
Abstract
Introduction
Since the introduction of highly active antiretroviral therapy (HAART), persons living with HIV/AIDS have seen a substantial reduction in morbidity and mortality associated with their illness. 1,2 The life expectancy of HIV-positive individuals on therapy now approaches that of uninfected individuals. 3 However, very high levels of adherence to HAART are required to derive a sustained long-term clinical benefit. This can be challenging due to potential tolerability and emergent drug toxicity issues. Optimal adherence has been reported as a precondition to achieve sustained virologic suppression and immune reconstitution and is associated with decreased morbidity and mortality. 4 –10 Optimal adherence can be defined as ≥95%, though recent evidence suggests virologic suppression can be achieved with more moderate levels of adherence. 5,11 Suboptimal adherence may lead to the development of drug resistance, which may increase mortality, limit treatment options, and lead to transmission of drug-resistant strains, a significant public health concern. 12 –14 Understanding the predictors of adherence to HAART is essential to design and target programs to optimize HAART outcomes.
Adherence is a dynamic process and depends on a variety of sociodemographic, clinical, and environmental factors. Some factors consistently shown to be associated with suboptimal adherence include depression, drug and alcohol abuse, and a lack of social support. 6,15 –21 Clinical factors including regimen complexity, disease severity, experience of side effects, and baseline CD4 count and viral load also play an important role in determining adherence to HAART. 6,22 A number of physician-mediated factors have been associated with adherence including overall quality of the physician–patient relationship and physician experience in HIV care. 23,24 Recently, there has been increased emphasis on the role of the broader determinants of health in adherence, including the role of housing and overall quality of life. 25,26 Among people who inject drugs these factors are often compounded, leading to poorer levels of adherence. In addition, people who inject drugs are also more likely to initiate HAART at a more advanced stage of disease and are more likely to die of HIV-related illness largely due to inequitable access to HAART. 27 –32
This study will determine the factors associated with antiretroviral adherence in a cohort of HIV-positive individuals on HAART in British Columbia (BC), Canada. In the current context of rapidly expanding access to HAART in this and other settings, an understanding of the barriers and facilitators of optimal adherence is essential.
Methods
Participants and Recruitment
The Drug Treatment Program (DTP) at the British Columbia Centre for Excellence in HIV/AIDS (BC-CfE) is mandated by the BC provincial government to distribute antiretroviral medications, free of charge, to all eligible persons living with HIV/AIDS requiring treatment in the province. The DTP distributes medications according to the guidelines set by the Therapeutic Guideline Committee, which are regularly updated and have remained consistent with those from the International AIDS Society–USA since 1996. 33 Details regarding the distribution of antiretroviral medications through the DTP have been previously described in detail. 34
Individuals enrolled in the DTP were eligible to take part in the Longitudinal Investigations into Supportive and Ancillary health services (LISA) study. To be eligible for LISA, participants had to be at least 19 years of age, be antiretroviral therapy (ART) naive, and have initiated ART after 1996 and prior to their interview. Participants were recruited through letters distributed by their physicians and pharmacists, advertisements at HIV/AIDS service organizations in BC, and through word of mouth. The LISA study is closely representative of the number of people on treatment by health authority in the province, although particular subpopulations were deliberately oversampled in order to sufficiently power subanalyses. Consequently, women, people who inject drugs and people who identify as Aboriginal are overrepresented in the LISA cohort.
A comprehensive interviewer-administered survey was conducted to collect data on sociodemographic information, service utilization, quality of life, and drug and alcohol use, among other important covariates. Clinical variables, including the year of HIV diagnosis and year of HAART initiation, were obtained through linkages with the DTP. The recruitment period for this study was July 2007 to January 2010. Interviews were carried out by trained interviewers and took approximately 60 minutes to complete. A $20 honorarium was offered to all participants as compensation for their time. Ethical approval for the LISA study was obtained from the University of British Columbia/Providence Health Care, Vancouver Coastal Health, University of Victoria, and Simon Fraser University Research Ethics Boards. The LISA study is supported by the Canadian Institutes of Health Research (CIHR).
Outcome and Explanatory Variables
The main outcome variable in this analysis was adherence to HAART. As previously mentioned, we estimated adherence based on refill compliance, calculated as the number of days of antiretroviral medications dispensed, divided by the number of days of follow-up during the 12 months prior to interview date, and expressed as a percentage. 35 Individuals with suboptimal adherence are those who received HAART for less than 95% of the time in the 12 months preceding the interview date. The prescription refill method of measuring adherence has been independently associated with clinical and biological end points in previous studies. 4,9
Explanatory variables of interest included housing, drug and alcohol use, HIV-related stigma, and depressive symptoms. Housing stability was assessed based on the participant’s reported place of residence. Unstable housing was defined as living in a single room occupancy hotel, shelter, hostel, treatment center, prison, or having no fixed address at the time of interview. Stable housing was defined as living in an apartment or house.
For drug and alcohol use behavior, current use was defined as self-reported use in the 3 months preceding the interview. In this analysis, injection drugs included injection of cocaine, crack, heroin, speedball (heroin and cocaine), methamphetamine, or anabolic steroids. Illicit drugs included ecstasy, hallucinogens, γ-hydroxyl butyrate (GHB), sniffing, and ketamine in addition to the injection drugs. Problematic drinking was defined using the CAGE questionnaire which consists of 4 questions regarding alcohol use including
Stigma was measured using a validated short form of the HIV Stigma scale. This scale covers a variety of areas including personalized stigma, disclosure concerns, negative self-image, and concern with public attitudes toward people with HIV. 37 Depressive symptoms were measured with the 10-item Center for Epidemiological Studies depression (CES-D 10) scale, with participants scoring 10 or higher being classified as having depressive symptoms. 38
Other variables of interest were daily pickup of HIV medications, self-reported satisfaction with primary care physician, use of medication memory aids (special containers or alarms), and methadone maintenance therapy in the 6 months preceding the interview date. Sociodemographic variables included age, gender, ethnicity, level of education, annual income, and history of incarceration.
Clinical variables obtained through linkages with the DTP included year of HIV diagnosis, year of HAART initiation, use of once-daily treatment regimen, and having a primary care physician with experience in HIV care. An experienced physician was defined as a physician who has 6 or more HIV-positive patients on ART in his or her practice. The maximally assisted therapy (MAT) variable was applied to participants whose pharmacy pickup site in the DTP database was listed as MAT in the 12 months prior to the interview date. This variable indicates enrollment with the MAT program within the year but does not specify the frequency or type of resources (counselor, nutritionist, case manager) each participant accessed.
Statistical Analysis
Patients were categorized into adherent and nonadherent groups using the 95% prescription refill compliance as the cutoff point. In bivariate analysis, the chi-square test was used on categorical variables and the Wilcoxon rank sum test on continuous variables to examine the relationship between adherence and each explanatory variable independently and to identify all potential factors associated with adherence. Variables with a significant P value (<.05) in bivariate analysis were considered potential factors associated with adherence and were entered into a multivariable logistic regression model. An Akaike Information Criterion (AIC)-based model selection approach was used to help select the combination of variables that best predicted the probability of being adherent. The Hosmer-Lemeshow test was used to examine the goodness-of-fit. All analyses were conducted using SAS version 9.1.3 (SAS, Cary, North Carolina).
Results
Between July 2007 and January 2010, interviews were conducted with 1000 participants in BC. Inclusion criteria for this study were 19 years of age, HAART naive before 1996, and for whom adherence estimates were available for the 12 months prior to the interview. Given these criteria, 566 participants (56.6%) were included in this analysis.
Table 1 describes the general characteristics of LISA participants who met the inclusion criteria. Among LISA participants, the median age at HAART initiation was 40 (interquartile range [IQR]: 33-46), 415 (73.3%) were male, 174 (30.7%) self-identified as having Aboriginal ancestry, and 338 (59.7%) completed high school education. Less than half (40.3%) had an annual income >$15 000, 389 (68.7%) reported stable housing, 287 (50.7%) had ever been incarcerated, and 344 (60.8%) reported a history of injection drug use. In the year prior to the LISA interview date, 316 (55.8%) participants were optimally adherent to HAART.
Characteristics of LISA Participants Meeting Inclusion Criteria (n = 566)

Abbreviations: LISA, Longitudinal Investigations into Supportive and Ancillary health services study; HAART, highly active antiretroviral therapy; IQR, interquartile range.
aInclusive of past and current injection drug use.
As shown in Table 2, LISA participants with optimal adherence were more likely to be older (median IQR 48 vs 43, P ≤.001), male (83.2% vs 60.9%, P ≤.001), self-report non-Aboriginal ancestry (77.0% vs 59.2%, P ≤.001), have completed high school education (69.3% vs 47.6%, P ≤.001), have an annual income >$15 000 (49.8% vs 28.2%, P ≤.001), be stably housed (74.7% vs 61.2%, P ≤.001), and to never have been incarcerated (58.2% vs 38.0%, P ≤.001). Optimally adherent participants were less likely to experience depressive symptoms (48.6% vs 37.6%, P = .009), to currently use illicit drugs (46.2% vs 62.4%, P ≤.001), and to report current or past injection drug use (17.4% vs 31.2% and 32.0% vs. 44.0%, respectively; P ≤.001). No significant difference was observed with respect to stigma or problematic alcohol use. Also in Table 2, clinical indicators associated with optimal adherence included not accessing methadone treatment (79.1% vs 64.8%, P ≤.001) and not using once-daily treatment regimens (30.1% vs 20.3%, P = .010). No difference was observed with respect to the year of HIV diagnosis or year of HAART initiation. Optimally adherent individuals were also more likely to use memory aids for medication (42.1% vs 31.0%, P = .007) and to be enrolled in the MAT program (12.0% vs 5.6%, P = 0.009). Physician-mediated factors such as satisfaction with physician and having a physician experienced in HIV care were not statistically significant in this cohort.
Characteristics of Participants by Adherence Level in the Year Prior to the LISA Interview (n = 566)

Abbreviations: HAART, highly active antiretroviral therapy; IQR, interquartile range; MAT, maximally assisted therapy.
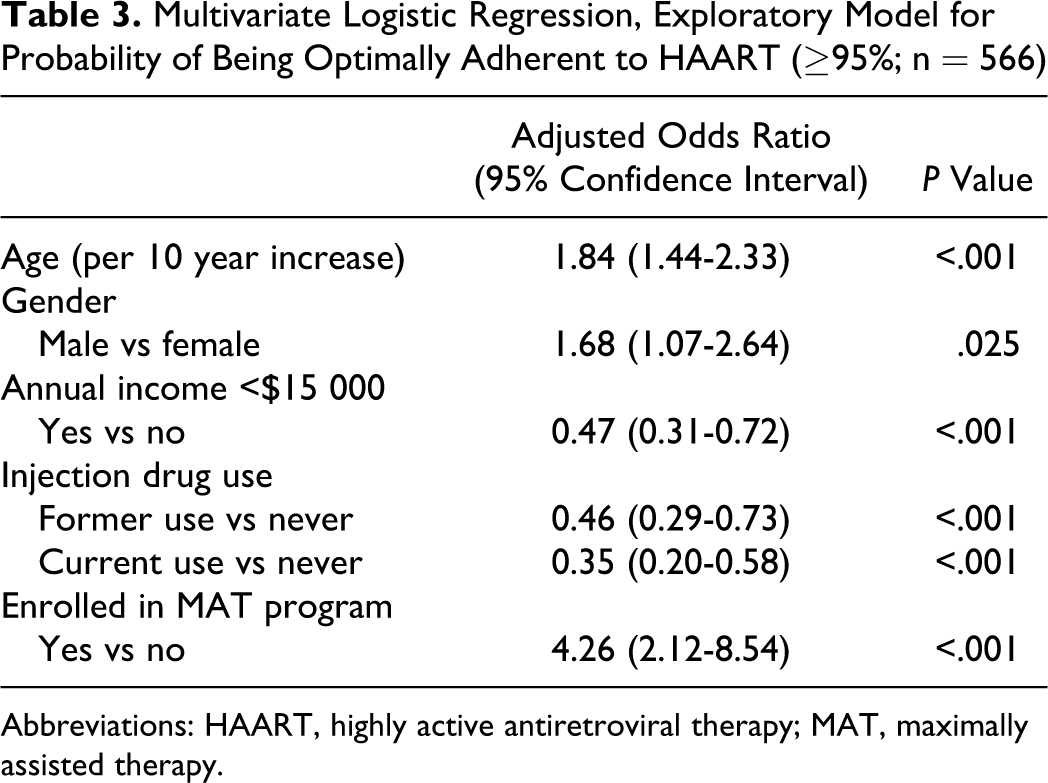
Multivariable logistic regression analysis was used to determine factors independently associated with optimal adherence. Table 3 shows that >95% adherence was independently associated with increasing age (adjusted odds ratio [AOR] = 1.84, 95% confidence interval [CI]: 1.44-2.33), being male (AOR = 1.68, 95% CI: 1.07-2.64), and being enrolled in the MAT program (AOR = 4.26, 95% CI: 2.12-8.54). Barriers to optimal adherence, identified in this analysis, included having an annual income <$15 000 (AOR = 0.47, 95% CI: 0.31-0.72) and past or current injection drug use (AOR = 0.46, 95% CI: 0.29-0.73 and AOR = 0.35, 95% CI: 0.20-0.58, respectively).
Multivariate Logistic Regression, Exploratory Model for Probability of Being Optimally Adherent to HAART (≥95%; n = 566)
Abbreviations: HAART, highly active antiretroviral therapy; MAT, maximally assisted therapy.
We conducted a sub-analysis of 344 individuals who reported a history of injection drug use. In this subset, less than half (45.3%) of the participants were >95% adherent to HAART. Bivariate analysis showed those with optimal adherence were more likely to be older (median IQR 47 vs 43, P ≤ .001), male (76.3% vs 56.9%, P ≤ .001), not report Aboriginal ancestry (69.2% vs 58.0% P = .031), and to have completed high school education (52.6% vs 41.0%, P = .032) compared to those with suboptimal adherence. There was no statistically significant difference in adherence between active injection drug use and former injection drug use. Among persons with a history of injection drug use, being enrolled in the MAT program (21.8% vs 6.9%, P ≤ .001) was more common among optimally adherent individuals. In multivariable analysis, ≥95% adherence among persons with a history of injection drug use was independently associated with increasing age (AOR = 1.74, 95% CI: 1.28-2.38), being male (AOR = 1.95, 95% CI: 1.17-3.27), and being enrolled in the MAT program (AOR = 4.02, 95% CI: 1.98-8.16; data not shown).
Discussion
Our results demonstrate that within a cohort of HIV-positive individuals on HAART in BC, only 55.8% of participants achieved ≥95% adherence, as measured by prescription refill compliance. This rate of adherence is consistent with previous studies utilizing this method of measurement. 9 Age, gender, income, past or current injection drug use, and enrollment in the MAT program were significantly associated with adherence in multivariable analysis.
We found that men were more likely to achieve optimal adherence than women. Gender remained a strong predictor of adherence even after adjusting for clinical and sociodemographic indicators such as age and a history of injection drug use. In the literature, a consistent relationship between gender and adherence has not been demonstrated. Some studies suggest there is no relationship between gender and adherence. 5,15,39,40 However, there is a growing body of evidence that women have poorer adherence than men. 17,24,41,42 Others have demonstrated that women are less likely to receive ART and tend to initiate HAART at a later stage of disease compared to men. 28,31,32,43 This differential access to, and utilization of, HAART is responsible for observable differences in HIV-associated mortality between men and women in some settings. 44 Previous studies comparing the predictors of adherence between men and women have found distinct differences between the 2 groups. For example, Turner et al, found that women had lower rates of pharmacy-measured adherence than men. 42 In their analysis, mental health care was associated with improved adherence in women, while substance abuse treatment was associated with improved adherence in men. The discrepancy in adherence between men and women reported here is concerning and thus further research regarding the facilitators and barriers to adherence among women is warranted. Our results suggest that gender-specific initiatives need to be evaluated as a means to support HAART adherence among HIV-positive women.
We report that both active injection drug use and having a history of injection drug use are independently associated with decreased likelihood of achieving optimal adherence to HAART. The observed relationship tended to be stronger for active drug use compared to past drug use, however, this difference was not statistically significant. Furthermore, among persons with a history of injection drug use, only 45.3% of individuals were optimally adherent to HAART. Previous studies have demonstrated that drug use is associated with poor adherence and worse virological, immunological, and clinical outcomes. 6,15 –19,35 This has led to the hesitancy among many health care providers in prescribing HAART to persons who inject drugs, given the perceived increased risk of suboptimal adherence and development of drug resistance. 12,45,46 These concerns are not, however, supported by the current evidence. For example, among those accessing HAART, a history of injection drug use is not significantly associated with decreased survival. 47 Further, it has been shown that administration of HAART to people who inject drugs is most effective when coupled with appropriate support mechanisms such as addiction counseling and methadone maintenance therapy. 48 –50 A multidisciplinary approach that integrates substance use interventions with strategies such as comprehensive case management, adherence counseling, and directly observed therapy is needed to improve clinical care for people who inject drugs.
There are some potential limitations of this study. First, measurement of adherence using prescription refill faces the same difficulty as other adherence measures in that it does not directly measure the number of pills that are actually taken. However, as discussed previously, estimates of adherence based on prescription refill compliance have been independently associated with clinical and biological end points in previous studies. 4,9 Second, the LISA cohort is a nonprobability sample, which limits the generalizability of our results. This cohort is enriched with underprivileged HIV-positive individuals, given that the small financial honorarium offered led to oversampling of individuals in need of financial gain. This represents a unique opportunity to shed some light into the challenges faced by marginalized individuals in the context of HAART expansion initiatives. Third, the LISA cohort is comprised of individuals who access a universal, publicly funded health care system where medically necessary services, including HAART, are provided free of charge. Prior to initiating treatment, all participants would have undergone an assessment by their health care provider, evaluating needs, readiness, skills, and medical and emotional resources. Thus, even the most marginalized participants in our study sample are within the reach of some medical and social services and were deemed adequately prepared to adhere to their medication regimen. However, the universal nature and the Canadian health care system gave us an opportunity to explore adherence barriers and facilitators not being clouded by the biases introduced by access to care related to income or health insurance coverage. Fourth, the association between the MAT program and adherence should be interpreted with caution, given the small sample size of MAT participants used in this analysis. Our results are, however, consistent with earlier findings and should promote further research in this area. 51 Lastly, because of the cross-sectional study design, we were unable to determine causality in adherence to HAART.
Conclusion
In the era of rapidly expanding access to HAART, an increasing number of studies are reporting promising levels of adherence. However, for a certain subset of people living with HIV/AIDS, optimal adherence continues to be difficult to achieve. In our study, we find that women and people who inject drugs are at an increased risk of suboptimal adherence. Adherence to HAART depends on the complex interaction between sociodemographic, structural, and clinical factors. Recognition of these factors is a precondition to improvements in clinical care for those not achieving optimal adherence.
Footnotes
Acknowledgments
The LISA research team is thankful for the cooperation of our various research sites. We are inspired by their amazing dedication to their clients and the communities they serve. We are also grateful for the financial support of the Canadian Institutes of Health Research (CIHR) and for the contributions of the LISA Community Advisory Committee and the study coinvestigators Dr Rolando Barrios, Dr David Burdge, Dr Marianne Harris, Dr David Henderson, Dr Thomas Kerr, Dr Julio S. G. Montaner, Dr Thomas Patterson, Dr Eric Roth, Dr Mark W. Tyndall, Dr Brian Willoughby, and Dr Evan Wood. We would especially like to thank the participants of the LISA study, who trust us with sensitive and intimate information and share their stories in hopes of supporting research projects that will make a difference in their communities. We humbly listen and interpret their experiences and hope that we are doing them justice.
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Julio Montaner has received grants from Abbott, Biolytical, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck and ViiV Healthcare. Dr Robert Hogg has received funding from GlaxoSmithKline and Merck.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Canadian Institutes of Health Research (CIHR).