
Abstract
The objective of this report was to assess Georgia’s progress toward Joint United Nations Programme on HIV/AIDS 90-90-90 targets over the period between 2011 and 2015. The number of HIV-positive persons was estimated using Spectrum software. Number of persons diagnosed, on antiretroviral therapy (ART) and virally suppressed were quantified using data from the national AIDS health information system. By the end of 2015, out of the estimated 7100 persons living with HIV, 62% were diagnosed, 38% were on ART, and 32% were virally suppressed. There were improvements in each stage of cascade from 2011 to 2015: the proportion of diagnosed persons increased from 46% to 61%, ART coverage among diagnosed persons increased from 46% to 62%, and the proportion of virally suppressed patients among those on ART increased from 74% to 85%. Despite the progress, additional efforts are needed to reach the 90-90-90 targets. Reducing the number of people living with undiagnosed HIV will be critical for achieving goals.
Introduction
The ability of antiretroviral therapy (ART) to save lives and prevent new infections 1,2 led Joint United Nations Programme on HIV/AIDS (UNAIDS) to set 90-90-90 targets, which aims to diagnose 90% of people living with HIV (PLWH), to treat 90% of those diagnosed, and to achieve viral suppression in 90% of those on treatment by 2020. 3 The number of people receiving ART globally dramatically increased over the last decade, reaching 15.8 million by mid-2015. 4 This is one of the greatest public health achievements of recent periods, which however requires further scale-up of ART toward reaching the 90-90-90 targets.
Georgia is an independent nation located in Eastern Europe. The first case of HIV infection in Georgia was identified in 1989. By the end of 2015, a cumulative 5412 cases were reported that included 1073 cases of death. The national HIV response was substantially strengthened since 2004 through the support provided by the Global Fund to Fight AIDS, Tuberculosis, and Malaria. Currently HIV testing activities are delivered through community-based programs for key populations (people who inject drugs [PWIDs], men who have sex with men [MSM], female sex workers [FSWs]) and through-facility based programs, including HIV indicator diseases guided testing, universal screening of pregnant women, and mandatory screening of blood donors.
Georgian model of HIV care includes provision of comprehensive package of services including ART and management of opportunistic infections and comorbidities, such as viral hepatitis, tuberculosis, and drug addiction. Although in 2011 ART was recommended for patients with a CD4 count <200 cells/mm 3 , the threshold was moved to <350 cells/mm3 by 2012, and then to <500 cells/mm3 by the end of 2013. Following the results of the landmark Strategic Timing of Antiretroviral Therapy (START) trial and updated World Health Organization recommendations, 5,6 at the end of 2015 Georgia implemented treat all policy offering ART to all HIV-positive persons regardless of CD4 count or disease stage. The standard of ART relies on regular monitoring of HIV viral load and CD4 count at least every 6 months. In addition to medical care, support services are also available, including adherence counseling and monitoring. All services are provided free of charge to patients.
The objective of this report was to assess Georgia’s progress toward 90-90-90 targets and to identify gaps in the continuum of HIV care.
Methods
We constructed HIV care cascades for each 90-90-90 targets for the period of 2011 to 2015. Diagnosed was defined as positive HIV test result by any method and confirmed by a positive Western blot or nucleic acid–based test. Being on ART was defined as at least 1 documented prescription refill of antiretroviral drugs within 3 months prior to the end of calendar year. Suppressed was defined as plasma HIV RNA level of <1000 copies/mL at the last viral load measurement.
The number of HIV-positive persons was estimated using Spectrum/Estimation and Projection Package (EPP; version 5.31). We used spectrum file created in 2015 and submitted to UNAIDS as part of Global AIDS Response Progress Reporting.
Data for remaining steps of HIV care cascade were quantified using the national AIDS health information system (AIDS HIS), which is the secure Web-based system collecting information on every case of HIV infection reported in Georgia.
Results
Spectrum-derived estimates of HIV-positive persons and AIDS HIS-derived counts of persons who were diagnosed, on ART and virally suppressed are summarized in Figure 1. The proportion of diagnosed persons increased from 46% in 2011 to 61% in 2015 (P < .0001). Improvements in diagnosis were statistically significant for each subsequent year.

Treatment cascade in Georgia, 2011 to 2015.
The number of patients on treatment increased by 147% over the 5-year period (P < .0001), reaching 38% coverage in total population in 2015 (Figure 1). Among diagnosed persons, ART coverage increased from 46% in 2011 to 62% in 2015 (P < .0001; Table 1). The difference was statistically significant for each subsequent year except the difference between 2014 and 2015. Disengagement from care was the reason of not being on ART in 32% of diagnosed population in 2011 and this decreased to 21% in 2015 (P < .0001).
Achievement of Individual 90-90-90 Targets.
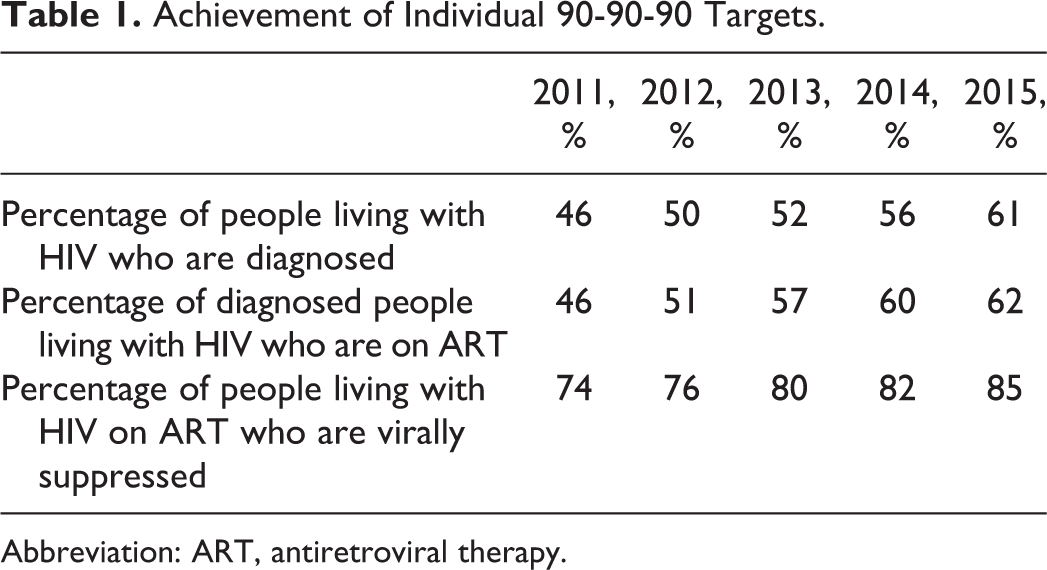
Abbreviation: ART, antiretroviral therapy.
The proportion of patients achieving viral suppression increased from 16% in 2011 to 32% in 2015 (P < .0001; Figure 1). Among persons on ART rates of viral suppression increased from 74% in 2011 to 85% in 2015 (P < .0001; Table 1).
By the end of 2015, out of the estimated number of HIV-positive persons 4826 were not virally suppressed, among which 2761 (57%) were not diagnosed, 931 (19%) were disengaged from care, 723 (15%) were in care but not on ART, and 411 (9%) were on ART without viral suppression because of either nonadherence or recent initiation of ART.
Discussion
Engagement in HIV treatment cascade has been improving in Georgia, with the proportion of HIV-positive persons who are diagnosed, on ART and virally suppressed, increasing annually. However, the current pace of improvement will not be sufficient to reach the 90-90-90 targets by 2020. The global progress toward these targets varies substantially between countries and regions. For example, ART coverage in Eastern Europe is as low as 19% of total HIV-positive population, with proportion of virally suppressed persons ranging from 9% in Russia to 32% in Georgia. 7,8 On the other hand countries of Western Europe are close to achieving targets with up to 70% of HIV-positive persons maintaining viral suppression. 9 –11 United Nations Programme on HIV/AIDS estimates that only 32% of PLWH are virally suppressed in sub-Saharan Africa 7 ; however, recent study from rural Malawi reported higher rates of viral suppression reaching 62% of HIV-positive population. 12 The study from Malawi highlights that ambitious targets set by UNAIDS are achievable in resource-limited settings.
Despite the improvements, the stage of HIV diagnosis remains the major gap in Georgia’s treatment cascade, with 39% of estimated number of PLWH unaware of their HIV status in 2015. This has profound negative effect on the entire continuum, with undiagnosed HIV accounting for 57% of persons without viral suppression. This gap in diagnosis is the result of low HIV testing coverage of key populations at risk and missed opportunities to diagnose infection in health-care settings. According to the recent country progress report, only 26% of PWIDs, 44% of MSM, and 52% of FSWs were screened for HIV in the previous year. 13 It is clear that unless HIV testing efforts are substantially scaled up, the first “90” target will not be reached.
Another important challenge is disengagement from care. The proportion of patients not in care decreased over time, but yet 21% of diagnosed patients in 2015 were lost and this affects all subsequent stages of care and first of all the second “90” target of treating 90% of diagnosed population by 2020. Previously we showed that persons with baseline CD4 count of greater than 350 cells/mm3 were at higher risk of attrition from care. 14 Evolving treatment initiation criteria toward earlier start of ART helped to increase ART coverage and reduce attrition; and recent implementation of treat all policy is expected to have greater effect. But the fact that only 62% of diagnosed persons are on ART underlines that more proactive approaches will be needed to ensure that diagnosed patients are linked to care, started on treatment, and retained in care, including through community involvement. 15
Georgia appears to be closest to achieving the third “90” target, with 85% of persons on ART already suppressed in 2015. However, there are some issues to consider. Effectiveness of ART depends on durable viral suppression to be maintained over extended periods of time. Our analysis was a cross-sectional assessment of situation and hence did not capture longitudinal dynamics in terms of maintaining viral suppression. The proportion of persons with viral suppression would decrease if we used lower threshold for defining viral suppression compared to the one used in our analysis of <1000. On the other hand, the proportion of suppressed cases would be greater if we limited our analysis to patients who were on ART for at least 6 or 12 months.
Improving engagement in HIV care continuum will not be possible without achieving another UNAIDS target of 0 discrimination. Although PLWH have unrestricted access to HIV clinical services, stigma and discrimination have been cited as important barriers to access prevention and testing services for key populations at risk. 16 The national HIV/AIDS strategy recommends specific activities to address stigma and discrimination, including through greater involvement of communities. 16
Our report has limitations that needs to be mentioned. The report primarily is descriptive and does not provide analytical insights into reasons for existing gaps in various stages of care. We did not have information on engagement in HIV care continuum by key populations at risk and thus were not able to look at the difference between subpopulations. Nevertheless, this article provides an accurate snapshot of current situation and identifies areas where interventions will have the greatest effect. Reducing the number of people living with undiagnosed HIV and eliminating disengagement from care will be critical for achieving the 90-90-90 targets in Georgia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.