
Abstract
Cerebral venous thrombosis in pregnancy in the first trimester is a very rare condition but should not be confused with the clinical presentation of other common conditions in pregnancy such as pre-eclampsia. Although it is rare and difficult to diagnose, it is potentially serious and can increase maternal mortality. Diagnosis by imaging tests such as MRI and early treatment with heparin reduces maternal and perinatal morbidity and mortality. We present the case of a 39-year-old pregnant woman at 8 weeks’ gestation who presented with early onset of severe headache and vomiting; MRI with angiography revealed a thrombosis in the right transverse venous sinus. Early treatment based on anticoagulation with heparin and maintenance with warfarin allowed a favorable response without neurological sequelae in the acute phase and at subsequent follow-up. The physiological state of hypercoagulability of pregnancy could increase the occurrence of pathologies such as cerebral venous thrombosis. We report this case as the only one published in the local literature.
Introduction
Many predisposing factors can contribute to the development of cerebral venous thrombosis (CVT), including a history of thrombosis and thrombophilia disorders. However, the most individual risk factor is pregnancy or puerperium. CVT during pregnancy is a rare and uncommon pathology, the prevalence depending on the country range from 0.49 to 1.72 per 1000 deliveries, 80% occur in the venous system and represent 10% of all maternal deaths. 1 Pregnancy is a hypercoagulable state prepared to prevent hemorrhage during the birth or a miscarriage; nevertheless, its natural condition increases the risk to thrombotic four or five times that these events appear even is higher during the puerperium.2,3 Even the mortality is low; clinically it could be confusing with other pathology prevalent in the local setting such as hypertensive disorders and its diagnostic delay could compromise maternal and fetal status. The most common clinical manifestations are severe headaches, seizures, nausea, vomiting and focal neurological deficit.4,5 Diagnosis based on neuroimaging and early treatment with anticoagulation are important to improve prognosis.
The purpose of this publication is to present a case of CVT in pregnancy. No case has been reported in the literature from Ecuador.
Case Presentation
A 39-year-old woman, mestizo, G4P2CS2M1, there was no previous record of using contraceptives or smoking, and the BMI falls within the normal range, and no history of diabetes or chronic medical conditions such as arterial hypertension or thrombotic disease. The patient was admitted to the emergency room with severe headache and vomiting for 48 hours. At the time of the event, she was 8 weeks pregnant, confirmed by eco test. The vital signs at presentation were blood pressure 110/60 mmHg, heart rate 80 bpm, respiratory rate 16 breaths/min, and oxygen saturation 94%.
The clinical characteristics of the headache are oppressive in the forehead, spreading to the orbital cavities, accompanied by nausea and vomiting, previously treated as hyperemesis and no visual symptoms. On examination there are preserved higher functions, isocoric and normally reactive pupils, normal cranial nerves without papilledema, preserved strength, tone and sensitivity, osteotendinous reflexes present. Normal finger-nose test, no dysdiadocinesia, normal tandem march and Romberg sign negative.
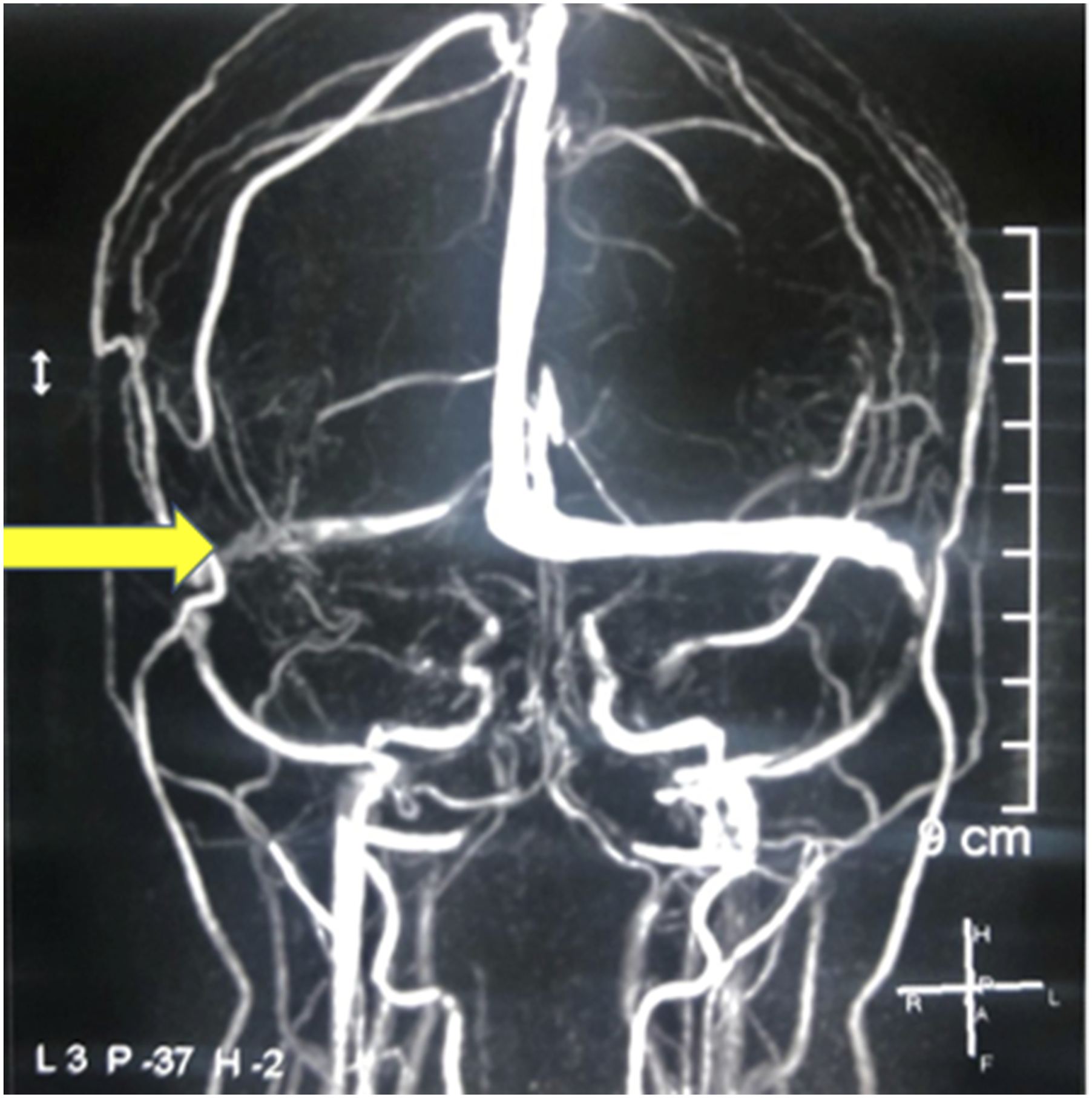
MRI of the brain shows hyperintense images with irregularities in the lumen of the right transverse venous sinus suggesting thrombosis. Angio resonance shows a correlation with the simple study in venography, there is an absence of irregular flow (Figure 1, Figure 2). (A) Reference imagen of transverse venous sinus on MRI angiography. (B) Right venous sinus thrombosis, symptoms started within 48 hours Thrombosis right sinus venous first, 5 months later the MRI shows that follow-up imaging demonstrated partial recanalization
After emergency assessment, the gynecological and neurological services start anticoagulation with sodium heparin and pain control with paracetamol. Laboratory tests were negative, including the absence of proteinuria. Hematological tests show normal values for S-protein, C-protein and other thrombotic measures; tests for antinuclear antibodies, antiphospholipid antibodies and factor Leiden mutation are negative. After five days, the headaches and vomiting resolved and her pregnancy was terminated. This decision was influenced by the early gestational age, the need for prolonged anticoagulation, and concern for potential maternal risk if neurological deterioration occurred. Termination was not performed as an emergency intervention for CVT itself, but rather as part of a shared decision-making process after counseling the patient regarding maternal risks and treatment implications.
After seven days, the patient leaves the hospital on warfarin for anticoagulation. Medical follow-up and control with MRI at 1 and 5 months show re permeabilization of the transverse sinus and no evidence of organic damage. Clinically, the patient is asymptomatic and has no neurological sequelae. Finally, estrogen-containing contraceptives were discouraged due to thrombosis risk, and alternative contraceptive methods were discussed. The patient was advised regarding recurrence risk, avoidance of additional pro-thrombotic factors, and the importance of close follow-up.
Discussion
The hypercoagulable state during pregnancy and puerperium increases the incidence of thrombosis or hemorrhagic events. The most common presentations are severe headaches, usually localized, very intense and worsening over a few days, seizures and paresis.6-8
Clinically, it is important not to confuse the symptoms of CVT with other disorders of pregnancy such as stroke, pre-eclampsia, eclampsia and others. In this case, advanced maternal age and caesarean section are the only risk factors associated with stroke in pregnancy.
Although pregnancy-associated CVT most frequently occurs in the postpartum period or late pregnancy, it is especially uncommon during the first trimester. Due to its challenging clinical diagnosis and potentially serious consequences, CVT should always be considered as a possible cause when evaluating headaches during pregnancy and the puerperium.9,10
Neuroimaging studies such as computed tomography (CT), magnetic resonance imaging (MRI) or Angio resonance are required for diagnosis and follow-up. CVT of obstetric origin generally has a good prognosis, a recovery without sequelae is observed, oral anticoagulation for at least 6 months is necessary to prevent new events. Also, there is low recurrence risk when no underlying thrombophilia is identified. In Ecuador, hypertensive disorders associated with hemorrhage and stroke are the main cause of maternal mortality and it is possible that other pathologies such as thrombotic events are underestimated.
This case contributes by documenting an unusually early (first trimester) presentation of CVT without identifiable thrombophilia, reinforcing the need to consider CVT in the differential diagnosis of severe headache even early in pregnancy.
Conclusions
Clinical suspicion and diagnosis by neuroimaging tests are essential to initiate anticoagulation treatment, which reduces maternal and perinatal morbidity and mortality.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.