
Abstract
Background:
The authors aimed to compare TST with QuantiFERON-TB Gold In-Tube (QFT) for detecting latent tuberculosis infection (LTBI) in HIV-infected patients in Iran as a TB-medium endemic country.
Methods:
In a cross-sectional design,130 HIV-positive patients in HIV clinic of Tehran University were studied. Patients screened for LTBI with QFT and TST simultaneously. Concordance between 2 tests results and variables associated with tests discordance were assessed.
Results:
Positive results found in 24.6% for TST and 7.7% for QFT. Overall agreement between them was 73.85% (Kappa = 0.083). History of imprisonment was associated with more positive TST (P = 0.014) and QFT (P = 0.01). Patients with intravenous drug use (IDU) history had significant discordant results (0.018).
Conclusion:
The authors recommend QFT for all negative cases of TST in HIV-positive patients especially who had history of IDU.
Introduction
Tuberculosis (TB) is one of the most common causes of death in HIV-infected patients. It usually results from reactivation of previous latent infection. HIV infection is also a risk factor for progression of latent TB infection (LTBI) to its active form. 1 Detecting LTBI in HIV-positive patients is recommended as the best strategy to control this progression. 2
Tuberculin skin test (TST) has been the only tool to diagnose LTBI. The main advantage of TST is its low cost, but there are some limitations. Some patients may not return to read the result; interpreting results need expertise. Development of T-cell-based assays has led to some new tests such as interferon (IFN) γ release assays (IGRAs), allowing measurement of IFN-γ, which is released from T cells following stimulation by 2 unique antigens of mycobacterium TB (MTB). These antigens are early secreted antigenic target 6 (ESAT-6) and culture filtrate protein 10 (CFP-10). 3
Interferon γ release assays appear to be more specific for MTB than TST, because the antigens used in IGRAs are more specific than those used in TST (purified protein derivate [PPD]). These antigens do not cross-react with strains in any BCG vaccine or most non-TB mycobacteria, so IGRAs are not confounded by past BCG vaccination. 4 –11,12 The IGRA tests, of which the QuantiFERON-TB Gold In-Tube Test (QFT) is a commonly used kit, need 1 visit, and the reliability of negative and positive results is increased by negative (nil) and positive (mitogen) controls. 13 The Centers for Disease Control recommends using these assays to detect MTB infection in some circumstances. 14
Some studies have compared these 2 tests in different circumstances for concordance. The decision to use either test depends on resources and logistical considerations and is best provided by national guidelines of each country. 15 There are a few studies on performance of IGRAs in HIV-positive patients. Most of them have reported discordance with TST results. 5,7,8,16
We designed this study to compare IGRA with TST for diagnosis of latent TB in HIV-positive patients in Iran, which is a medium-TB burden country. The results could be useful in developing related guidance.
Methods
Study Design, Setting, and Population
In a cross-sectional study from January 2013 to May 2013, a total of 150 HIV-positive patients participated in the study. They were selected from Tehran University of Medical Science’s HIV clinic. The study was approved by the ethics committee of Tehran University of Medical Sciences, and all the patients provided written informed consent.
Demographic and clinical data of the patients including sex, age, route of transmission, time from diagnosis of HIV infection, CD4 count, antiretroviral treatment (ART), BCG vaccination status, history of TB contact, other underlying immunosuppressive diseases, immunosuppressant drug use, and history of incarceration were recorded. Chest X-ray and sputum smear for bacillus Koch (BK) was performed 3 times in all patients to rule out active TB infection.
Patients with active TB, past history of TB and chemoprophylaxis, and no re-entry for recording the TST results were excluded from the study. Diagnosis of active TB was based on the results of history and clinical examination, radiological finding, and/or isolation of MTB from sputum.
Procedures
A conventional TST was performed for every patient, and a blood sample for measurement of the QFT was taken simultaneously. Tuberculin skin test was performed by injecting 0.1 mL of 5-unit PPD solution by the Mantoux method. 17 The skin induration was measured (in mm) 48 to 72 hours after the inoculation by a trained health care provider. We considered skin indurations positive if they were equal or higher than 5 mm.5 To detect booster effect, all patients with a negative TST were retested after 1 to 3 weeks. Booster test was defined as positive if the induration measures 5 mm or greater.
Three milliliters of whole blood sample were obtained from each patient. The samples were treated as recommended by the manufacturer. Whole blood was sampled in each of the 3 QFT tubes containing TB-specific antigen (ESAT-6, CFP-10, and TB7.7), a phytohemagglutinin as positive control, and a null control. The tubes were stored at 4°C to 25°C and far from sunlight. After vigorous shaking of the tubes, they were sent to the laboratory within 6 hours after acquisition. Samples incubated at 37°C for 16 to 20 hours and then were centrifuged for 15 minutes at 2000 to 3000 rates. The harvested plasma was stored at −70°C before quantification of the IFN-γ level by enzyme-linked immunosorbent assay method according to manufacturer’s instructions (Cellestis, Carnegie, Australia). On the basis of specific software provided by the manufacturer, the results were considered positive, negative, or indeterminate.
Statistical Analysis
Data analysis was done using the version 19 of SPSS software package (SPSS Inc, Chicago, Illinois). Variables were analyzed using frequencies and percentages for categorical variables and means or medians for continuous measures. Associations between variables were evaluated by using Fisher exact test and chi-square tests for categorical variables and t tests or Wilcoxon rank-sum tests for continuous variables depending on whether the data were normally distributed. Logistic regression analysis was used for identifying factors associated with concordance and discordance results.
Concordance between TST and QFT was assessed by κ coefficient. Strength of agreement was considered “optimal” for 0.80 < κ ≤ 1.00, “substantial” for 0.60 < κ ≤ 0.80, “moderate” for 0.40 < κ ≤ 0.60, “fair” for 0.20 < κ ≤ 0.40, and “poor” for κ ≤ 0.2. 18
Results
Study Population
One hundred fifty participants were screened. Twenty patients of initial participants were excluded and we included 130 participants in our study during the study period. Two patients of excluded participants had past history of TB, 2 of them had active TB, and 10 others had past history of chemoprophylaxis. Six patients were excluded because of no reentry for recording TST results.
All patients had positive history of BCG vaccination at birth. The mean (± standard deviation) age of the participants was 37.1 ± 8.6, ranging from 19 to 71 years and most of them (79.2%) were 25 to 45 years old; 56.2% were male, 59.2% had history of tobacco smoking, and 47 (36.2%) patients had history of intravenous drug use (IDU). Two patients had history of TB contact. Most of the participants were on ART (80%) for at least 1 month. The median of CD4 count was 377 cells/mm3 (range 10-1600) and 24.7% of them had CD4 count < 200 cells/mm3. Mean duration of HIV diagnosis was 31.2 ± 25.8 months. We had no patients with underlying immune-suppressed diseases or being on immunosuppressant.
Test Results
A total of 32 (24.6%) participants had a positive TST with the induration range of 5 to 35 mm (mean = 8.5 ± 5.9 mm). All 98 (75.4%) patients with negative TST had negative retest results. Ten (7.7%) patients had a positive QFT and 120 (92.3%) had a negative QFT. We had no indeterminate result in our findings.
Test Results Stratified by CD4 Counts
The median of CD4 count in patients with negative TST was 377 cells/mm3 and was 346 cells/mm3 for patients with positive TST. These values for patients with negative and positive QFT were 378 cells/mm3 and 361 cells/mm3, respectively. There was no statistically significant difference between CD4 count and test results.
Eight patients (6.2%) had a positive TST and CD4 count less than 200, and 4 (3.1%) patients had positive QFT and CD4 count less than 200. The TST and QFT test results according to CD4 count are shown in Table 1.
TST and QFT Test Results According to CD4 Count.
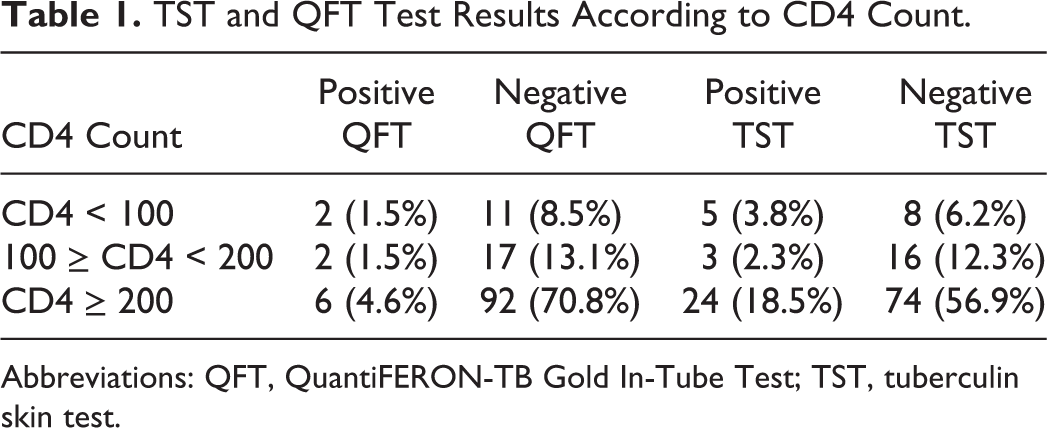
Abbreviations: QFT, QuantiFERON-TB Gold In-Tube Test; TST, tuberculin skin test.
Analytical Findings and Intertest Agreement
Forty-two (32.3%) patients had at least 1 positive test. We classified the patients into 2 groups according to concordant results of the tests (QFT+/TST+ or QFT−/TST−) and discordant results of the tests (QFT+/TST− or QFT−/TST+). Patient distribution by TST and QFT results is shown in Table 2.
Patient Distribution by TST and QFT Results.

Abbreviations: QFT, QuantiFERON-TB Gold In-Tube Test; TST, tuberculin skin test.
There was no statistically significant difference between TST or QFT positivity and evaluated variables except for history of imprisonment. These people had higher positive TST (P = .014) and QFT results (P = .01). No statistically significant association was found between TST induration size and QFT result (P = .251). The results of either TST or QFT were not associated with CD4 count (P > .2). Although there was 73.85% agreement between TST and QFT, their concordance was poor (κ = 0.083, 95% confidence interval = 0.256-1.332). Logistic regression analysis showed that history of IDU was associated with discordant results, suggesting there was more concordance between the 2 tests in patients with no history of IDU. Association of different variables with tests concordance and discordance is shown in Table 3.
Association of Different Variables With Tests Concordance and Discordance.

Abbreviations: TB, tuberculosis; BMI, body mass index.
Discussion
Early diagnosis of LTBI in HIV-infected patients would lead to reducing its morbidity, mortality, and dissemination in the community. Comparing TST and QFT in the screening of the patients for LTBI has been done in some studies. In such studies, QFT is considered as an alternative diagnostic tool for TST. Although some parameters have been shown to affect the results, studies evaluating these tests face a challenge, which is the lack of a “gold standard” for assessing their sensitivity and specificity, particularly in HIV-infected patients. 8,12
Positive TST results (24.6%) in our study were lower than similar reports of TB-high endemic settings (46.5%) and higher than TB-low endemic settings (7.7%). 19 Positive QFT in our study was 7.7%, which was lower than the reported value for a highly endemic TB setting (68%) and higher than the result (5.3%) of low endemic setting. 19 These findings are compatible with considering our community as a medium-TB burden country.
Indeterminate results are one of the disadvantages of QFT. 20 –22 Such results happen when the nil tube shows strong reaction or when reaction is weak in mitogen and TB antigen tubes. Some reasons for indeterminate results include inappropriate sampling and incubation, presensitization of T cells with an unknown antigen, and immune suppression. The frequency of indeterminate results is variable in different studies and ranges from <1% up to 38.3%. 20 -22 We had no indeterminate results in contrast to other studies, which is in favor of correctness of our procedure. 6,19 Another reason could be our patients’ CD4 counts. Low CD4 count or immunosuppressive status has been reported to be associated with indeterminate result of QFT. Some authors such as Talati et al, 23 Cho et al, 24 and Oni et al 25 have shown that HIV-infected persons with a CD4 ≤ 200 cells/mm3 are significantly more likely to have an indeterminate result.
We had some positive QFT results in patients with negative TST result that means applying QFT raised detecting LTBI by 4.6% in our study. This finding correlates with those of some similar studies and means that replacement of each test by the other may lead to false negative results, which will limit early management of the patients. 8,26 -29,30 Pai et al 31 showed that TST-positive cases are only a part of the cases with LTBI. They found IGRAs to be more sensitive than TST. Diel et al, 32 by reviewing studies on HIV-infected and non-HIV–infected patients, concluded that IGRA results are more strongly associated with progression to active TB than TST. The ability of IGRAs to predict progression of LTBI to active TB in HIV-infected patients was studied in some longitudinal studies. On the basis of these reports, patients with positive IGRAs have higher risk for active TB. 26 –29
Comparisons of QFT and TST in diagnosis of LTBI are studied by calculating the overall agreement between the 2 tests in terms of concordance. The concordances between them have been reported variously in different studies.
Two-test concordance was poor in our study, similar to the results of Hung in Taiwan, a country with an intermediate TB burden. 33 Fair concordance or moderate agreement between tests had been reported in some other studies. 14,19 Souza et al 34 represented an 81.8% relative raise in LTBI detection when QFT is added to TST. They showed that concordance between both tests was 96% in Brasilia, Brazil. Hoffmann and Ravn 19 had reported poor or moderate agreement for low-/middle-income regions in Europe. The agreement between TST and QFT was reported as good by in Egypt Abdel-Samea et al. 35 Khawcharoenporn et al 36 has reported low concordance between 2 tests. The level of agreement between tests has improved when using a TST cutoff ≥ 10 mm (κ = .39).
Kowada has recommended that in close contacts, IGRA would yield the greatest benefits at the lowest cost. And in immigrants and occasional screenings, TST followed by QFT would yield the greatest benefits at the lowest cost in low TB incidence countries. 37
Some factors such as study population, sample size, ethnic variations, different instruments used for the study, or many other unknown factors could lead to these differences in various studies. Some parameters such as economic issues have been shown as important determinants in final recommendations of such studies.
People with history of imprisonment in our study had statistically higher positive TST (P = .014) and QFT results (P = .01), which is compatible with the results of similar studies and expectable because of the close contact of the participants in such situation.
There was more discordance between the 2 tests in patients with history of IDU. This finding is compatible with some similar studies and might be because of their impaired cell-mediated immunity and more rapid CD4 count decline among these patients.38,39
It is not conclusively defined which diagnostic test is better to evaluate LTBI in HIV-infected patients, and decisions about this subject is influenced by some factors such as cost, accessibility, and patient convenience. 39 Considering imposed cost caused by dissemination of disease in the community and treatment of the patients would convince us that QFT performance and even chemoprophylaxis of false positive ones would be more cost-effective. So patients with initial positive TST do not need additional QFG to rule out false positive ones and should receive chemoprophylaxis and negative ones should be evaluated with QFT.
The QFT has become part of some national guidelines in the diagnosis of LTBI. Related guideline for immune-suppressed persons in United Kingdom recommends either TST or IGRAs, 17 and US guidelines also recommend TST or IGRAs but recommend the use of both if the first is negative and there is high clinical suspicion. 12 In Canadian guidelines for these patients, TST is recommended, followed by IGRA if TST is negative. 40 Present national guidelines in Iran recommend TST as screening test which would be advised to be changed as a dual testing approach in HIV-infected patients. This approach should be done especially for IDU patients.
As some other studies, the main limitation in our study was the lack of a gold standard for assessing 2 tests’ sensitivity and specificity. Other limitations were small sample size and impossibility of patient follow-up, which limited assessing diagnostic value of each test and better judgment on tests discordance.
Conclusion
A reasonable approach for LTBI screening in HIV-infected patients in medium-TB burden countries could be a dual testing approach. This approach starts with low cost TST, and the more expensive QFT is done for all negative TST. This approach should be done annually for all HIV-infected patients especially patients with history of IDU.
Footnotes
Acknowledgments
The authors are indebted to Ms Poursaleh and the personnel of HIV clinic of Tehran University of medical sciences and laboratory of Tehran organ transplant bank for cooperation in data collection and test performance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Tehran University of Medical Sciences grant.