
Abstract
Objectives:
To examine the relationship between retention in continuous care and sustained viral suppression.
Methods:
The authors retrospectively followed 653 persons who were virally suppressed and seeking care at an infectious disease clinic in Kentucky for an average of 6 years to determine the rates of retention in medical care (≥2 visits separated by ≥3 months within a 12-month period) and sustained viral suppression (<400 copies/mL). A generalized linear mixed model was used to determine an association between retention and suppression over time.
Results:
Approximately 61% of the study population were retained in continuous care and 75% had sustained viral suppression for all patient-years. Persons retained in care were 3 times the odds of sustaining viral suppression over time (P < .001).
Conclusion:
Retention is essential to achieving and maintaining viral suppression. Strategies should be set in place that emphasize increasing the rates of retention, which in turn may increase the rates of suppression.
Introduction
Achieving and sustaining viral suppression is essential for persons living with HIV. Not only does achieving viral suppression reduce morbidity and mortality due to HIV, it also reduces one’s risk of transmitting the virus to others. 1 Even so, in the United States, a large percentage of persons living with HIV (PLWH) have not achieved viral suppression. It is estimated that in the United States, approximately 1.2 million people are living with HIV; and of those, 70% have not achieved viral suppression. 1 There are many factors that may contribute to individuals not achieving viral suppression, including not being aware of their infection and not being engaged in care (ie, retention in care). 1,2
Engagement in HIV care is imperative for all PLWH, as this greatly improves the opportunity to achieve viral suppression. Specifically, retention in continuous HIV care is an important piece in the engagement in care continuum, as poor retention poses an arduous obstacle in increasing the percentage of persons with a suppressed viral load. 1 -4 However, approximately one-half or more of PLWH are not retained in continuous care after being diagnosed and linked to care. 1,5,6 Approximately two-thirds of those that did not have a suppressed viral load were not engaged in care, whereas 76% of those that were engaged in care were virally suppressed, suggesting the importance retention in care plays in the management of HIV disease. 1
When an individual suppresses his or her viral load, it is important that he or she maintains suppression. Over time, a large proportion of patients have viral loads that rise above detectable levels after initial suppression. 7 -10 Similarly, the proportion of those retained in continuous care may decrease over time. 11,12 Continuing to understand the association between retention in continuous care and sustained viral suppression is important. The purpose of this study was to examine the effects of retention in continuous HIV care and other factors on sustained viral suppression among Kentuckians living with HIV.
Methods
Study Design
We retrospectively evaluated patients who were diagnosed with HIV and sought HIV medical care at an urban, academic infectious disease clinic between 2003 and 2011. The clinic is a multidisciplinary, urban, and academic infectious disease clinic located in Kentucky. Over half of the patient population lives in rural areas. Patients who sought care and provided complete data between 2003 and 2011 were eligible for the study. Patients who were virally suppressed (viral load <400 copies/mL) for the first time during the study period were followed for at least 12 months after the initial viral suppression to examine the rates of sustained viral suppression. The institutional review board approved this study.
Study Population and Eligibility
Patients eligible for the study were those who sought care at the clinic between 2003 and 2011, were diagnosed with HIV, and were ≥18 years of age. Patients were included in the study if they were currently on antiretroviral therapy (ART), had a suppressed viral load at least once during the study period, and the initial suppression date allowed for at least 1 year of follow-up. If a patient had missing diagnosis or clinic visit dates, they were excluded from the analysis. Each patient included in the study was followed for 12-month intervals from the time of their first suppressed viral load until the end of the study period, death, or movement out of the service region. The follow-up period extended through December 31, 2011.
Study Measures
Demographic and clinical data for each patient were abstracted from all medical records. Demographic data collected at baseline included date of birth, sex, race (white and nonwhite), marital status (single, married, widowed, and divorced), employment status (employed, unemployed, and retired/disabled), HIV risk behavior (men who have sex with men [MSM], heterosexual, injection drug user [IDU], and others), annual income (≤US$10 000 and >US$10 000), insurance type (private, Medicare, Medicaid, and none), and current tobacco use, alcohol use, and/or illicit drug use. Clinical data collected at baseline and/or during the follow-up included viral load, CD4 counts, depression, AIDS diagnosis, and hepatitis C diagnosis. After each 12-month follow-up period, viral loads were collected to determine viral suppression.
The primary independent variable of interest for this study was retention in continuous care. Retention in continuous care was defined, using the Institutes of Medicine’s core indicator, as having ≥2 clinic visits separated by at least 3 months within a 12-month period. 13,14 Whether a patient met the retention criteria or not (yes/no) was observed for each year the patient was in the study. The percentage of patient-years where an individual was retained in continuous care was calculated; patients were considered optimally retained in continuous care if they maintained retention 100% of the time while in the study.
Outcome Measure
The outcome measure of interest for this study was sustained viral suppression. Viral suppression was defined as having a viral load <400 copies/mL. Viral loads were captured for each patient at the end of each 1-year period (±90 days). The percentage of patient-years where a patient was virally suppressed was calculated; sustained viral suppression was defined as maintaining a suppressed viral for all yearly intervals observed (100%).
Statistical Analysis
To assess trends in viral suppression and retention in care among the entire group, the proportions of patients with a suppressed viral load and meeting the retention criteria in each study year period were calculated. Descriptive statistics were conducted to describe the cohort, with means, standard deviations (SD), medians, and interquartile ranges (IQR) calculated for all continuous variables and frequencies and percentages calculated for all categorical variables. For the bivariate analysis, χ2 tests were performed to determine the differences between sustained suppression and categorical variables, whereas independent 2-sample t tests and Wilcoxon rank sum test (when appropriate) were conducted to determine the differences between sustained suppression and continuous variables.
A generalized linear mixed model (GLMM), using a logit link function, was used to determine the factors associated with sustained viral suppression over time; in particular, retention in care. A GLMM was used for this study due to the nonnormal data and the repeated measures per individual. To account for random variation between individuals, we employed a random intercepts model. The fixed effects were included in the model as well (eg, age, sex, race, income). The Gauss-Hermite quadrature method was used for the likelihood approximation and the random intercepts model estimated the probability of sustaining a suppressed viral load. Known confounders and variables with a P values ≤.15 in the bivariate analysis were initially included in the model and confounders and variables with a P value <.05 were retained in the model. In this model, retention in care and depression were observed as time-varying factors. All data were analyzed using SAS version 9.4, and P values <.05 were regarded as statistically significant.
Results
A total of 653 patients, who were on ART and virally suppressed at any time between 2003 and 2011, were included in the study. The mean age at first suppression was 40.4 years (SD = 9.4). The majority of the patients were male (82.9%), white (76.3%), single (70.4%), and reported MSM as their HIV risk behavior (59.7%). Over half (54.4%) of the patients who were suppressed and sought care during this time period had annual incomes ≤US$10 000, and almost one-third of the patients were uninsured. Approximately 61% of the patients were diagnosed with AIDS and 42% were diagnosed with depression during the study period (Table 1).
Association of Demographic Characteristics and Sustained Viral Suppression among Patients Virally Suppressed and Seeking HIV Medical Care in Kentucky, 2003-2011.a
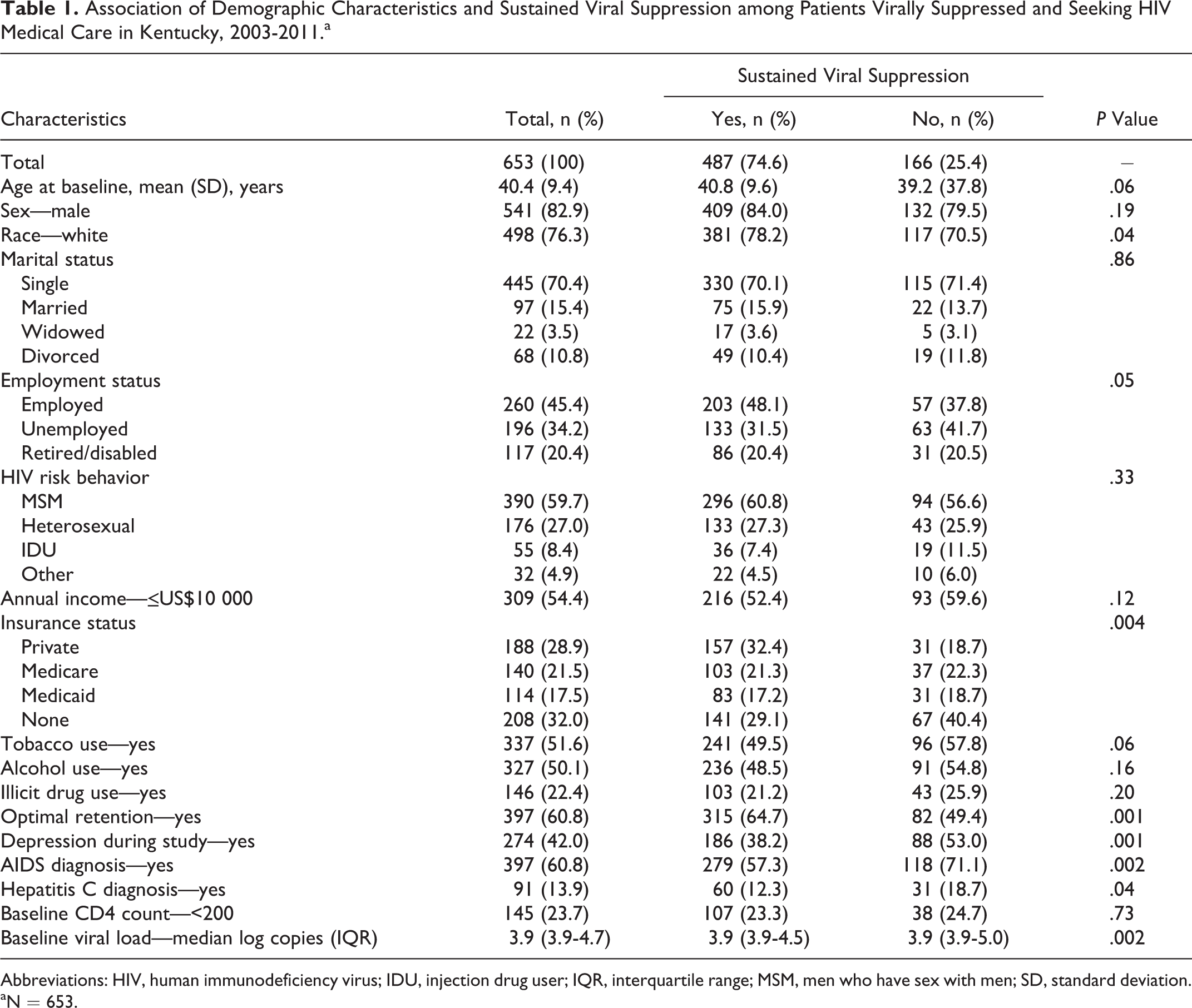
Abbreviations: HIV, human immunodeficiency virus; IDU, injection drug user; IQR, interquartile range; MSM, men who have sex with men; SD, standard deviation.
aN = 653.
The average follow-up time after viral suppression was 6.2 years (SD = 2.5; range = 1-8) and the average number of outpatient clinic visits attended during this follow-up period was 9.4 visits (SD = 8.0; range = 1-80). The rate of retention among this cohort ranged from 94.3% in year 1 to 76.1% in year 8 (Ptrend ≤ .0001); however, the average overall rate of retention was 81.9% (SD = 28.9). Overall, approximately 61% of the patients were optimally retained in continuous care (Table 1). Optimal retainers were more likely to be older, MSM, privately insured or on Medicare, and have an annual income >US$10 000, compared to their counterparts.
Overall, the average percentage of patient-years an individual was virally suppressed was 87.5% (SD = 26.2). The proportion of patients virally suppressed remained steady over time, with a slight increase from 2004 (88.5%) to 2011 (92.3%; Ptrend = .04). A total of 487 (74.6%) patients, with suppressed viral loads, maintained suppression throughout the course of the study. Individuals with sustained suppression were more likely to be optimal retainers in care compared to their counterparts (64.7% versus 49.4%; P = .001). Also, those with sustained viral suppression were more likely to be white (78.2% versus 70.5%; P = .04), employed (48.1% versus 37.8%; P = .05), and privately insured (32.4% versus 18.7%; P = .004). Sustained suppression was less likely to be observed among the uninsured (29.1% versus 40.4%; P = .004), those diagnosed with depression (38.2% versus 53.0%; P = .001), those diagnosed with AIDS (57.3% versus 71.1%; P = .002), and those diagnosed with hepatitis C (12.3% versus 18.7%; P = .04; Table 1).
A GLMM was performed to determine which factors were associated with sustained viral suppression over time, in particular retention in continuous care. Table 2 presents the associations between each factor and sustained suppression. The results suggest that individuals who were optimally retained in continuous care had greater odds of sustaining suppressed viral loads. While controlling for all other variables in the model, an individual who retained in continuous care throughout the course of the study were almost 3 times the odds of sustaining a suppressed viral load compared to those not retained in continuous care over time (odds ratio [OR]: 2.97; 95% confidence interval [CI]: 1.65-5.32). Also, those at greater odds of sustaining a suppressed viral load were found among older patients (OR: 1.05; 95% CI: 1.01-1.08) and those privately insured compared to those not insured (OR: 2.32; 95% CI: 1.07-5.02). Nonwhites, which consisted of blacks and Hispanics, were at much lower odds of sustained suppression over time compared to whites (OR: 0.51; 95% CI: 0.26-0.98). In addition, those with depression, AIDS, or hepatitis C were at lower odds of sustaining suppressed viral loads compared to their counterparts (Table 2).
Generalized Linear Mixed Model to Determine Sustained Viral Suppression over Time among Patients Virally Suppressed and Seeking Care in Kentucky, 2003-2011.a,b

Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; GLMM, generalized linear mixed model.
aN = 613.
bGLMM controlled for year in study.
cTime-varying factors.
Discussion
In this study, we examined the factors that were associated with sustained viral suppression, in particular retention in continuous care. We retrospectively followed 653 patients who were virally suppressed and seeking medical care for an average of 6 years to determine the rates of retention and sustained suppression. Among the 653 patients included in the study, optimal retainers were at increased odds of sustaining viral suppression over time compared to those not retained in care. The results of this study suggest that seeking continuous care even after viral suppression is vital, and this can help maintain viral suppression over time. In this study, we showed that approximately 75% of the cohort had sustained viral suppression for all patient-years observed. There were also significant increases in the rates of suppression as the rates increased from 88% in year 1 to 95% in year 8. Our study results corroborate other studies that have shown significant increases in the rates of suppression over time. 15 -18 Yehia et al showed significant increases in the rates of sustained suppression among 483 patients who received care between 2001 and 2010; the rates of suppression increased from 45% in 2001 to 72% in 2010. 15 Westergaard et al conducted a study among HIV-infected IDUs and observed that the rates of suppression increased from 15.7% in 1998 to 60% in 2011. 16
Our rates of suppression were slightly higher compared to other studies that observed sustained suppression. 1,3,15,16,19,20 This could be due to our definition of viral suppression (ie, <400 copies/mL). To maintain consistency between those who initiated care at earlier time period and those who initiated care at later time periods, we stuck with <400 copies/mL as the cutoff. Other studies have used <50, <200, or <500 copies/mL as their cutoff for suppression. Because of this inconsistency, it is difficult to compare studies. Although not shown, a sensitivity analysis was conducted comparing the different measurement levels, and the results remained the same.
Improved rates of sustained suppression were found among those who sought continuous care (ie, retention) compared to those who did not. In our study, approximately 61% of the cohort met the retention criteria in all patient-years. This retention rate falls within the range of other studies as researchers have shown retention rates ranging between 30% and 90%. 1,6,13,17,20 -23 Retention in continuous care after initial viral suppression increased the odds of sustained viral suppression. This shows the importance of retaining in care even after achieving viral suppression. It is suggested that individuals living with HIV who have achieved viral suppression should attend a clinic visit at least once every 6 months. 24 Those individuals that do not seek continuous care risk the chance of their viral loads rising above detectable levels, and from a public health standpoint, this is extremely important as this could increase their risk of transmitting the virus onto others. 25 The results of the current study are similar to other studies that have shown poor retention to be associated with low rates of viral suppression. 4,12,17,26 In a similar study, Crawford showed that suboptimal retainers, compared to optimal retainers, had twice the odds of experiencing a viral rebound (viral load >400 copies/mL) after initial viral suppression. 4 Retaining PLWH in continuous care is essential in order to increase the percentage of persons who achieve viral suppression. Researchers and clinicians should direct their focus and interventions to improving retention in care, such as service delivery interventions. 27,28
Poor rates of sustained viral suppression were found among younger patients, nonwhites, those uninsured, and those with an HIV diagnosis. This is similar to other studies that have observed factors related to viral suppression. 15 -18,29 Similar to other studies, nonwhites have a harder time suppressing their viral loads. 26,29 This could be due to multiple reasons, in particular retention in care. Although not shown, nonwhites were less likely to be optimally retained in care compared to whites. This could explain poor rates of sustained suppression among this group. Blacks and Hispanics were grouped into nonwhites due to the small sample sizes as the HIV population in Kentucky is predominately white and non-Hispanic.
An interesting result was that those who were diagnosed with depression had lower odds of sustained suppression compared to those who were not depressed. A large proportion (42%) of our cohort were diagnosed with depression throughout the study period. Depression among PLWH is not uncommon, but only a small number of researchers have observed the effect depression has on HIV outcomes. 30 -32 It is important to make sure these individuals are getting the care they need to address their depression and this in turn may have a positive effect on their viral suppression.
There were a few limitations to the current study. The study was an observational, retrospective cohort study. Due to the retrospective nature of this study, we can only discuss association and not causation. Also, the study was subjected to uncontrolled confounders for which we did not have any information (eg, education). Another limitation of this study is that we did not obtain data on medication adherence. This information was not captured in the medical records and therefore we were not able to look at the association between sustained suppression and medication adherence. Also, our results may not be generalizable to all PLWH receiving ART. The strength of this study is that we looked at the longitudinal nature of retention in continuous care and viral suppression among individuals who achieved a suppressed viral load.
In conclusion, the results of this study carry significant implications for clinical outcomes of PLWH as well as future public health prevention efforts. Retention in HIV medical care plays a central role in sustaining viral suppression. The results of this study showed that individuals who are retained in care over time have greater odds of sustaining viral suppression compared to their counterparts. Interventions should be set in place that put an emphasis on increasing rates of retention in care which in turn increases the rates of viral suppression.
Footnotes
Authors’ Note
The results of this study were partially presented at the 2014 American Public Health Association’s Annual Meeting; New Orleans, Louisiana.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.