
Abstract
Background:
Assessment of longitudinal adherence patterns on virologic and immunologic responses to HAART in perinatally acquired HIV patients has not been studied.
Methods:
Perinatally infected pediatric HIV patients with adherence documented at least twice and corresponding viral load and T-cell (%) data measured during 2008-2009 were studied. Multiple adherence measures were utilized to identify patients with persistent adherence, nonadherence, or alteration of adherence. Virologic and immunologic outcomes were assessed.
Results:
Persistent adherence, nonadherence, and alteration of adherence to HAART were recorded in 41.9%, 8.1%, and 50.0% of 62 studied patients. Persistent adherence was associated with higher likelihood for persistent virologic suppression and lower risk for persistent virologic failure.
Conclusion:
Alteration of adherence to HAART is a significant predictor of persistent virologic failure and high viremia in perinatally infected HIV patients. Implementation of longitudinal adherence assessments may target patients with nonsustained adherence patterns and help decrease the risk for virologic failure and disease progression.
Introduction
High adherence to antiretroviral (ARV) treatment plays a significant role in the prevention of therapeutic failure in patients with HIV infection. 1,2 Imperfect adherence leads to altered ARV pharmacodynamics/pharmacokinetics and the development of drug resistance that furthers disease progression. 3 Although clinical management of children with perinatally acquired HIV infection requires additional considerations, inadequate treatment in growing children with HIV is associated with persistence of high levels of viral replication. 4 Studies have shown that nonadherence negatively impacts clinical and virologic outcomes in pediatric patients with HIV infection. 5 -7 However, approximately half of HIV-infected children and adolescents are not completely adherent to the ARV treatment regimens. 8 -10 In particular, perinatally infected patients challenged with initiation of treatment at an early stage of life have tremendous family-related social and psychological pressures and are at high risk of nonadherence to longitudinal courses of ARV therapy. The 2011 national guidelines for the use of ARV agents in pediatric infection recommend a measurement of adherence at each pediatric clinic visit in order to maintain and improve adherence to therapy in HIV-infected children and adolescents. 11 Because adherence to ARV therapy in HIV-infected children is a dynamic phenomenon, 12 the longitudinal assessment of adherence is superior to cross-sectional measurement in prediction of health outcomes. 13 A subset analysis of 35 adolescents with an initial undetectable viral load (VL) who were followed for more than 12 months in a Reaching Excellence in Adolescent Care and Health (REACH) project 14 showed a relationship between the lack of virological rebound and longitudinal self-reports of adherence to high activity antiretroviral therapy (HAART). Khan et al 15 identified complete adherence during 52 weeks as a significant predictor of reaching the lowest limit of VL (<400 copies/mL) in pediatric patients with HIV. However, there is still a gap in knowledge regarding the association between virologic and immunologic failure and adherence patterns during treatment of patients with perinatally acquired HIV infection. The present study is the first that was designed to identify a relationship between the types of adherence patterns to HAART and the risk of virologic and immunologic failure in pediatric patients with perinatally acquired HIV infection. We hypothesized that not only nonadherence but also nonsustained adherence to HAART increases the risk of persistent virologic and immunologic failure among pediatric patients with perinatally acquired HIV infection.
Methods
Perinatally infected HIV-positive children and adolescents on HAART, followed at the Robert Wood Johnson Medical School Pediatric AIDS Clinic in New Brunswick, New Jersey, during 2008 to 2009, with at least 2 consecutive adherence measurements and correspondingly tested VL (copies/mL) and CD4 count (%), were retrospectively included in this study.
This study was approved by the University's institutional review board. Informed consent was waived because of the retrospective data analysis study design.
Adherence was measured using a tool that was validated
10
and implemented in our clinic. The tool includes 3 measurements: self- or caregiver report, pharmacy refill report, and appointment maintenance data.
10
Self-report (if child
Predictor Variables
The longitudinal adherence patterns were classified as persistent adherence to HAART if the adherence scores of 3 or as persistent nonadherence if adherence scores of less than 3 were recorded consistently during the observation period. Variation in the adherence scores at different points during the observation was classified as alteration of adherence. For multiple regression analysis, the adherence pattern was identified as a dichotomous variable: persistent adherence versus persistent nonadherence/alteration of adherence.
Outcome Variables
Department of Health and Human Services (DHHS) guidelines 16 were used to categorize the virologic response during the follow-up. The patient was classified as having (1) persistent virologic suppression (if the VL was <48 copies/mL at each point of the adherence measurement), (2) persistent virologic failure (if the VL was >200 copies/mL at each point of the adherence measurement), (3) virologic rebound (if the VL was >200 copies/mL after being <48 copies/mL), and (4) virologic blip (if after the VL < 48 copies/mL, an isolated HIV RNA level that was detectable followed by a return to VL < 48 copies/mL). Serial VL results with persistent virologic failure (>200 copies/mL) were classified as persistent high (VL ≥ 1000 copies/mL) or persistent low (VL < 1000 copies/mL) viremia. For the purpose of multiple regression analysis, virologic response was identified as a dichotomous variable: persistent virologic suppression versus virologic alteration (includes patients with persistent virologic failure, virologic rebound, or virologic blip).
The revised Centers for Disease Control and Prevention (CDC) classification
17
was used to categorize the immunologic response during the follow-up as persistent nonsuppression if the CD4 count (%) was
Statistical Analysis
The descriptive comparison of virologic and immunologic outcomes was analyzed with respect to the adherence pattern (persistent adherence, persistent nonadherence, or alteration of adherence) using χ 2 test statistics or Fisher exact test, if needed, for the comparison of the categorical and analysis of variance for the continuous variables. Data are presented as proportion (%) and mean ± standard deviation (SD). Odds ratio (OR) and 95% confidence interval (95% CI) were calculated to identify the risk of virologic and immunologic outcomes in association with the adherence pattern. We carried out multiple regression analysis to identify (1) the effect of persistent adherence versus persistent nonadherence/alteration of adherence on virologic response (persistent virologic suppression versus virologic alteration) and (2) immunologic response (persistent nonsuppression versus immunologic alteration) after adjusting for age, number of observations, and duration of follow-up. The regression data are presented as β ± standard error of β (standard error). A 2-tailed P value of less than .05 was considered statistically significant. Statistical analysis was performed using STATISTICA software for Windows, Release 10.0 (StatSoft, Tulsa, Oklahoma).
Results
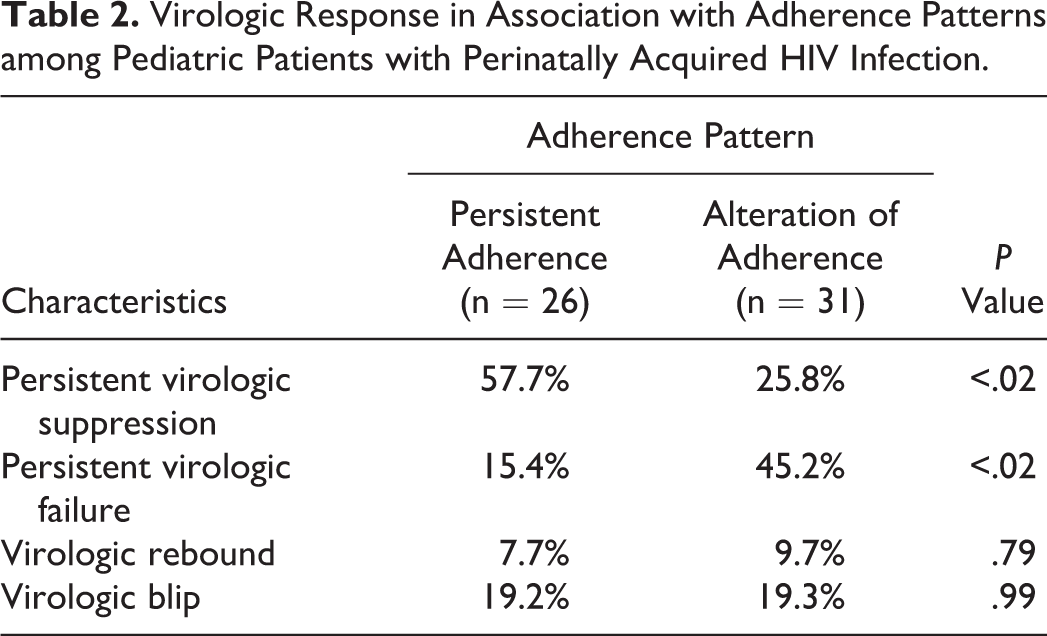
A total number of 62 children and adolescents with perinatally acquired HIV infection on HAART were enrolled retrospectively. Among these, 64.5% were female, 61.3% were African American, and their age ranged from 3 to 23 years with a mean age of 14.7 years (SD 4.3). A consecutive number of adherence assessments (2, 3, 4, and 5-6) had been recorded in 100%, 69.2%, 24.2%, and 8.1% of the patients, respectively, with an average of 3.0 (SD 0.9). The periods between measurements varied from 2 to 8 months with the average between the first and second, second and third, third and fourth, and fourth and fifth/six measurements being 3.9 ± 1.3 months, 3.5 ± 1.2 months, 3.4 ± 1.0 months, and 2.9 ± 0.5 months, respectively. The mean time of follow-up was 7.4 months (SD 2.8). Persistent adherence, persistent nonadherence, and alteration of adherence were seen in 41.9% (n = 26), 8.1% (n = 5), and 50% (n = 31) of the patients, respectively. Because of small numbers (n = 5), the patients from the persistent nonadherence group were not included in the descriptive comparison of adherence groups. As shown in Table 1, the differences in the demographic characteristics, duration of follow-up, and frequency of adherence assessments between patients with persistent adherence and alteration of adherence were statistically insignificant. A comparison of the virologic response (presented in Table 2) revealed lower prevalence of persistent virologic suppression and a higher rate of persistent virologic failure in patients with alteration of adherence than those who showed persistent adherence to HAART. Odds ratios of 3.9 (95% CI 1.28-12.0) and 0.22 (95% CI 0.06-0.79) were obtained retrospectively for the development of persistent virologic suppression and persistent virologic failure in patients with persistent adherence as compared to the group that included patients with alteration of adherence throughout the observation. Persistent high viremia (
Demographic Characteristics of Pediatric Patients with Perinatally Acquired HIV Infection Based on the Patterns of Adherence to ARV Treatment.

Abbreviation: ARV, antiretroviral.
Virologic Response in Association with Adherence Patterns among Pediatric Patients with Perinatally Acquired HIV Infection.
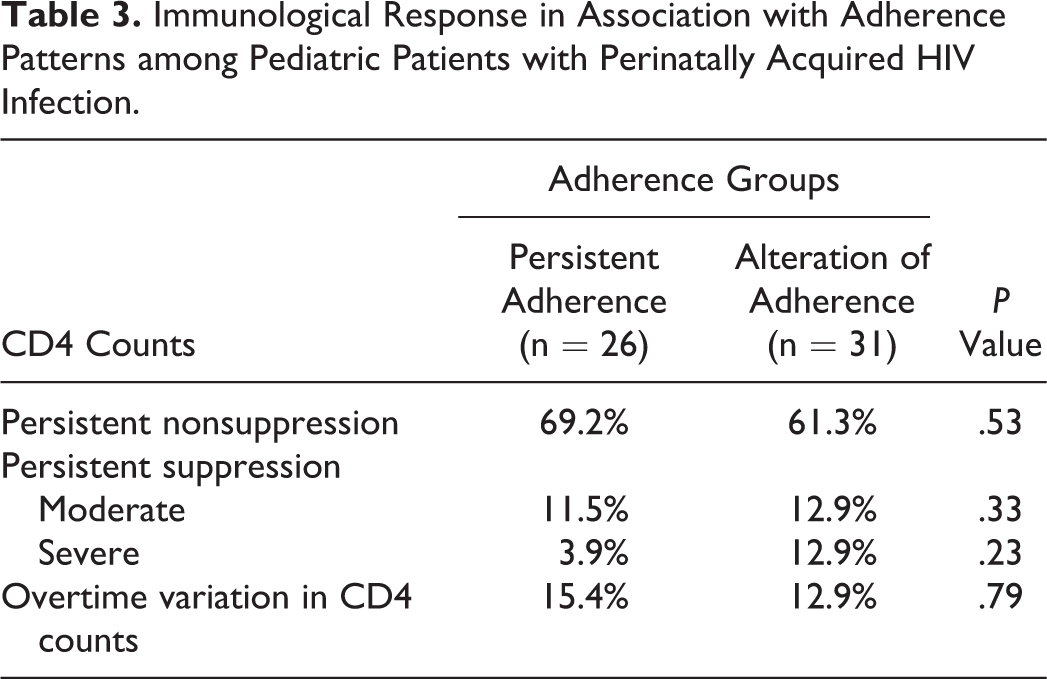
As shown in Table 3, the majority of patients, irrespective of the type of adherence pattern, showed persistent nonsuppression of CD4 counts. The 2 groups did not show any statistically significant difference in immunologic response. However, as compared to patients with persistent adherence, an insignificantly higher frequency of persistent severe suppression (CD4 count < 15%) was seen in those with an alteration of adherence over time.
Immunological Response in Association with Adherence Patterns among Pediatric Patients with Perinatally Acquired HIV Infection.
Overall, 9 (14.5%) of the 62 patients were recorded with persistent virologic and immunologic moderate/severe suppression, which accounted for 7.7% of the patients with persistent adherence, 16.1% with alteration in adherence, and 40% of patients with persistent nonadherence to ARV therapy. Multiple regression analysis showed significance for persistent adherence to ARV therapy in the achievement of persistent virologic suppression but not persistent immunologic nonsuppression after adjustment for age, duration, and number of observations (Table 4). For the patients included in the study, we found an indirect association of persistent immunologic nonsuppression with age (β = −0.275 ± 0.126, P < .04).
Factors That Impact the Odds for Persistent Virologic Suppression (VL < 48 copies/mL) or Persistent Immunologic Nonsuppression (CD4 ≥ 25%) in Pediatric Patients with Perinatally Acquired HIV Infection.

Abbreviations: VL, viral load; SE, standard error.
a After adjustment for age, duration, and number of observations.
b P < .04.
c P < .02.
Discussion
This study assessed therapeutic responses in pediatric patients with perinatally acquired HIV infection with respect to prospectively monitored adherence to HAART. In addition to the prospective approach, utilization of the previously validated, 10 multiple adherence measures, instead of a single measure, is a major strength of the present report. For the enrolled patients, we were able to characterize the longitudinal adherence patterns to ARV treatment as persistent adherence (41.9%), persistent nonadherence (8.1%), and alteration of adherence (50%). An approximate 4 times higher likelihood for sustenance of undetectable VL (<48 copies/mL) in association with persistent adherence was identified as compared to patients with alteration of adherence during HAART. Moreover, patients with nonsustained adherence throughout treatment were at a significantly higher risk of persistent virologic failure (VL > 200 copies/mL) and viremia (VL ≥ 1000 copies/mL) than those who were persistently adherent to HAART.
The existing evidence stresses the significance of nonadherence to ARV therapy as one of the major challenges in the management of HIV infection including children and adolescents with perinatally acquired HIV infection. 1,10,12,18 Several cross-sectional reports found that an undetectable VL was an important indicator of adherence to ARV therapy. 2,9,12 Bangsberg et al 19 showed that virologic control can vanish if there is a 10% decrease in adherence to ARV treatment regimens. Therefore, complete adherence to ARV treatment is considered a gold standard in the clinical care of HIV-infected patients. There are a few studies that showed a relationship between self-reported adherence and VL during prospective monitoring of adherence in pediatric patients with HIV. 15,20 Significantly lower VL was reported in pediatric patients with HIV infection who were adherent in the preceding month20 and during the 52 weeks of observation 15 as compared to those who were nonadherent. No assessment of immunologic response with respect to adherence was provided in these studies. We found that the immunologic response in the majority of patients was in the persistent nonsuppression category and was not associated with adherence patterns. Previously in our cross-sectional study, 21 we had also not found an association between the high level of virus production and severity of CD4 count depletion in children with HIV. Resino et al 22 showed that VL suppression is not necessary for recovery of CD4 counts. This discordant response in HIV-infected children is due to an opportunity for CD4 count recovery despite virological failure. 23 The renewal/replacement mechanisms for CD4 counts include both peripheral and thymic components, 24 and therefore it is possible that viral replication in children with perinatally acquired HIV infection is counterbalanced by high thymus activity that allows better replacement of CD4 counts as compared to adult patients with HIV. 4 Interactions between HIV replication and the immune system are specific in perinatally infected adolescents and young adults. 25 We found a significant association between persistent nonsuppression (CD4 ≥ 25%) and younger patient age (Table 4). Achievement of persistent nonsuppression is important for HIV-infected children due to the risk of immune-regulatory impairment associated with immunosuppression that leads to increased levels of autoantibodies and total immunoglobulin. 26
Several limitations of this study are a subject for discussion. The major limitation is the retrospective design based on the analysis of the data that were originally collected for clinical care. However, the standardized and timely concomitant assessment of adherence to ARV therapy and virologic/immunologic data that is implemented in the Pediatric AIDS Clinic minimizes the methodological limitation of the retrospective manner of data collection. In addition, very well documented demographics and follow-up records decreased the risk of collection of incomplete or missing information. Another limitation is the variation in the age of the participants and the number and duration of observations. However, the multiple regression analysis allowed control of these variables for the identification of the association between persistent adherence to HAART and persistent virologic suppression and persistent immunologic nonsuppression in the studied patients.
Conclusion
Alteration of adherence throughout HIV treatment with ARV regimens is a significant predictor of persistent virologic failure and high viremia in pediatric patients with perinatally acquired HIV infection. Since sustained virologic suppression requires maintaining persistent adherence to HAART, implementation of longitudinal assessments of adherence should be considered in the pediatric clinic setting to target patients with nonsustained adherence patterns in order to decrease the risk of virologic failure and disease progression.
Footnotes
Acknowledgments
We would like to acknowledge and thank our HIV care provider team and the administrative support staff for their efforts in patient care and meticulous data collection and entry. We would also like to thank our patients for allowing us to care for them and learn from them.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.