engaged in anal intercourse as the insertive partner (17.5%) and as the receptive partner (14.0%) without a condom. One or both partners used inhalant nitrites in one-third (33.0%) of dyads. In about one-fifth of dyads, 1 or both partners used erectile dysfunction drugs (19.0%) or used alcohol (16.0%). Additionally, in 12.5% of dyads, 1 or more partners used stimulants.
There were some significant differences in co-occurring substance use by age. It was most common for respondents aged between 18 and 30 years to report that either 1 or both partners in the dyad were intoxicated during the sexual encounter (28.2%) compared to those of all other ages (8.2%), χ2(4) = 14.3, P = .006. It was most common for respondents aged 41 years and older to report that either 1 or both partners in the dyad used erectile dysfunction drugs during the sexual encounter (42.6%) compared to those of all other ages (8.6%), χ2(4) = 40.7, P < .001. There were no significant associations between age or ethnic group concordance and engagement in particular sexual behaviors or use of particular substances.
Seroconcordance, Serodiscordance, and Sexual Behaviors
Most dyads (62.5%) were classified as seroconcordant, where both partners were reported to be HIV negative in 57.0% of dyads and both partners were reported to be HIV positive in 5.5% of dyads. A small percentage (3.5%) of dyads were classified as serodiscordant, where respondents were HIV positive and partners were HIV negative. In about one-third (34.0%) of dyads, the HIV statuses of 1 or both partners were unknown, where the respondent was reported to be HIV negative and the HIV status of the partner was unknown in 26.5% of dyads, and the respondent was reported to be HIV positive and the HIV status of the partner was unknown in 2.5% of dyads. Table 2 displays the proportion of dyads where the respondent had engaged in condomless receptive anal intercourse and condomless insertive anal intercourse by seroconcordance. Both condomless insertive anal intercourse, χ2(5) = 37.2, P < .001, and condomless receptive anal intercourse, χ2(5) = 13.7, P = .018, were most common among dyads where both partners were HIV positive and were not reported among serodiscordant dyads.
Condomless Behaviors by Seroconcordance.a,b

aCondomless insertive anal intercourse: χ2(5) = 37.150, P < .001.
bCondomless receptive anal intercourse: χ2(5) = 13.715, P = .018.
Serodiscussion, HIV Testing, and Sexual Behaviors
Two-fifths (43.5%) of respondents reported that they and their partner had shared HIV statuses prior to the sexual encounter. Among HIV-uninfected respondents (n = 177), 95.5% had ever been tested for HIV, where 90.5% of those who had ever been tested had been tested in the preceding 12 months. Among those who had never been tested for HIV (n = 8), 12.5% reported their status as negative, with the others reporting their HIV status as unknown. Most respondents reported being tested every 3 months (36.0%) or every 6 months (27.9%). Serodiscussion was most common among dyads in which the respondent had been tested for HIV in the preceding 12 months (58.2% versus 33.3%), χ2(1) = 5.2, P = .023. It was also most common among dyads in which the respondent is tested for HIV every 3 months (69.4%) compared to those tested less frequently (38.7%; χ2(3) = 12.5, P = .006.
Table 3 displays the prevalence of serodiscussion within dyads by seroconcordance, where serodiscussion was most common among seroconcordant HIV-positive dyads (90.0%), χ2(5) = 60.3, P < .001. Serodiscussion was associated with the respondent engaging in insertive anal intercourse without a condom (71.4% versus 53.3%); χ2(1) = 3.8, P = .046, where 71.4% of those who shared HIV statuses with one another engaged in condomless insertive anal intercourse (compared to 53.3% of those who did not share HIV statuses). In addition, sharing of HIV statuses was associated with the respondent engaging in receptive anal intercourse without a condom, χ2(1) = 6.5, P = .011, where 78.6% of those who shared HIV statuses engaged in condomless receptive anal intercourse (compared to 52.9% of those who discuss HIV statuses).
Serodiscussion by Seroconcordance.a

aχ2(5) = 60.311, P < .001.
Discussion
To date, no studies have examined the roles of serodiscussion and seroconcordance among dyads of MSM who use geosocial-networking smartphone applications to meet sexual partners, hence it is difficult to compare these findings. Among a sample of 5410 dyads of MSM who use the Internet to meet sexual partners in the United States, however, serodiscussion occurred in 65% of dyads and condomless anal intercourse occurred in 45% of dyads, 4 compared to 43.5% and 25.5% of dyads, respectively, in the current study. The HIV testing rates were comparable to other samples of MSM who use smartphone applications. In samples of MSM who use geosocial-networking smartphone in New York, 90% had ever been tested for HIV and 71% had been tested within the preceding year, 17 and in Atlanta, 88.1% had ever been tested and 78.6% had been tested in the preceding year, 11 compared to 95.5% and 86.4% in the current sample, respectively.
In this sample of 200 dyads formed through the use of a geosocial-networking smartphone application, less than half (43.5%) of respondents reported a mutual discussion of HIV status prior to sexual activity with their partner, where this was most common in dyads reporting concordant HIV-positive or HIV-negative statuses (76.0%) and discordant HIV status (71.4%). In dyads where the respondents reported their HIV status as negative, serodiscussion was most common among those who had been tested recently and most frequently, potentially reflecting more confidence in the absence of HIV infection. Engagement in both condomless insertive and receptive anal intercourse by the respondent was associated with serodiscussion and were most common in dyads reporting concordant HIV-positive statuses and least common in dyads reporting discordant HIV statuses. However, condomless anal intercourse was common among dyads where the HIV status of 1 or both partners was unknown (14.7% and 13.2% for insertive and receptive anal intercourse, respectively), and given that 87.5% of respondents who had never been tested for HIV reported their status as unknown, these dyads represent potentially high-risk partnerships where an HIV-infection-unaware partner may transmit HIV to his or her partner.
These findings have implications for the promotion of HIV testing among at-risk MSM and of the mutual discussion of HIV status and testing between partners, allowing them to make informed seroadaptive decisions about their sexual behaviors and reduce risk of transmission or acquisition of HIV. Broader efforts are needed to understand and address barriers to accessing HIV testing or discussion of HIV status and testing between partners. For example, the stigmatizing nature of HIV is a factor that affects delayed HIV testing by at-risk individuals 18 or the disclosure of HIV status by individuals living with HIV, 18 so there may be opportunities to improve HIV testing coverage and serodiscussion among MSM through the development and implementation of interventions to reduce HIV-related stigma.
These findings should be considered in light of their limitations. First, the current sample is a relatively small sample of 200 MSM in London recruited exclusively from a single geosocial-networking smartphone application and their most recent sexual partner met on such an application. As such, the findings may not be generalizable to MSM who use other geosocial-networking smartphone applications or who use these applications in other large European cities. Future research should be conducted with larger numbers of dyads and inquire more about the most recent sexual encounter per respondent. A substantial percentage (85.7%) of individuals who saw the broadcast advertisement and clicked on it did not complete the survey, so the sample is likely to be biased by some degree of self-selection. The HIV status was assessed by self-report, and HIV testing patterns were collected only from the respondents, so there may be misclassification related to sexual risk or seroconcordance in HIV-infection-unaware respondents or their partners. Based on previous work among dyads of MSM, measures of partner-reported age and race are likely to be accurate; however, certain self-reported sexual behaviors (eg, condom use) may be unreliable and differentially reported by ethnic group. 19 Additionally, while there may be some underreporting of substance use due to social desirability bias, the survey was administered anonymously so the answers may more likely reflect actual behaviors.
Although both serodiscussion and seroconcordance were associated with engagement in condomless receptive and insertive anal intercourse with an individual’s most recent sexual partner met on a geosocial-networking smartphone application, there were no significant differences in condomless anal intercourse behaviors based on how recently or frequently the respondent was tested for HIV, representing potentially high-risk partnerships where the virus may be transmitted by an HIV-infection-unaware partner. Further efforts should be made to increase HIV testing coverage among MSM to improve accurate and honest serodiscussion.
Footnotes
Authors’ Note
All procedures performed in studies involving human participant were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants who were included in the study.
Acknowledgments
The authors thank the participants for their contributions to the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by an individual research grant from the New York University College of Arts and Science Dean’s Undergraduate Research Fund (principal investigator: William C. Goedel) and by the New York University School of Medicine. Dr Dustin T. Duncan was funded by his New York University School of Medicine Start-Up Research Fund to work on this project. Dr John A. Schneider was supported by grants from the National Institute of Mental Health (Grant # 5R01MH100021; principal investigator John A. Schneider, MD, MPH) and the National Institute of Allergies and Infectious Diseases (Grant #1R21AI118998; principal investigator John A. Schneider, MD, MPH).