
Abstract
Interferon gamma release assays (IGRAs) are poorly studied in HIV-infected children. The authors prospectively evaluated QuantiFERON-TB Gold results and family-described tuberculosis (TB) risk factors in 100 HIV-infected children in Botswana. Median age was 10.2 years; 58 were girls, 92 had received the Bacillus Calmette–Guérin (BCG) vaccine, 98 were receiving antiretroviral therapy, and the median body mass index was 15.8 kg/m2. Eighty-nine children had undetectable viral loads and the median CD4 count was 962 cells/mm3. Eighteen children had been treated for TB in the last 3 years. In the last 3 years, 36 (including 9 with TB) had contact with persons with TB (26 within/15 outside the home and 5 had >1 contact). In all, 96 children had negative IGRAs, 3 were indeterminate, and 1 was positive. The positive IGRA was reported in a child treated for TB prior to 3 years. Interferon γ release assay positivity was rare in this pediatric cohort living in an area with a high prevalence of TB.
Keywords
Introduction
Mycobacterium tuberculosis remains the most common opportunistic infection causing death in HIV-infected patients globally. 1 It is estimated that 13% of all cases with tuberculosis (TB) and 30% of all deaths from TB occur in persons living with HIV. 2 Resource constraints have precluded widespread implementation of preventive strategies for TB, such as screening and treatment of latent TB infection (LTBI). 3 Additionally, the best way to identify patients for prophylactic therapy is unclear. Both tuberculin skin tests (TSTs) and interferon gamma release assays (IGRAs) have demonstrated variable performance in HIV-infected patients. 4
Concern for IGRA conversions and reversions, indeterminate results in immunocompromised patients, and cost have limited the utilization of IGRAs in many high-burden settings. The World Health Organization has advised against IGRA use in low- to middle-income nations. 5 The goal of this investigation was to correlate the results of IGRAs with family-reported TB risk factors in a cohort of HIV-infected children in Botswana.
Materials and Methods
This was a prospective convenience sample of 100 HIV-infected children presenting to the Botswana-Baylor Children’s Clinical Centre of Excellence (COE) in Gaborone, Botswana. Botswana is a middle-income nation of 2 million persons, with an estimated HIV prevalence of 37% in adults and TB incidence rates of 455 per 100 000 persons. 6 Sixty-four percent of all cases of TB occur in HIV-infected persons. The COE cares for 2111 HIV-infected children. Children 1 month to 18 years old were eligible for inclusion if they were not receiving anti-TB therapy.
Questionnaires on TB risk factors, household density, and current symptoms were completed by caregivers with research assistant’s support. Electronic medical records were abstracted for anthropometrics, most recent viral load, CD4 count, antiretroviral therapy (ART), and TB treatment history. Blood for QuantiFERON-TB Gold (Qiagen, Maryland) was collected, incubated, and the plasma was extracted, and then the specimens were frozen in Botswana. Plasma was stored at −70°C for a maximum of 3 weeks, shipped to the laboratory of one of the investigators (E. A. G.), and processed according to the manufacturer’s instructions. 7 Tuberculin skin tests were not available in this clinic. Prior to the initiation of the study, approvals were obtained from the Botswana Ministry of Health, The Methodist Hospital Research Institute, and the Baylor College of Medicine and Affiliated Institutions institutional review boards. Consent to participate in the study was obtained from a parent or a legal guardian, and assent was obtained from children aged 7 years and older.
Frequencies were calculated for demographic variables and TB risk factors. Anthropometrics, viral loads, and cell counts were analyzed as continuous variables. Analyses were performed using Stata 11 (Stata, Inc, Texas).
Results
One hundred children were enrolled in the study. The demographic characteristics are listed in Table 1. No child was suspected of having TB at the time of enrollment based upon the symptoms. A total of 36 children reportedly had contact with at least 1 case having TB in the last 3 years: 26 in the home and 15 outside the home. This included 9 children who had been previously treated for TB. In the last 3 years, 18 children had a history of TB, that is, 17 pulmonary and 1 lymphadenopathy. In 10 cases, the diagnosis of TB was made in part by sputum smear microscopy and in 2 cases by radiographic findings; but in 6 cases, the TB records were unavailable for review.
Demographic Characteristics of Study Population.a
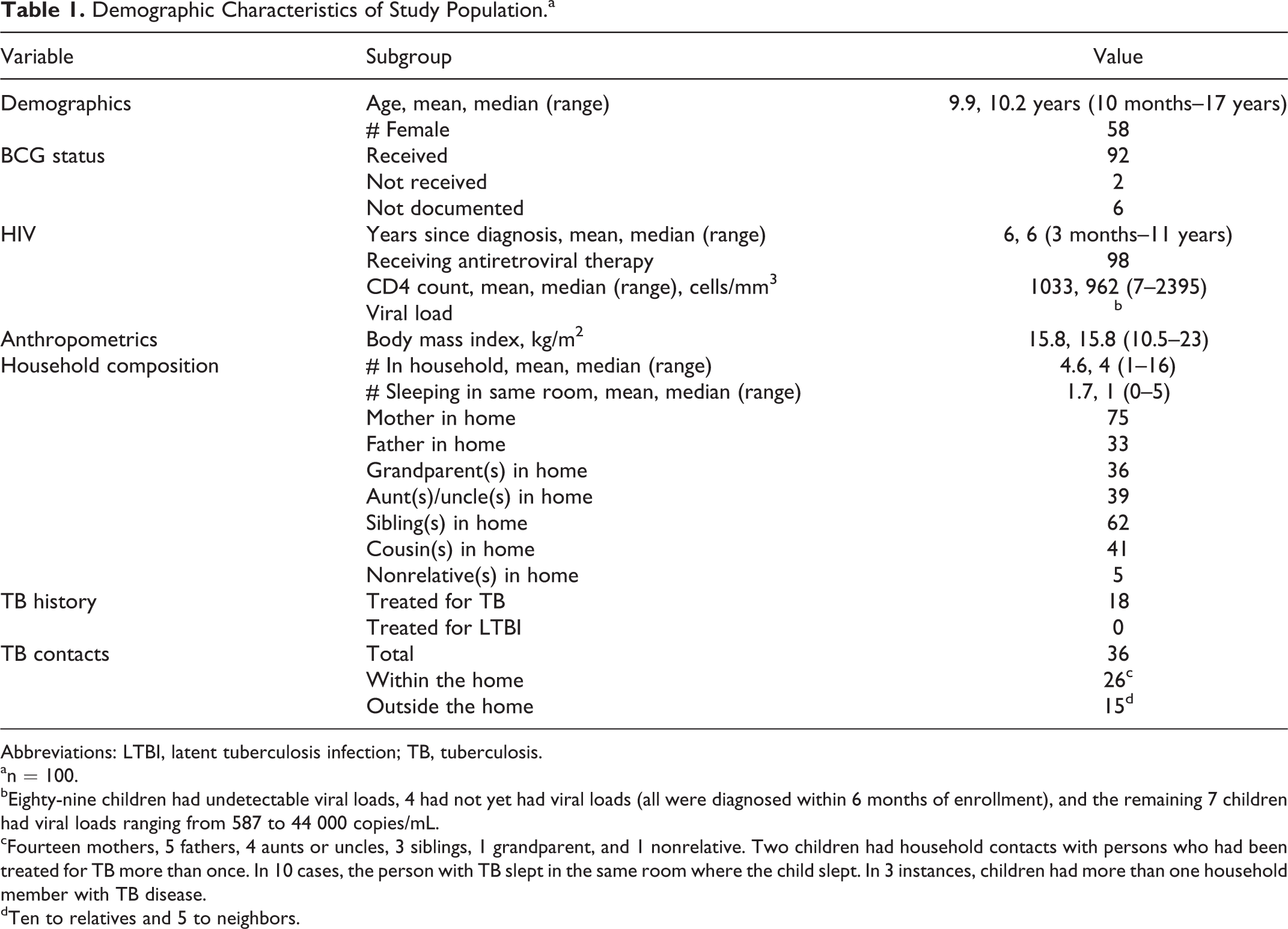
Abbreviations: LTBI, latent tuberculosis infection; TB, tuberculosis.
an = 100.
bEighty-nine children had undetectable viral loads, 4 had not yet had viral loads (all were diagnosed within 6 months of enrollment), and the remaining 7 children had viral loads ranging from 587 to 44 000 copies/mL.
cFourteen mothers, 5 fathers, 4 aunts or uncles, 3 siblings, 1 grandparent, and 1 nonrelative. Two children had household contacts with persons who had been treated for TB more than once. In 10 cases, the person with TB slept in the same room where the child slept. In 3 instances, children had more than one household member with TB disease.
dTen to relatives and 5 to neighbors.
Ninety-six children had negative IGRAs, 3 were indeterminate, and 1 was positive. The positive assay was reported in a 9-year-old boy treated for pulmonary TB (clinical case) prior to 3 years. He had no household or other contact with a known source case. Three children (aged 10 months, 2 years, and 9 years) had indeterminate results (all from failure of the positive control). One was recently diagnosed with HIV infection and had no viral load available (CD4 count: 739 cells/mm3), 1 had an undetectable viral load (CD4 count 1769 cells/mm3), and 1 had a HIV RNA-1 viral load of 25 000 copies/mL (CD4 count: 7 cells/mm3). None had any known TB contacts.
Discussion
In this population of children in a TB-endemic low- to middle-income country whose HIV is well controlled, IGRAs are infrequently indeterminate, and positives were rare. Prior studies have reported a wide range of indeterminate rates in immunocompromised hosts, which are as high as two-thirds in 1 study. 8 The low indeterminate rate may reflect that the vast majority of our cohort was on ART, thereby showing low viral loads and normal CD4 counts. A more intriguing finding was the low rate of IGRA positivity in this cohort, which occurred despite the rate of previous TB (18%) and high reported exposure history (36%). There are several possible explanations for this—IGRA positivity is not durable in HIV/TB-coinfected children, the children treated for TB did not have TB; IGRAs are insensitive in this population, particularly if children have high viral loads and low CD4 counts at the time of infection, or that shipping of the samples may have altered the results.
Data are available to support that IGRA positivity is not durable. One study of persons with positive IGRAs identified during a contact investigation showed that treatment with isoniazid and rifampin for LTBI resulted in reversions in IGRA positivity by 6 months in one-third of the patients, with a higher likelihood of reversion occurring in recent IGRA converters. 9 Similar findings have been observed in health care workers serially screened using IGRAs, where reversions were more common in younger health care workers. 10 Fluctuating IGRAs in immunocompetent health care workers have been hypothesized to be due to true reversions, repeated infections, or periodic secretion of TB antigens. 11 For children with TB, the negative IGRA obtained months to years after treatment may represent IGRA reversions. In 1 series of HIV-infected children with TB, treatment of TB reduced the magnitude of IGRA positivity, but both conversions and reversions were seen. 12 As none of our children was treated for LTBI, discordance between IGRA results and reported exposures was not due to treatment-associated reversions. However, exposures were reported by families because source case data were unavailable.
A second explanation for the low rate of IGRA positivity in children previously treated for TB is that the children never had TB. The diagnostic capabilities for children with suspected TB are limited. Smear microscopy was often the only available test. Given the high prevalence of TB in adults and the risk of morbidity and mortality of untreated TB in an immunocompromised child, the threshold for treating is understandably low. It is also possible that many of the adult contacts treated for TB did not have M tuberculosis. Microbiologic differentiation of TB and nontuberculous mycobacteria (NTM) is challenging in many settings, and the burden of NTM in persons living with HIV in sub-Saharan Africa is likely underestimated. One study of acid-fast bacilli smear-positive patients in Cameroon found that NTM and nonmycobacterial species comprised over 15% of culture-positive cases. 13 In 1 series of Ugandan infants and adolescents with suspected TB, 93% of all cultures grew NTM species. 14
A third explanation is that children infected with TB are insensitive to IGRAs, especially at a time when they were immunosuppressed. In our cohort the HIV infection was well controlled, but when they got infected with TB (if any) remains unknown and may have occurred before they received ART. Some studies have shown that HIV-infected adults coinfected with TB had lower interferon levels than that of HIV-negative adults with TB, and sensitivity increased with increasing CD4 counts. 15 Another possible explanation is homing, that is, when T cells migrate to the site of infection (eg, pulmonary) and leave the blood.16,17
Finally, it is possible that the process of shipping the specimens altered the results. We feel that this is unlikely, given that the test positive and negative controls worked consistently for the majority of children.
This study has several limitations. Concomitant use of TSTs was unavailable. This was a convenience sample relying on families reporting of TB contacts, which could not be verified against a national registry. Additionally, data on source case smear microscopy, timing and duration of exposure, and clinical course for contacts were unavailable. There were missing data on the treatment and diagnostic testing performed in children who had been treated for TB remotely, as this care was not coordinated through the COEs. These findings (especially the low rates of indeterminate tests) may not be generalizable to the settings where children have less ready access to antiretroviral drugs or to children whose HIV is less controlled.
In conclusion, we found that IGRA positivity and indeterminate assays in this cohort of children living with well-controlled HIV were rare, despite the frequency of previous TB and reported contacts with TB within and outside the home.
Footnotes
Acknowledgements
We thank Professor Gabriel Anabwani, Mrs Keofentse Mathuba, and Mr Kennedy Sichone for their assistance and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
ATC received a Baylor College of Medicine / Texas Children's Hospital Pediatric Pilot Grant for this project.