
Abstract
Objective:
Sustained adherence to highly active antiretroviral therapy is necessary to suppress viral replication and improve immunological and clinical outcomes. Although different studies tried to identify factors affecting adherence to highly active antiretroviral therapy, there are few studies after initiation of test and start strategy and the first-line drug regimen change in the study area. Therefore, this study aimed to determine the level of adherence to highly active antiretroviral therapy and associated factors among people living with HIV in Eastern Ethiopia.
Methods:
Institutional-based cross-sectional study design was conducted from 2 March 2020, to 30 March 2020. A total of 501 study participants were recruited using systematic random sampling. Data were collected using face-to-face interviews at the end of the clinic visit and a review of participants’ medical records. The level of adherence to highly active antiretroviral therapy was measured using the eight-item Morisky Medication Adherence Scale. The score ranges from 0 to 8, and a score of less than 8 indicates poor adherence. The data were entered into EpiData and exported to STATA for further analysis. The binary logistic regression analysis model was employed to identify associated factors. The association was reported with an adjusted odds ratio and a 95% confidence level. The significance level was declared at p = 0.05.
Results:
A total of 501 participants participated in the study, giving a response rate of 98.2%. The majority (314 or 62.7%) of study participants were females. The participants’ mean (standard deviation) age was 38.17 (8.75). The level of poor adherence to highly active antiretroviral therapy was found to be 33.73% (confidence interval: 29.70, 38.00). Age category 35 to 44 (1.65 (confidence interval: 1.02, 2.69)), no shortage of highly active antiretroviral therapy (0.46 (confidence interval: 0.28, 0.75)), substance use (1.67 (confidence interval: 1.11, 2.25)), having moderate depressive symptoms (4.00 (confidence interval: 1.94, 8.48)), and moderate anxiety symptoms (5.22 (confidence interval: 2.31, 8.84)) were significantly associated with the poor adherence to highly active antiretroviral therapy among adult people living with HIV.
Conclusion:
The level of poor adherence to highly active antiretroviral therapy was found to be high in this study. Poor adherence to highly active antiretroviral therapy was significantly associated with age, availability of highly active antiretroviral therapy drugs, substance usage, depressive symptoms, and anxiety symptoms. Improving the adherence levels requires stringent counseling, assuring continuous drug availability, and timely screening and management of depression and anxiety.
Introduction
Human immunodeficiency virus (HIV) is a global health issue that affects people of all ages and continues to pose a threat to social and economic development. 1 At the end of 2020, an estimated 37.7 million people worldwide were living with HIV/AIDS, with two-thirds of them being from the World Health Organization (WHO) 2 African Region. Ethiopia has a 0.9% national HIV/AIDS prevalence rate. 3 Ethiopia has made notable steps in controlling HIV/AIDS, but the prevalence remains comparatively high in urban areas. In the year 2020, approximately 11,000 adults aged 15 and above died as a result of AIDS-related illnesses. 4
Antiretroviral treatment began in 2003, and free highly active antiretroviral therapy (HAART) was launched in Ethiopia in 2005. The introduction of HAART reduces the burden of HIV meaningfully.5,6 Adherence to HAART is a primary cause of treatment success. At least 95% of the HAART adherence level is required to suppress viral replication.7,8 The optimal adherence level of HAART decreases the risk of developing ARV drug resistance, reduces the risk of transmitting HIV, reduces hospitalization, and lessens the need to switch from the first line to more expensive second and third-line treatments. 9 Adherence is defined as the extent to which a person’s behavior in taking prescribed medication, following a diet, and/or executing lifestyle changes corresponds with agreed recommendations from a healthcare provider. 10 Sustained high levels of adherence are, therefore, crucial to suppressing viral replication and improving people’s quality of life. 10 In contrast, poor adherence to HAART raises considerable difficulties for long-term follow-up. 11
The report from different studies conducted in Ethiopia revealed that the level of optimal adherence ranges from 72.4% to 94.3%, which indicates that HAART adherence is remaining suboptimal. 12 The roots of poor adherence to HAART are extremely varied, and adherence is associated with many individuals and facility-related factors. The findings of studies carried out in some developing countries like India, Nepal, Togo, and Nigeria identified that females, daily alcohol consumers, and people with depressive symptoms are less likely to adhere to HAART.10,11,13,14
Similarly, several studies in different corners of Ethiopia revealed that people with primary educational level, rural residents, lower monthly income, jobless, divorced people, and people with poor level of knowledge toward HAART were non-adherent, and two studies reported access to medication at any time and younger age (35–44 years) indicated associations with good adherence level to HAART.15–20 Previous studies also showed that proximity to the healthcare facility, the availability of HAART drugs, and the patients’ satisfaction with health service delivery were found to be significantly associated with HAART adherence.19,21–23 Despite the above reports, limited studies were conducted after the initiation of the “test and treat” strategy in August 2016 24 and the first-line HAART regimen change in the study area. Therefore, this study assessed the level of adherence to HAART among people living with HIV in Eastern Ethiopia.
Methods
Study design and setting
An institutional-based cross-sectional study design was employed among adult people on HAART at public health facilities in Harar from 2 March 2020 to 30 March 2020. Harar is located 522 km to the east of Ethiopia’s capital city. In Harar, two public hospitals, Hiwot Fana Specialized Comprehensive Hospital and Jugal General Hospital, offer comprehensive HIV/AIDS care and treatment. There were 4588 people on HAART in both hospitals.
Population and sample size
The source population for this study was adult people with HIV and on HAART at public health facilities in Harar, Eastern Ethiopia. The study has two objectives. The first objective was to determine the magnitude of poor levels of adherence to HAART, and the second objective was to identify factors associated with a poor level of adherence to HAART among adult people living with HIV in Eastern Ethiopia. Therefore, the sample size was determined for both the first and the second objectives. For the first objective, the sample size was calculated using a single population proportion with the following assumptions: 95% confidence level with a 5% margin of error and the poor adherence level (65%) from the previous study conducted in Dire-Dawa, Ethiopia. 25 Based on these assumptions, the calculated sample size for the first objective was found to be 350.
For the second objective, using a double proportion formula, which considers the following assumptions: 95% confidence level, with a 5% margin of error, power of 80%, ratio of 1:1, the percentage of outcome exposed (got family support) was 89% and the percentage of the outcome unexposed (had no family support) was 79%. Accordingly, the sample size for the second objective was 464, which is greater than the sample size calculated for the first objective. Therefore, the final sample size by adding a 10% non-response rate was 510.
All adults (⩾18 years old) living with HIV who had been in follow-up at a HAART clinic for at least a month and were available during the data collection period were eligible to participate. However, patients who were critically ill during the data collection period were not eligible to be included in the study. Critically ill patients may not be able to accurately respond to our questions. Moreover, issues related to autonomy and the validity of consent may not be ensured for critically ill patients.
Sampling procedures
Both public hospitals found in Harar were purposively selected based on the provision of comprehensive HIV/AIDS care and services. The calculated sample size was proportionally allocated to the two selected public hospitals: 325 and 185 from Hiwot Fana Specialized Comprehensive Hospital and Jugol General Hospital, respectively.
A systematic sampling technique was utilized to select study participants. The estimated client load during the study period in each hospital was divided by the total sample size allocated to the respective hospitals to obtain the fixed periodic interval (kth value). Then, participants were selected using every kth value. The first study participant was selected by the lottery method.
Variables of the study
The dependent variable was a poor level of adherence to HAART. The predictor variables were as follows: socio-demographic characteristics (age, sex, marital status, educational status, and occupation), psychosocial (depression, anxiety, substance use, and knowledge of HAART), and health service-related (medication availability).
The level of adherence to HAART was measured using a widely utilized self-reported eight-item Morisky Medication Adherence Scale (MMAS-8). Scores obtained are summed up to give a total scale score, which ranges from 0 to 8, with a score of 8 reflecting high adherence, 6 to 7 as moderate adherence, and less than 6 reflecting low adherence, 26 but, unlike other chronic diseases, people receiving HAART should have a high level of adherence (>95%) to suppress viral load and increase CD4 count. 27 Therefore, respondents who scored less than 8 out of eight questions in MMAS-8 were considered poor adherents. Knowledge of patients toward HAART was assessed using six items adapted from similar literature, 17 and those who scored above the mean were considered to have good knowledge. Depression was assessed using the Patient Health Questionnaire (PHQ) with nine items. The PHQ-9 is the depression module, which scores each of the 9 DSM-IV criteria as “0” (not at all) to “3” (nearly every day). The scores represent 0–4 as none/minimal, 5–9 as mild, 10–14 as moderate, 15–19 as moderately severe, and 20–27 as severe depression. Anxiety was also assessed using the Generalized Anxiety Disorder Assessment (GAD-7) with seven items. The GAD-7 score is calculated by assigning scores of “0” (not at all) to “3” (nearly every day). The scores represent 0–4 as none/minimal, 5–9 as mild, 10–14 as moderate, and >15 as severe anxiety.28,29
The level of social support was measured using Oslo social support scale (OSSS-3). OSSS-3 consists of three items with a total score ranging from 3 to 14. The scores represent 3–8 as poor social support, 9–11 as moderate social support, and 12–14 as strong social support. 30 Moreover, whether study participants used substances (drinking alcohol, smoking cigarettes, and chewing khat) were assessed by yes or no questions. Finally, health service-related variables were assessed using different variables such as counseling and availability of medications in ART clinics by using yes-or-no questions.
Ethics approval and consent to participate
The ethical review committee of the College of Medicine and Health Sciences of Haramaya University approved the study protocol. Besides, a support letter was obtained from the medical directors of both hospitals to interview the respondents and review medical records. Written and signed informed consent was obtained from all respondents enrolled in the study. Confidentiality during all phases of research activities was kept, and data were held on a secured password-protected system.
Data collection procedures and quality control
Structured questionnaire was used by translating into two local languages (Amharic and Afan Oromo languages). The questionnaire was pre-tested on 10% of the study population from outside the study area. Data were collected through face-to-face interviews using self-reported questionnaires at the end of an ART clinic visit. In addition, the medical records of respondents were reviewed to identify clinical markers like CD4 count and WHO clinical staging. Following a 2-day training, data were collected by nurses with BSc degrees. The principal investigator supervised the data collectors closely. Besides, daily monitoring of data for completeness and consistency was conducted.
Statistical analysis
Data entries were conducted by using EpiData 3.1 version and exported to STATA 14 for further analysis. Descriptive statistics and summary statistics were presented using text and tables. The association of socio-demographic factors, clinical-related factors, depression, anxiety, and knowledge of HAART with poor adherence was conducted by using binary logistic regression. Variables to be included in the binary logistic regression model were checked for their important assumptions. Important assumptions that should be fulfilled for binary logistic regression comprise independence of errors, linearity in the logit for continuous variables, absence of multicollinearity, and lack of strongly influential outliers. Moreover, there should be an adequate number of events per independent variable. 31 Primary, bivariate logistic regression model was fitted, and variables with a p-value of ⩽ 0.25 were retained for the final multivariable logistic regression analysis. The variables with a p value of less than 0.05 in the multivariable logistic regression analysis were declared statistically significant.
Results
Socio-demographic characteristics
A total of 501 participants took part in the study, giving a response rate of 98.2%. The majority (314, or 62.7%) of study participants were females. The participants’ mean (SD) age was 38.17 (± 8.75). More than one-third, 194 (38.7%) were married (Table 1).
Socio-demographic characteristics of adult people living with HIV in Harar, Eastern Ethiopia, 2020 (n = 501).
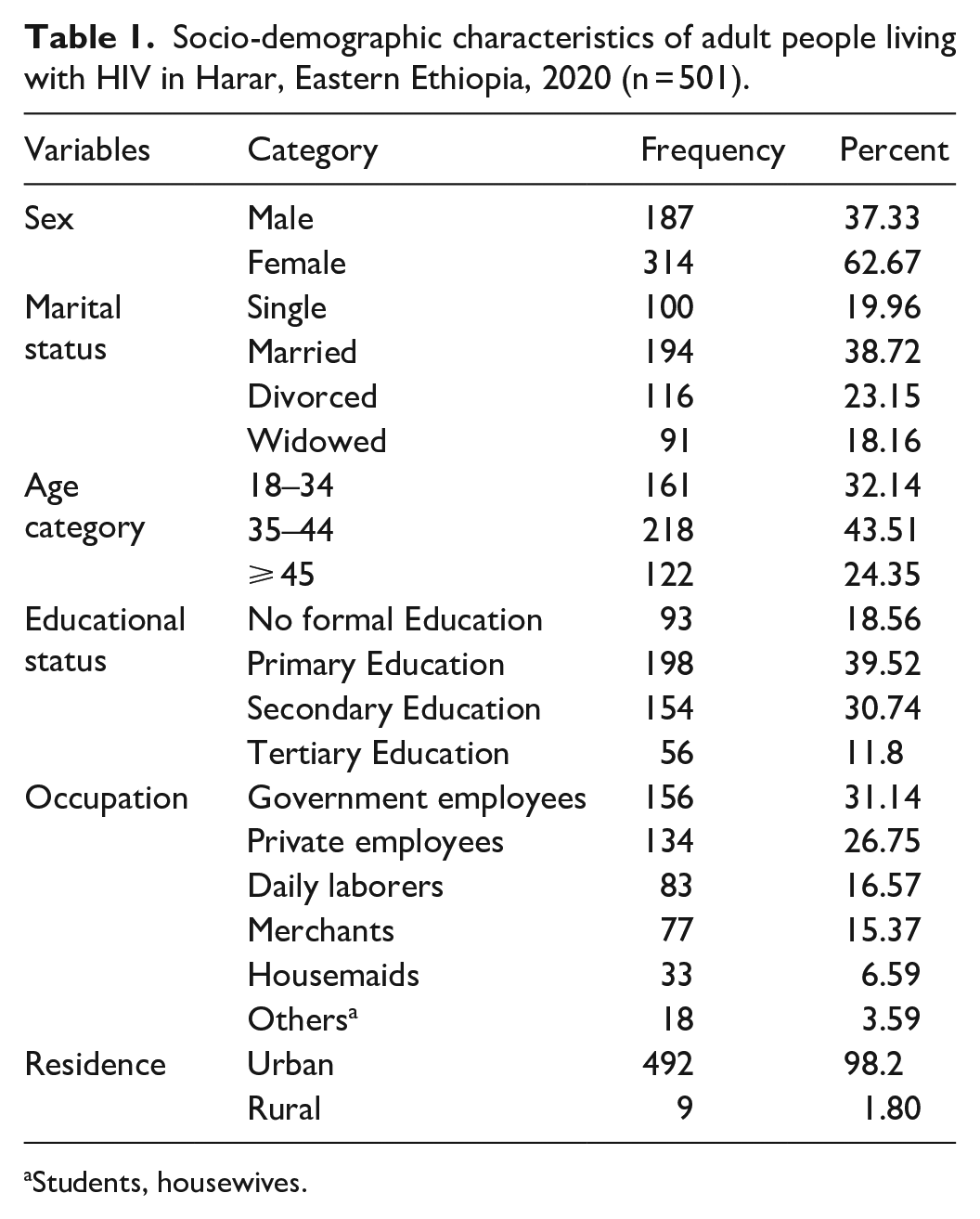
Students, housewives.
Clinical related and other characteristics
The majority of respondents, 435 (82.5%), were on HAART for ⩾ 24.1 months’ duration. More than three-fourths (382, or 76.2%) had a CD4 count of ⩾ 500 cells/mm3. The majority, 351 (70.1%), were taking FDC of TDF + 3TC + DTG. More than one-third of participants, 186 (37.1%) took additional drugs other than HAART. The most commonly used additional drugs were pain killers, which accounted for 57 (11.4%), followed by cotrimoxazole with 46 (9.2%). One hundred fifty-five (30.9%) participants reported different side effects. Around 474 (94.0%) of study participants have good knowledge of ART medication. Among 501 enrolled in the study, 219 (43.8%) of them were using substances. The most commonly used substance was khat, at 146 (66.7%), followed by alcohol at 50 (22.8%). In addition, 430 (85.82%) of the study participants had mild depression, and 439 (87.62%) of them had mild anxiety (Table 2).
Clinical-related and other characteristics of adult people living with HIV in Harar, Eastern Ethiopia, 2020 (n = 501).

Level of adherence to HAART among people living with HIV
Of the 501 study participants, 33.73% (95% CI: 29.70, 38.00) were found to be poor HAART adherents, while 66.26% (95% CI: 61.99, 70.02) were found to be good HAART adherents.
Factors associated with poor adherence to HAART among PLHIV
Multivariable logistic regression analysis showed that participants’ age, shortage of highly active antiretroviral drugs, substance use, depressive symptoms, and anxiety symptoms were significantly associated with poor adherence. The study showed that the odds of being a poor adherent to HAART were 1.65 (AOR = 1.65 (CI: 1.02, 2.69)) times more likely among the 35–44 age group when compared to the 18–34 age group study participants. Individuals from health facilities where HAART drugs were available were 54% (AOR = 0.46 (CI: 0.28, 0.75)) less likely to have poor adherence than individuals from health facilities where HAART drugs were unavailable. The odds of poor adherence were 4.00 (AOR = 4.00 (CI: 1.94, 8.48)) times more likely among patients with moderate depressive symptoms compared to those with none/minimal and mild depressive symptoms. Moreover, among the risky behaviors, this study revealed that the odds of poor adherence were 1.67 (AOR = 1.67 (CI: 1.11, 2.25)) times more likely among patients with substance users when compared to their counterparts. Finally, it was observed that the likelihood of poor adherence was 5.23 (AOR = 5.22 (CI: 2.31, 8.84)) times more likely among patients with moderate anxiety symptoms when compared with patients with none/minimal and mild anxiety symptoms (Table 3).
Factors associated with poor adherence to HAART among PLHIV in Harar, Eastern Ethiopia, 2020 (n = 501).

Significant at p value ⩽ 0.05.
Discussion
The purpose of this study was to determine poor adherence to HAART and associated factors among adult people on HAART in Harar, Eastern Ethiopia, at selected public health facilities. Poor adherence to HAART was found to be high. The findings revealed that participants’ age, availability of HAART drug, substance use, and having depressive and anxiety symptoms were all significantly associated with poor HAART adherence.
In this study, 33.73% of participants were poor adherent to HAART (CI: 29.70, 38.00). The finding was in line with the study conducted in Southwest Ethiopia 34%. 32 However, the finding was higher than the study conducted in Nigeria 20%; 33 Hara Town, Ethiopia 15%; 34 Hosanna Town, Ethiopia 9.3%; 18 and Debre-Birhan, Ethiopia 12.8%. 35 This discrepancy may be due to the difference in the medication adherence measurements scale (use of MMAS-8 in our findings).
Some of the factors identified in this study are consistent with the literature from both developed and developing countries. Participants in this study who were 35–44 years old were more likely to be non-adherent than those who were 18–34 years old. This finding is inconsistent with the finding of a study conducted in Brazil and Tanzania, which shows younger people were more likely to be non-adherent.36,37 In addition, studies conducted in different parts of Africa reported that younger age has been associated with poor adherence.38–40 The association between older age and poor adherence toward HAART was not reported elsewhere. The difference in age category could be a potential explanation for these inconsistent results. In this study, age was categorized as 18–34, 35–44, and 45 or higher.
Participants in this study who reported a shortage of HAART drugs in the ART clinic were more likely to be poor adherent than those who reported no shortage. This finding was supported by the study conducted in Jima zone health facilities. This might be because easy accessibility of services including medication will improve utilization. 19 People with easy access to HAART and other important medications may adhere to prescribed medication compared with those who lack access. Substance users were also shown to be more likely to have poor adherence in this study. This finding was coherent with a cross-sectional study conducted in Togo and Wolaita Sodo.41,42 This might be because alcohol intake increases forgetfulness to take HAART on time and based on the instructions and can lead to poor drug adherence. The most commonly used substance by study participant in this study was khat and alcohol.
Moreover, this study also showed that moderate depressive symptoms were expected to increase the odds of being poor adherent. This finding was also supported by the study conducted in Sub-Saharan Africa, 43 Chile, 44 and the United States. 45 This might be due to mental comorbidity may result in forgetfulness, poor organization, and poor comprehensive treatment plan, and can lead to poor medication adherence.15,46 Furthermore, HIV and depression comorbidity have been shown to impair self-care and medication adherence. Finally, this study found that participants with moderate anxiety were more likely to have poor adherence than those with mild anxiety. Various studies found that anxiety has a significant association with poor and imperfect adherence.47,48 People with anxiety may lack interest in lifelong HIV treatment and find it hard to adhere to HAART for a long period of time.
This study had several limitations. Primarily, since this study was a cross-sectional study, it will not show a causal relationship between the study’s dependent and independent variables. The study also investigated findings at a single point in time; therefore, factors affecting the adherence level outside of the study period could not be investigated. Finally, the questionnaire was prone to social desirability bias, because everyone does not want to expose their inability or unwanted attitude.
Conclusion
The magnitude of poor adherence to HAART was high. Age of participants, shortage of the drugs, substance use, depression, and anxiety were significantly associated with the poor level of adherence to HAART. Continuous counseling services on the importance of adherence, making medications available, and considering early screening and management of depression, as well as anxiety, are highly recommended. Thus, addressing significant predictors and strengthening continuous follow-ups are suggested to improve medication adherence.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221104429 – Supplemental material for Poor adherence to highly active antiretroviral therapy and associated factors among people living with HIV in Eastern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221104429 for Poor adherence to highly active antiretroviral therapy and associated factors among people living with HIV in Eastern Ethiopia by Degu Tegegne, Galana Mamo, Belay Negash, Sisay Habte, Tesfaye Gobena and Shiferaw Letta in SAGE Open Medicine
Footnotes
Acknowledgements
First, we would like to forward our kindest regards to our study participants. We extend our thanks to data collectors and supervisors who are the backbone to finalize the report. In conclusion, the authors would forward great thanks to Haramaya University for minimal financial support.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting the article, reviewing; gave approval of the final version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from Haramaya University College of Health and Medical Sciences Institutional Health Research Ethics Review Committee (IHRERC). The ethical approval letter number was IHRERC/167/2020.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed voluntary consent was obtained from all study participants before the commencement of data collection.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.